Document Type : Original article
Subjects
Abstract
Background: Concerns about patient safety, resident work hour restrictions, and recent technology improvements have increased interest in surgical simulations. This study was designed to find the most effective and applicable model for total knee arthroplasty simulator.
Methods: This is a qualitative study using Focus Group Discussion (FGD) to collect data and grounded theory for analysis. A topic guide including main questions in a structured approach was used by the moderators. Three FGD sessions were held using video chat. Session’s content was recorded and extracted data was analyzed by inductive content analysis method.
Results: Eligible 5 orthopedic residents, 4 orthopedic fellowships, and 7 academic professors from referral tertiary center hospital were interviewed. The main domains of discussion were about the necessity of a Total Knee Arthroplasty (TKA) simulator, virtual vs. physical model, bone and soft tissue characteristics, and the feedback system. Twelve percent of the participants believed a virtual model has more advantages while the others thought physical model is more applicable and 12% of them suggested a mixed model. Gap balancing was noticed as a crucial part by 40% of the participants to be included in the model.
Conclusion: All the participants deemed the existence of a simulator for TKA necessary. The essential parts of the TKA simulator like foot, ankle, hip, soft tissue elements, ligaments and tendons (especially collateral ligaments) were emphasized. To improve the simulator, the participants suggested that it should have a modular design and also sensors to alarm any damage to the vital elements. Also, they pointed out having feedback option for development of TKA simulator.
Keywords: Ankle, Arthroplasty, Feedback, Fellowships and Scholar-ships, Focus groups, Grounded theory, Hip joint, Hospitals, Patient safety, Tendons
Introduction
There has been a growing interest on simulation-based learning in the surgical training curricula (1). Concerns about patient safety, resident work hour restrictions, and recent technology improvements have increased interest in laboratory-based surgical simulations (2). This way, medical students are able to make mistakes and learn from them without causing economic or health-related burden (3). Importantly, COVID-19 has affected medical care and education. The strategies to diminish interruptions for residency and fellowship training programs should be developed.
Karam et al (2) surveyed the U.S. orthopedic residency program directors and residents attitude regarding surgical skills training in a laboratory setting. Eighty percent of the program directors and 86% of the residents emphasized that surgical skills’ simulations should become main part of training, and 82% and 76% suggested a standardized surgical skill curriculum, respectively. Total Knee Arthroplasty (TKA) as multiple steps surgery, is one of the major complex procedures in the orthopedic surgical training programs. Attention to details is critical to achieve a well-balanced and functional knee following TKA and minimize the risk of complications. Creating a plan for successful biomechanical reconstruction of the knee requires knowledge of an individual patient’s anatomy including the limb alignment, ligamentous supports of the knee, skeletal anatomy along with expertise in performing precise bone cuts and soft tissue releases to achieve balanced mediolateral tension with rectangular gaps prior to component insertion. The extensive bone and cartilage removed during implantation makes the procedure practically irreversible (4).
On the way to building an effective simulator, having the future perspectives is a necessity. Similar studies, have asked orthopedic surgery residents and medical students to fill out surveys with a validated scale to rate their pre-intervention and post-intervention confidence, skill, and knowledge to assess the subjective effectiveness of the training (5-7). To authors’ knowledge, this is the first qualitative study to explore learners’ ideas about simulation-based learning, its value and the necessary characteristics of a TKA simulator.
Materials and Methods
Study design and setting: This is a qualitative study, exploring characteristics of ideal TKA simulator from the perspectives of the trainees. Focus Group Discussion (FGD), as an in-depth interview, was used to collect data. Interaction of the participants through FGD helps obtain more detailed and saturated data on the subject. Accordingly, three FGD sessions were held using a constructive paradigm. The interviews were held via video chat. This voluntary FGD study was conducted in accordance with the ethical principles of the Declaration of Helsinki and informed consent was obtained from all the participants (8,9).
