Document Type : Original article
Subjects
Abstract
Background: To have an efective patient education material, health professionals need a comprehensive tool to evaluate these materials. The Evaluation of the Patient Education Information Materials scale (PERSI-PEIMET) evaluates patient education materials and enables nurses and healthcare professional to assess and optimize the Patient Education Information Material (PEIM) according to scientific criteria. This paper describes the development and psychometric testing of PERSI- PEIMET.
Methods: The psychometric properties of PERSI-PEIMET (with 42 items) including face, content, and construct validity and reliability were done. Exploratory factor analysis was used in order to evaluate construct validity and 527 experts in Medical library and information sciences, nursing education and clinical experts who were faculty member in Tehran, Iran, Tabriz, Boushehr, Isfahan, Zahedan and Ahvaz medical universities, were recruited randomly.
Results: Exploratory factor analysis identified 10 factors including readability, design, structure, coherence, suitability, appropriateness, actionabiity, quality, formatting and reliability that together accounted for 83.92% of the total variance of the factors. The Cronbach’s alpha of these ten factors and the total scale were 0.922, 0.917, 0.836, 0.831, 0.816, 0.717, 0.749, 0.781, 0.737 and 0.951, respectively. The intra-class correlation coefficient based on test-retest was 0.85 which showed entire scale reliability is high.
Conclusion: The PERSI- PEIMET appears to have acceptable validity and reliability and it is considered as a good instrument for evaluatin PEIM. PERSI_PEIMET comprehensively evaluates all the characteristics and variables affecting the efficiency of PEIMs. Instrument development is an iterative process and further testing with other cohorts and in other settings is required.
Keywords: Comprehension, Education, Factor Analysis, Statistical, Faculty, Information Science, Iran, Psychometrics, Reproducibility of results, Nursing, Universities
Introduction
Changes in health systems and the patient’s tendency to participate in treatment decisions-making have increased the need for patient education (1). Patient education is one of the basic rights of the patient and their family/relatives and caregivers (2). The purpose of patient education is protection of the patient from complications related to their disease and other health problems that may accrue to their disease. Also, patient education changes the patient’s awareness, attitude, and skill, and increases the patient’s competence and ability to take care of himself, and makes him perform activities that increase the level of health and well-being of the patient’s behavior and prevent the occurrence of potential complications (3). Patient education reduce the cost of health care, increase the quality of life, and help the patient become physically, psychologically, and socially self-sufficient as soon as possible (4). A 2022 patient survey by Tebra found that 68% of the patients who receive patient education are more likely to return to a healthcare provider. A recent pilot shows patients who were armed with information before they underwent a procedure were 11% more knowledgeable about it (5). This highlights how patient education fosters trust and loyalty, improving patient-provider relationships and encouraging follow-up care, which can enhance long-term health outcomes. A meta-analysis of studies on discharge education using the teach-back method for heart failure patients showed that this approach significantly reduced overall readmission rates, with an odds ratio of 0.40 (95% confidence interval: 0.17–0.94), indicating a substantial decrease in the likelihood of readmission compared to standard care (6). In a randomized controlled trial involving rheumatoid arthritis patients, those who received needs-based education guided by the Educational Needs Assessment Tool (ENAT) indicated statistically significant improvements in self-efficacy, as measured by the Arthritis Self-Efficacy Scale (ASES), with notable gains in managing pain and other symptoms over a 32-week period (7). Research cited in conference proceedings from 2019 indicated that interactive health education sessions increased behavior change adoption by 40%, suggesting that engaging educational methods can effectively motivate patients (8) to adopt healthier practices. Studies on diabetes self-management education have shown mixed but promising results, with some reviews reporting improvements in glucose control and quality of life. For instance, randomized controlled trials have demonstrated reductions in diabetes incidence by up to 58% in high-risk populations through structured lifestyle interventions supported by education (9).
Patient education is an important responsibility and function of nurses, because nurses are in close and constant contact with patients. Raising patients’ awareness of prescription drugs, drug interactions, diet, signs and symptoms that patients should inform their caregivers, and many other activities are nurses’ duties (10). One of the most effective ways to provide a patient education program is to provide Patient Education Information Materials (PEIM) in the form of brochures, pamphlets, and training booklets, so, nurses in their role as patient educators, are expected to provide or evaluate these resources and to provide them to the patient.