Participants: Orthopedic surgery residents, fellowships, and professors from a referral tertiary center hospital, Tehran, Iran participated. The number of participants was determined once the data on the subject reached saturation. FGD sessions were held virtually and separately for each group based on their knowledge level from January 2022 till February 2022. For selecting the participants form residents, the candidates who had the knowledge of the surgery steps and experience in operating room of total knee surgery were considered. Two of the fellowships and three of the residents had experience of using virtual models. The participant characteristics are illustrated in table 1. The program participants including medical residents, fellowships and professors were invited formally through email with two reminders during a week. Finally, 16 from 28 eligible participants agreed to participate in the virtual FGD sessions. Five residents, four knee surgery fellowship trainees, and seven university professors of knee surgery were interviewed in the course of three FGD sessions. The participants were informed on the topic and main objectives of the session. Consistent with the qualitative framework, data collection and the analysis were performed concurrently.
Table1. Characteristics of the participants in the focus groups
|
Education |
Age(years) |
Gender |
|
|||||
|
Professor |
Fellowship |
Residency |
41-60 |
31-40 |
20-30 |
Female |
Male |
|
|
7 |
4 |
5 |
7 |
4 |
5 |
- |
16 |
Number |
Holding the FGDs session and data collection: During each session, a fully-trained moderator managed the session as a facilitator and would explain to the participants the ground rules of the session. The FGD sessions were conducted during approximately a month interval. The facilitator was an experienced person in qualitative health studies and particularly, leading FGD sessions.
Discussed questions were prepared before by the collaboration of experts according to the purpose of the sessions. All records of the sessions were transcript to be used in next steps.
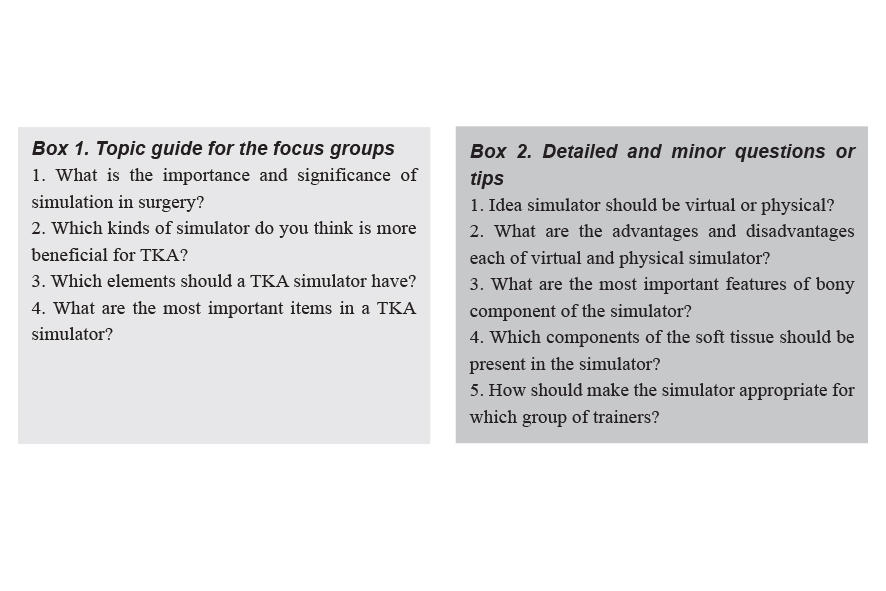
The moderator used a topic guide including lead questions in a structured approach. The questions were open ended, about the participants’ expectations for a TKA simulator and its necessary elements and items (Box 1). After each open-ended question, more limited and sometimes closed-ended questions were used to clarify the various aspects of the issue. After each answer, the moderator summarized the person’s answer and made sure that it was accurate and comprehensive. FGD sessions lasted from 60 to 75 min and an observer took notes during the interviews. The FGDs were recorded and converted to the text verbatim in addition to the observer’s field notes.
Data analysis: The current study followed a grounded theory analysis approach. Grounded theory is an analytical method mainly used in the qualitative research studies in which an inductive approach is taken in order to establish a previously unknown theory based on the participants’ ideas and opinions (10). A list of all the discussed issues is presented in table 2.