Written PEIM are economical than other types of patient education resources such as video patient education, reinforce oral instruction and are preferred form of education by most patients. These materials are provided to increase awareness, sensitization, and practical reminders, improve physician-patient relationship, and promote patients’ health literacy. In order to achieve these goals, health information must be provided in the format that can increase patents’ knowledge, skills and behaviors. If the information in these sources is incomplete, inaccurate, out of date, contained too much information and uncommon words, it will be more dangerous than beneficial to the patient. Incomplete and incorrect information can negatively affect the medical-patient relationship and cause anger and stress in patients and their families (10).
Although, given the above, it is important to evaluate these resources, nowadays the necessity of producing PEIM often takes precedence over quality assessment of resources. In therapeutic settings, instead of evaluating and measuring the characteristics of PEIM, the main focus is on providing these resources (11,12). Research has shown that although efforts have been made to develop a tool for evaluating PEIM, each of these tools addresses only part of the criteria for standardization of resources such as readability, information quality, complexity, and usability (13-18). Some existing tools for evaluating PEIM, such as DISCERN and PEMAT, focus on specific aspects like readability and actionability but lack comprehensive evaluation criteria.
However, in evaluating an information source, in addition to evaluating the content other characteristics such as structural characteristics should be considered.
Review of previous research has shown that not only is there currently no complete tool that comprehensively evaluates all the indicators affecting the efficiency of a PEIM, but also there exists no tool that is simple enough for individuals to evaluate the PEIM. Since one of the responsibilities of medical librarian is to identify and support patients’ information needs, create, locate and evaluate health information or PEIM, as well as serve as a quality filter for health information or PEIM in accordance with the American Medical Library Association’s policy (19,20), therefore, the authors, in order to have a comprehensive vision for the production of tools, conducted this research with a team of medical librarians and nurses. Clinical medical experts conducted the present study to develop and determine psychometric properties of Evaluation of the Patient Education Information Materials scale (PERSI-PEIMET): a tool with high comprehensibility and simplicity to evaluate written PEIM which assist healthcare professionals to evaluate and select the most appropriate written PEIM for clients.
Materials and Methods
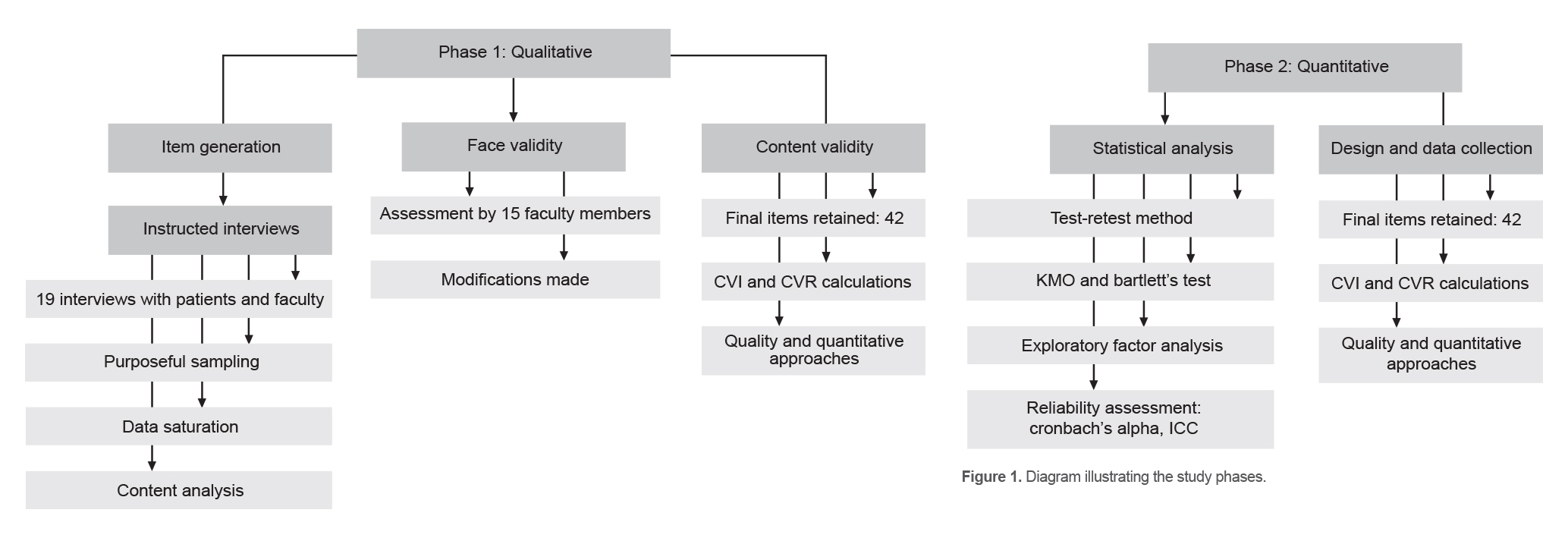
This study which is a part of a parent projects as a PhD dissertation and some parts of that is published as an article (21), had two phases, one of which was qualitative (this phase was done to generate the scale), while the other was quantitative.