After each session, a transcribed version of recorded session and observer’s notes were used as the sources of information in the upcoming analysis phase. The analysis of the source material consisted of the following steps:
1. Two team members closely familiar with both the structure and function of the FGD and also with the nature and purpose of the study went through each transcribe individually.
2. Each transcribe was coded separately via each member. In coding, the text is read and all the parts relevant to the research questions are highlighted digitally. A different color is used for all the text relating to each individual concept or idea and that concept is given a name (e.g. a sentence describing the superiority of virtual simulators is given the code “virtual is better”).
3. A ranking system was created that divided the participants into three groups (junior resident, senior resident and fellowship were used for first- and second-year residents, third- and fourth-year residents and fellowships, respectively).
4. After the completion of the first round, the FGD transcribes were switched and each member coded the other transcribe without having any knowledge of the first coding. This step was taken as a precaution to further ensure the reliability of coding.
5. A rough classification was developed before the analysis in which different codes were classifies under different headings and sub-headings. As the next step, a table was constructed based on that classification that included the code, the rank of the speaker, and the number of times that this code was mentioned during the session and finally a selection of eye-catching sentences regarding that code.
6. The classification was refined and modified to better suit the found results.
7. All the classifications were redone by other members of the team to increase the reliability.
8. The resulting Table was distributed between all the team members and was subject to open debate until all the members contested to the completeness of the results and were satisfied with it. A detailed account of the final codes can be found in Table 2.
Table 2. Detailed list of the discussed issues during the focus group discussion sessions
|
Code |
Notable example |
Number of times mentioned and education |
Category |
Theme |
|
General questions |
||||
|
TKA is a step-by-step procedure |
- |
3 Senior residents/ 1 Fellowship |
This simulator is needed |
General opinion |
|
TKA utilizes expensive tools and devices |
- |
1 Professor/ 1 Senior resident |
||
|
A low volume of surgery is done in many educational centers |
If I was told to choose a single type of orthopedic simulator, I would definitely choose to build one for TKA or THA |
1 Senior resident |
||
|
Education in a stress-free environment |
- |
1 Senior resident/ 1 Fellowship |
This simulator is beneficial |
|
|
The procedure is repeatable |
- |
2 Professors/ 2 Senior residents |
||
|
Higher opportunity for asking questions during the operation |
- |
2 Professors/ 1 Senior resident/ 1 Fellowship |
||
|
Much lower stakes than real surgery |
A patient is supposed to live with these prosthesis for 20 to 30 years, that is too much pressure on the trainee |
1 Senior resident |
||
|
More opportunity for modifications and improvisations |
- |
1 Senior resident |
||
|
The simulator’s mere existence |
I believe that this simulator’s biggest benefit is its mere existence |
1 Senior resident |
||
|
Virtual is better |
In virtual, we can make any mistake and just undo In virtual, one can learn all different pathologies |
2 Professors/ 6 Senior residents |
Physical vs. virtual |
Model nature |
|
Physical is hard to manufacture |
Out of experience, I have never seen an actually great physical simulator. They are hard to build |
3 Senior residents |
||
|
Physical has a better feeling |
A lot of learning in orthopedics comes from the actual feel of the material and their tension This cannot be learned from a virtual simulator |
4 Senior residents |
||
|
Physical’s cost of operation and repair |
- |
2 Senior residents |
||
|
It can be mixed, best of both worlds |
- |
1 Senior resident/ 4 Fellowships |
||
|
Physical simulator specific questions |
||||
|
Simulator must include foot and ankle |
It is better if you include foot and ankle, part of the implant positioning needs them |
1 Senior resident |
Anatomy |
Bone specifications |
|
Simulator must include hip |
- |
1 Fellowship |
||
|
Distinction between cortical and cancellous bone |
Hardness of different parts of the bone should approximate the real tissue |
2 Professors/ 1 Fellowship |
Material |
|
|
Variable bone density choices |
- |
1 Professor/ 1 Fellowship |
||
|
The ability to perform site exposure |
Having the possibility to also practice limb exposure is really good |
2 Fellowships |
General opinion |
Soft tissue specifications |
|
Inclusion of vital soft tissue elements |
It is necessary to at least include the vital soft tissue elements, even as the only part of soft tissue present |
3 Professors/ 1 Fellowship |
||
|
Soft tissue simulation is hard or nearly impossible |
- |
1 Senior resident/ 1 Fellowship |
||
|
Tendon and ligament presence is crucial |
Tendon and ligament presence is crucial as feeling their tension is necessary for implant placement |
4 Professors/ 4 Senior residents/ 1 Fellowship |
Tendons and ligaments |
|
|
Ligament tension should be adjustable |
- |
3 Fellowships |
||
|
Retention of joint stability after bone cuts |
- |
1 Fellowship |
||
|
Patellar ligament |
- |
1 Fellowship |
||
|
Collateral ligaments |
- |
1 Fellowship |
||
|
ACL, PCL |
- |
1 Fellowship |
||
|
Joint capsule is needed |
- |
1 Fellowship |
||
|
Quadriceps |
- |
1 Fellowship |
Muscles |
|
|
Gastrocnemius |
- |
1 Fellowship |
||
|
Limb natural fixation points |
- |
1 Fellowship |
General opinion |
Stand specifications |
|
Gap balancing capability is crucial |
Gap balancing is the central pillar in TKA surgery |
2 Professors/ 2 Senior residents/ 4 Fellowships |
Gap balancing |
Functional specifications |
|
A physical simulator must have a modular design |
The ability to change a small compartment of the simulator and introduce a new pathology A modular design can have different difficulty levels |
3 Fellowships |
Modular design |
Others |
|
The more detailed, the better |
One can even have problems in wound closure, so the more detailed, the better |
1 Fellowship |
Simulator detail |
|
|
Added functionality questions |
||||
|
Its implementation is greatly beneficial |
It can be helpful in all the stages of the surgery. Whenever a vital element may be damaged |
2 Fellowships |
General opinion |
Sensor & feedback system specifications |
|
Saw angle detection |
Saw handling with all its details and needed skills, it would be great to have a system that can recognize weaknesses in a trainee in this skill |
2 Senior residents /2 Fellowships |
Damage sensing and prevention |
|
|
Popliteal vital elements protection |
If you could make it in a way that the saw would stop as soon as you left the green zone, that would be phenomenal |
2 Professors/ 1 Senior resident/ 3 Fellowships |
||
|
Ligament tension measurement |
You must design a bunch of sensors that can detect the tension for example on lateral ligaments |
1 Senior resident |
||
|
Gap balancing feedback |
- |
1 Professor/ 1 Senior resident |
||
|
Instant feedback |
If the trainee fails a step, the device can sound the alarm and keep them from advancing to the next step |
1 Senior resident/ 1 Fellowship |
General opinion |
Augmented reality specifications |
|
Variable difficulty by means of AR |
- |
1 Senior resident/ 1 Fellowship |
||
|
Immersive scenario |
It can have an immersive scenario, e.g., the patient may expire if you nick an artery |
1 Fellowship |
||
Results and Discussion
Importance of TKA simulator: a step-by-step procedure, cost-effectiveness
“TKA is a complicated surgery and designing a suitable simulator could help us in better training of orthopedic residents”. (Professor) “When we are doing [the procedure] on the simulator, we can develop our creativity and develop new ideas.”(PGY 3 resident). “TKA is a step- by- step procedure and also, it is device-dependent. The devices are so expensive. I wish a simulator had been available for us to use before the actual surgery.”(PGY 4 resident). Accordingly, simulators are known as cost-effective tools for training and utilizing the residents’ creativity (11,12). Among several studies comparing the effectiveness of the simulators with the traditional and cadaver trainings (11,13,14), some significant differences in the performance of residents between simulation and traditional method were found. Additionally, the simulators helped residents learn the steps of the procedures (11,14,15).