Descriptions of these are provided as follows:
Phase 1
Item generation
Two stages were done to obtain criteria that should be considered in preparing or evaluating a PEIM.
1. Using a qualitative approach, 19 instructed interviews were conducted with four patients referring to Namazi Hospital in Shiraz and 15 faculty members of Medical Librarianship and Information, Nursing and Clinical Medical from Bushehr, Isfahan, Kerman and Tabriz medical universities during April 2020 to February 2021. The participants were selected using purposeful sampling. The inclusion criterion in the study was the work experience in the clinical environment and work experience about patient education, having special knowledge or experience in preparing or evaluating PEIM, using PEIM, ability to express their experiences and their willingness to cooperate in the study. The exclusion criterion in the study was the refusal of people to continue participating in the research. There were two categories of question, one for patients and one for faculty members.
During the interviews, the participants (if were faculty members) were asked about their experiences in preparing or evaluating a PEIM, participate in academic course or workshop about patient education and if they were patients, they were asked about their experiences in using a PEIM. Sampling continued until no further new data emerged, indicating that the data saturation point was reached. The duration of each interview varied from 20 t0 30 minutes. All the interviews were digitally recorded having obtained the permission of the participants. After completing each interview, it was listened to carefully several times and transcribed word by word. The data was explored using content analysis.
2. A systematic review was conducted to extract the considered criteria in evaluating or preparing a PEIM. According to this systematic review, 24 criteria were identified (16).
Based on the analysis of interviews and results of systematic review, an initial pool of 143 items was generated. After a careful review of the items by the research team, items that were similar and overlapped were merged or removed, and thus, in the first stage, the items were reduced to 45. The scale was then scrutinized for its face and content validity.
Face validity
The qualitative ways were used to determine the face validity of the scale. In order to determine the qualitative face validity, 15 faculty members in Medical Library and Information Sciences, Nursing, Clinical Medical experts and two editors of Farsi Language from Ahvaz, Bushehr, Isfahan, Kerman and Tehran medical universities, were recruited using convenience sampling to determine the ambiguity, relevance and difficulty of each item. No additional item for evaluating was identified by the expert for inclusion in the scale.
Content validity
The content validity of the scale was carried out using qualitative and quantitative approaches. For the qualitative evaluation of content validity, factors such as grammar, appropriate wording and item allocation were assessed.
The quantitative content validity, both the Content Validity Index (CVI) and Content Validity Ratio (CVR) were calculated. To evaluate the CVR, the opinion of 11 specialists in Medical Library and Information Sciences, Nursing and Clinical Medical, who were faculty member in Ahvaz, Busher, Isfahan, Kerman and Tehran medical university, were asked to assess each item on a 3-point Likert scale (where 1=essential, 2=useful but not essential, 3=not essential).
The Lawshe’s Table (13), was used to decide on CVR and the items whose CVR was equals to or greater than 0.62 were retained. Items that scored greater than or equal to 0.62 were kept in the scale. Throughout this phase, 3 items were removed. In order to calculate the CVI, these expert panelists were asked to determine the relevance, clarity, and simplicity of each item using a 4-point Likert scale. However, in accordance with Waltz and Baussel (22), items with CVI value greater than or equal to 0.78 were accepted and three items that did not meet the criterion were removed. 42 items had a CVI value of greater than or equal to 0.79. Also, based on the average scores of the content validity index of all the items (I-CVI), the average content validity index of the questionnaire (S-CVI/Ave) was calculated as 0.95.
Following the face and content validity checks, the pre-final version of the instrument had 42 items which rated on a five-point Likert scale from 0 (not applicable in this material) to 4 (met all of the time). The scores for all the items were summed, with a possible range from of 0 to 168, which higher scores indicating the more criteria the patient education information resource meets. To interpret these scores, they were divided into four quartiles, thus scores between 0 and 42 were classified as poor, scores from 43 to 84 as poor, scores from 85 to 126 as good, and scores from 127 to 168 as excellent.
Phase 2
Design and data collection
Psychometric analysis of the scale was performed by a cross-sectional study with a sample of experts in Medical Library and Information Sciences, Nursing and Clinical Medical who were faculty members in medical universities in Tehran, Iran, Tabriz, Bushehr, Isfahan, Zahedan and Ahvaz medical universities. Since a part of the sample was faculty members of Medical Librarian and Information Sciences, the mentioned universities were selected due to having this major. The participants were recruited using a random sampling method. For sampling, in the selected universities, experts in mentioned field were identified and then randomly selected. It was estimated that a sample of 420 faculty members would be enough for this study (10 individuals per item of the questionnaire). However, 600 individuals of seven universities were selected and finally 527 questionnaires were returned.
The study objectives were explained to the participants, and after obtaining the informed consent, the scale and three patient information education which were selected randomly among PEIM which were prepared by Isfahan university of Medical Science was sent to them by email in order to evaluate these PEIM according to the scale.
Statistical analysis
The adequacy of the tool in measuring existing structures was considered in the construct validity. To determine the construct validity, exploratory factor analysis with Equamax rotation were used in SPSS 24 (IBM Corp, Armonk, NY, USA). In the exploratory factor analysis, the Keiser-Mayer-Olkin (KMO) sampling index and Bartlett’s Test of Sphericity were evaluated. The value of 0.4 was considered the minimum load factor and eigenvalue greater than one. To determine the reliability, the Cronbach’s alpha coefficient and Intraclass Correlation Coefficient (ICC) were calculated. Both of these coefficients are acceptable with values of higher than 0.6 (23). Moreover, using test-retest method, the questionnaires were completed by 30 faculty members within an interval of 2 weeks. The steps of conducting the study are shown diagrammatically in figure 1.
Results
In this section, the results of each phase have been shown separately.
Phase 1.
Face validity
In this stage which scale validity was reviewed by Face validity, no additional item for evaluating was identified by the expert for inclusion in the scale.
Content validity: In this stage, three item were removed and 42 items had a CVI value of greater than or equal to 0.79. Also, based on the average scores of the content validity index of all items (I-CVI), the average content validity index of the questionnaire (S-CVI/Ave) was calculated as 0.95.
Phase 2.
Construct validity
The mean (SD) age of the faculty members was 41.7 (7.4; minimum 25, maximum 58), 49.7% were female and the rest were male. In terms of academic ranks, 13.1% had MSc degree and were lecturer, 47.2% were assistant professor, 28.8 % were associate professor and 10.8% were professor (Table 1).
The instrument construct validity was determined in this study through via exploratory factor analysis with Equamax rotation. The Kaiser-Meyer-Olkin (KMO) sample adequacy test statistic was calculated as 0.624 (Table 2) which indicates the suitability of sample size for conducting the factor analysis (24).
The acceptable level for the scale items was adjusted to be higher than 0.40. As there was no item with a factor load of <0.40 in the first iteration, the 42-item draft scale structure was protected. The Bartlett Test of Sphericity was <0.05 which indicates it is appropriate for factor analysis in order to identify the structure of the factor model.