“You know that it is not possible to ask many questions during the actual surgery. We (as surgeons) might lose our concentration. By using a simulator, you can ask your questions easily and, make mistakes which are its main benefits.”(PGY4 resident). Studies on arthroscopic and virtual reality simulations reported that repeating the simulated practice in a safe environment away from stress and with immediate feedback (especially in virtual reality) causes significant improvement in the performance of the trainees (16-18). “ It can have a beginner mode for PGY1 residents which accepts 4 mm error and an expert mode which does not accept more than 2mm error [modes with different levels of accuracy].”(PGY3 resident). Furthermore, simulators have been proposed as valid and objective assessment tools to distinguish between the residents and the novice and experimented surgeons and certificate them (13,16). Besides, the level of the complexity of the simulators can alter based on the learning progress of the residents that enhances the educational quality (17).
Physical vs. virtual simulator: better tension and feeling, complexity of the design
“Physical simulators and cadaver are better options in learning this kind of surgery. According to cadaver limitations, simulators could be used widely”. (Professor) “In virtual, we can make any mistake and just undo without wasting the materials. In virtual, one can experience all different pathologies which is not possible most of the times in reality.” (PGY 4 resident). Virtual simulators provide the possibility of more manipulation such as cutting or handling and better visual experience. It can also contain more augmented components such as vessels, nerves and other components which it is difficult to be included in physical simulators (19). The best advantage of a virtual simulator is its ability to be modular, to customize different parts, rely on our needs, and to insert various bone deformities such as varus or valgus. In fact, it is possible to apply different sizes and pathologies in the virtual simulator and simulate them in different modes for the trainer to face different situations. In virtual simulators, trainer can go backwards to the previous step and correct it, while in physical simulators, a mistake cannot be easily corrected (20).
“Out of experience, I have never seen a high-quality and practical physical simulator. They are hard to build.” (PGY 3 resident). “A lot of learning in orthopedics comes from the actual feeling of the material and their tension, this cannot be learned from a virtual simulator.” (PGY1 fellow). Instant feedback also can be considered only in a physical simulator, not a virtual one. In this regard, the trainer in each step of the training can be aware of the mistakes or outcomes of that step instantly to improve or solve the problem in the moment. Physical simulator despite all these disadvantages, has an important and useful advantage. In the real model, we can feel the traction and tension more easily. In fact, the feeling of an experiment by the trainer is never comparable to a virtual simulator (21). In general, a real physical simulator can be used for the bony part of the work and a virtual component is better to use for the soft tissue part, which is more difficult to simulate (22).
Bone, soft tissue, joint, tendons and ligaments specifications
“It is better if you include foot and ankle, part of the implant positioning needs them.” (PGY1 fellow). Knee joint movements in relation to other joints like hip, ankle and foot could influence TKA surgery outcomes (23). Therefore, TKA simulator should contain mentioned parts. Kansas knee simulator as an example of constructed simulator, consists femur, patella, tibia, ankle-fixture, and hip-fixture. Interaction between ankle and ground segments is designed through sliding joints (24).
“It is important to use materials which resemble real bone characteristics, like elasticity and pressure tolerance of the bone.” (Professor) “Hardness of different parts of the bone should approximate the real tissue.” (PGY1 fellow) During total knee Arthroplasty, surgeons cut surfaces of the bone. Bone tissue structure is consisted of spongy and compact tissue with different physical characteristics (25). Different resistance of these two types of bone is felt by surgeon during operation is important to be simulated in designing a successful TKA simulator.
“It is necessary to include the vital soft tissue elements. According to text books, TKA is a soft-tissue surgery more than a bony procedure” (professor). Natural human knee consists of ligaments which constraint anterior-posterior, coronal and rotational movements. Existing studies have been conducted using spring constraints in total knee simulators (26,27). The surgeon tests function of the ligaments during balancing phase of the surgery which is of utmost importance for stability of joint post TKA. The ligaments of Kansas are modeled using elastic spring elements. The ligaments are wrapped around various geometrical shapes rather than penetrating bones (24). Syracuse knee simulator, as a hydraulic simulator, also included the quadriceps tendon and patella (28).