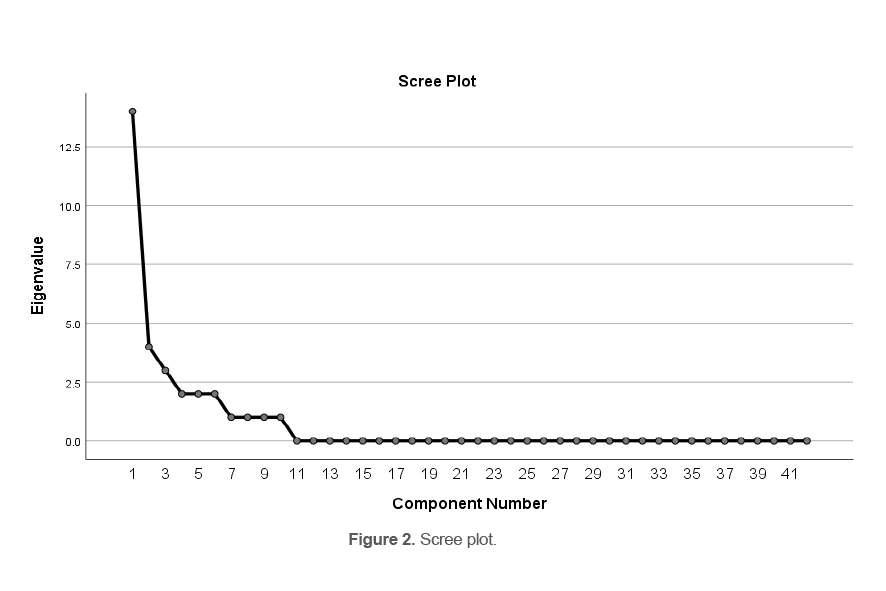
In the exploratory factor analysis, it was found that the 42 items in the draft scale were divided into ten factors that explained 83% of the total variance as shown in table 3.
Scree plot which can be seen in figure 2, shows that ten factors have a specific value greater than one, therefore 10 factors were considered for the scale.
Table 3 shows the extracted factors along with the specific value, the percentage of variance and the cumulative variance explained by each of these factors.
Table 4 shows the factor matrix after Equamax rotation. In table 4, the factor loads of each item of the PERSI- PEIMET on the ten extracted components are specified. Factor loads of about 0.40 and above were considered to assign each question to a component. The items that were common in more than one factor were considered among the ten main factors due to the higher factor load, conceptual fit, the nature of the item and the results of the qualitative stage in one factor. Therefore, item number six and seven were considered in the third factor.
In the ten-factor structure formed after the exploratory factor analysis, item analysis and Cronbach’s alpha internal consistency analysis was used to assess the item total score correlations in the factors and the internal consistencies of the obtained measurements.
The acceptable value for the internal consistency of the scale was determined as 0.70. The internal consistency analysis revealed that the sub factor and general scale item total correlation coefficients and the Cronbach’s alpha coefficient values were high. The Cronbach’s alpha coefficient of the scale was 0.94. Table 5 shows the Cronbach’s alpha coefficient for each factor.
Table 1. Demographic information
|
Variables |
Frequency |
Percent |
|
|
Universities |
Ahvaz |
78 |
14.8 |
|
Bushehr |
61 |
11.6 |
|
|
Iran |
75 |
14.2 |
|
|
Isfahan |
22 |
4.2 |
|
|
Kerman |
72 |
13.7 |
|
|
Tabriz |
57 |
10.8 |
|
|
Tehran |
110 |
20.9 |
|
|
Zahedan |
52 |
9.9 |
|
|
Degree |
MSc |
69 |
13.1 |
|
PhD |
256 |
48.6 |
|
|
Resident |
202 |
38.3 |
|
|
Sex |
Female |
262 |
49.7 |
|
Male |
265 |
50.3 |
|
|
Rank |
Lecturer |
69 |
13.1 |
|
Assistant professor |
249 |
47.2 |
|
|
Associated |
152 |
28.8 |
|
|
Professor |
57 |
10.8 |
|
Table 2. KMO and Bartlett’s Test
|
p-value |
Df. |
KMO |
Chi-square |
|
<0.001 |
861 |
0.624 |
41677.123 |
Table 3. Eigen value and percentage of total variance determined for 10 questionnaire factors
|
Component |
Initial eigenvalues |
Rotation sums of squared loadings |
||||
|
Total |
%of Variance |
Cumulative% |
Total |
%of Variance |
Cumulative% |
|
|
1 |
14.579 |
34.712 |
34.712 |
4.236 |
10.086 |
10.086 |
|
2 |
4.079 |
9.712 |
44.424 |
4.119 |
9.808 |
19.893 |
|
3 |
3.397 |
8.088 |
52.512 |
3.539 |
8.427 |
28.320 |
|
4 |
2.884 |
6.867 |
59.379 |
3.495 |
8.322 |
36.642 |
|
5 |
2.520 |
6.000 |
65.379 |
3.447 |
8.208 |
44.850 |
|
6 |
2.227 |
5.302 |
70.681 |
3.374 |
8.033 |
52.883 |
|
7 |
1.710 |
4.072 |
74.753 |
3.308 |
7.877 |
60.760 |
|
8 |
1.438 |
3.423 |
78.176 |
3.259 |
7.759 |
68.519 |
|
9 |
1.355 |
3.227 |
81.403 |
3.239 |
7.712 |
76.231 |
|
10 |
1.059 |
2.521 |
83.924 |
3.231 |
7.693 |
83.924 |
Table 4. Factor matrix after equamax rotation
|
Items number |
Factors |
|||||||||
|
|
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
|
2 |
0.725 |
|
|
|
|
|
|
|
|
|
|
8 |
0.722 |
|
|
|
|
|
|
|
|
|
|
9 |
0.668 |
|
|
|
|
|
|
|
|
|
|
11 |
0.632 |
|
|
|
|
|
|
|
|
|
|
19 |
0.536 |
|
|
|
|
|
|
|
|
|
|
20 |
0.534 |
|
|
|
|
|
|
|
|
|
|
22 |
0.511 |
|
|
|
|
|
|
|
|
|
|
28 |
0.503 |
|
|
|
|
|
|
|
|
|
|
31 |
0.464 |
|
|
|
|
|
|
|
|
|
|
12 |
|
0.854 |
|
|
|
|
|
|
|
|
|
13 |
|
0.796 |
|
|
|
|
|
|
|
|
|
14 |
|
0.785 |
|
|
|
|
|
|
|
|
|
15 |
|
0.782 |
|
|
|
|
|
|
|
|
|
16 |
|
|
0.785 |
|
|
|
|
|
|
|
|
5 |
|
|
0.651 |
|
|
|
|
|
|
|
|
17 |
|
|
0.598 |
|
|
|
|
|
|
|
|
6 |
|
|
0.539 |
|
0.413 |
|
|
|
|
|
|
7 |
|
|
0.530 |
|
|
|
0.459 |
|
|
|
|
10 |
|
|
|
0.847 |
|
|
|
|
|
|
|
18 |
|
|
|
0.649 |
|
|
|
|
|
|
|
24 |
|
|
|
0.613 |
|
|
|
|
|
|
|
25 |
|
|
|
0.542 |
|
|
|
|
|
|
|
27 |
|
|
|
|
0.852 |
|
|
|
|
|
|
32 |
|
|
|
|
0.779 |
|
|
|
|
|
|
4 |
|
|
|
|
0.466 |
|
|
|
|
|
|
16 |
|
|
|
|
|
0.881 |
|
|
|
|
|
26 |
|
|
|
|
|
0.685 |
|
|
|
|
|
21 |
|
|
|
|
|
0.579 |
|
|
|
|
|
36 |
|
|
|
|
|
|
0.830 |
|
|
|
|
38 |
|
|
|
|
|
|
0.487 |
|
|
|
|
39 |
|
|
|
|
|
|
0.446 |
|
|
|
|
33 |
|
|
|
|
|
|
|
0.781 |
|
|
|
34 |
|
|
|
|
|
|
|
0.719 |
|
|
|
35 |
|
|
|
|
|
|
|
0.685 |
|
|
|
37 |
|
|
|
|
|
|
|
0.661 |
|
|
|
1 |
|
|
|
|
|
|
|
|
0.904 |
|
|
23 |
|
|
|
|
|
|
|
|
0.509 |
|
|
29 |
|
|
|
|
|
|
|
|
0.484 |
|
|
30 |
|
|
|
|
|
|
|
|
0.485 |
|
|
40 |
|
|
|
|
|
|
|
|
|
0.942 |
|
41 |
|
|
|
|
|
|
|
|
|
0.939 |
|
42 |
|
|
|
|
|
|
|
|
|
0.919 |
Table 5. Cronbach’s alpha coefficient and Intraclass Correlation Coefficient (ICC)
|
Factors |
Number of items |
Items |
Cronbach’s alpha |
ICC |
|
Readability |
9 |
3-8-9-11-19-20-22-28-31 |
0.922 |
0.770 |
|
Design |
4 |
12-13-14-15 |
0.917 |
0.752 |
|
Structure |
3 |
4-5-17 |
0.836 |
0.778 |
|
Coherence |
4 |
36-38-39-32 |
0.831 |
0.782 |
|
Suitability |
4 |
6-7-10-18 |
0.816 |
0.723 |
|
Appropriateness |
3 |
1-2-26 |
0.717 |
0.755 |
|
Actionability |
4 |
21-24-25-27 |
0.749 |
0.771 |
|
Reliability |
4 |
33-34-35-37 |
0.781 |
0.687 |
|
Formatting |
4 |
16-29-30-23 |
0.737 |
0.748 |
|
Quality |
3 |
40-41-42 |
0.951 |
0.682 |
|
Total |
42 |
|
0.942 |
0.851 |
According to the results presented in table 5, Cronbach’s alpha Coefficient was 0.942 for the total scale. The ICC for the total scale was 0.851 (95% CI: 0.771-0.950).