Augmented reality specifications
“It seems that 3D-based simulators are more effective than computer-based simulators.” (Professor) Orthopedic VR simulators are divided into three types: non-interactive simulators, interactive simulators with visual feedback, and interactive simulators with visio-haptic (tactile) feedback (29). Non-interactive simulators are mainly structured to visualize anatomy and volumetric data. The primary purpose of these simulators is help to diagnose. Non-interactive simulators help trainees to arrange surgery and predict surgical outcomes. Though these devices do not boost psychomotor skills, they may help trainees plan and anticipate events during surgery.
“If the trainee fails a step, the device can sound the alarm and keep them from advancing to the next step.” (PGY 4 resident and fellow). Instant feedback is one of the crucial features of other types of virtual reality devices. Electromagnetic sensors are applied in interactive simulators with visio-haptic feedback as an instant feedback system. These devices are defined as simulators that apply tactile feedback. The advantage of this type of simulator is that it can enhance surgeon’s competency in psychomotor skills. One of the best examples of interactive simulators with visio-haptic feedback is a novel orthopedic drilling simulator by Johns (30). This training simulator includes four main parts: a personal computer, an actual surgical drill, a synthetic proximal left femur bone model (Sawbones5 Part No. 1129), and an electromagnetic tracking system. Electromagnetic sensors are attached to the bone and drill machine to feedback the trainee instantly. Another type of simulator that applies instant feedback is interactive simulator with visual feedback. Trainees utilize a mouse, keyboard, or other optical trackers to work through these simulations. Some of these simulators are on the market as a game. For instance, Sabri et al (31) developed a game for TKA simulation. At the start of any procedure, the game asks a few questions. If the trainee chooses wrong answers or selects an incorrect instrument, then it gives feedback by an animated assistant (29).
“It can have an immersive scenario, e.g., the patient may lose the limb if you nick an artery!” (Fellow). Some virtual reality simulators use three-dimensional object texture to depict the operating theatre in order to simulate the atmosphere of surgery (32,33). It is also essential to demonstrate the consequence of any errors in the surgery. Trainees should be educated on how to control any situation that they will face during the surgery. By using virtual reality, making rare and critical conditions are available. Hence, they can also practice these situations beforehand. This approach will reduce trainees’ stress and give them more experience and confidence before encountering their fault in real surgery.
In general, ideal virtual reality simulators consist of computer platforms, video displays, and force-feedback (haptic) interfaces that simulate both knee joint and operation room atmosphere.
Limitations
During focus group discussion, it was possible that facilitators influence opinions and participant’s sight of view during FGDs in spite of training and studying guidelines beforehand. By virtual meeting, there was no social contact, and as a result, some of the participants may have not paid attention properly and participated actively. The participants were recruited from the same hospital; which limit the generalizability of the finding to the wider population.
Conclusion
This study summarized the orthopedic surgeons’ and trainees’ opinions about an applicable TKA simulator. The main themes of the discussions were general opinions regarding the necessity of a TKA simulator, virtual vs. physical model, hard and soft tissue characteristics, and feedback system. All the participants deemed the existence of a simulator for TKA necessary. Results for choosing virtual model versus physical model were discussed. The essential parts of the TKA simulator like presence of foot, ankle and hip in the model and inclusion of vital soft tissue elements and ligaments and tendons (especially collateral ligaments) were addressed. Gap balancing was noticed as a crucial part of procedure by senior residents and fellowships. To improve the simulator, the participants suggested that it should have a modular design and also sensors to alarm any damage to the vital elements. Also, they pointed out having feedback option for development of TKA simulator.
Consent to participate
All the participants gave oral and written consent for using their discussions in focus groups in this study.
Funding
No funding was received.
Acknowledgement
The ethical code number is IR.TUMS.SINAHOSPITAL.REC.1399.050 from Tehran University of Medical Sciences.
Conflict of Interest
There was no conflict of interest in this manuscript.