Discussion
Since review of literature revealed no comprehensive tool for evaluating PEIM, Thus, the purpose of this study was to develop and investigate the reliability and expletory factor analysis of PERSI- PEIMET. The PERSI- PEIMET with 42 items were developed based on the experiences of faculty members in medical library and information Sciences, nursing, clinical medical faculty members and patients in preparing, evaluating or using a PEIM as well as the literature review. The items of this tool were categorized into 10 dimensions: readability, design, structure, coherence, suitability, appropriateness, actionability, quality, formatting and reliability. The Persian and English version of the tool are available in the appendix 1.
The readability dimension, with the largest number of items (9 items), had the highest percentage of total variance compared to other dimensions. The high variance of this dimension shows that the items that make up this dimension play an important role in evaluating the PEIM. This factor, which focuses on the clarity and readability of a PEIM for the audience, is in line with the findings of Doak, Doak and Root, who believed that a PEIM should use common words, avoid the use of specialized words, and sentences should be written in an active voice or colloquial style (25-27). In line with the current research in the field of attention to this factor, two PEIM assessment tools with 26 items and a health information rating form with five items measure the ability to understand and have paid attention to factors such as word choice, writing style and content (28,29).
The design dimension, with 4 items, focuses on the type of arrangement of text and images, the amount of empty space in the text, and the distance between lines, and is consistent with the findings of the Doak, Doak and Root, Tong et al and Grase et al (38-40). Medication information design assessment scale (MIDAS) with 13 items that measures the quality of the written information design of a PEIM showed the importance and attention of previous researchers to this dimension. Of course, this tool has only evaluated construct validity (28). Also, six items out of 17 items of the Consumer Information Rating Form (CIRF) assessed the quality of the design of a PEIM from the perspective of the audience of the mentioned materials (28).
The structure dimension has 3 items. This dimension emphasizes the size of a PEIM and its binding type, and in cases where the educational source is electronic, it emphasizes the logical architecture of the website and the ease of navigation on the page, is aligned with the results of Maron’s research, which developed the BIDS tool and Clayton, which used the TEMPTED tool developed (11,30) .
The coherence dimension has 4 items. This dimension, which refers to the coherence of sentences with each other and with adjacent sentences and how to use the conjunctions and relative adjectives, was not considered in any of the existing tools and also had little researches. Among the studies that considered the coherence criterion were Carinci et al and Smith et al (31,32).
The appropriateness dimension has 4 items. This aspect of the questionnaire, which refers to what extent the content of a PEIM matches the opinions, beliefs and standards of the audience., was considered a subset of suitability in the researches of clayton and maren (11,30).
The suitability dimension has 3 items. In the present study, this dimension highlights more how much educational resource content is interactive and how much it motivates the audience and acts as a stimulus for the readers to actively participate in the text. In the Clayton and Doak, and Root, motivation was also considered as one of the subsets of suitability, and therefore this part is consistent with the researches of the researchers (11,38).
The actionability dimension, which has 4 items, is consistent with the findings of Holt’s research. Hewlett found that audiences understood drug dosage instructions more easily when the hour of administration was specified in the dosage section rather than when abbreviations were used (34).
The quality dimension has 4 items. This dimension, which refers to the transparency of the source preparation time and the use of the latest scientific evidence, has been confirmed by other researches, and these researches have paid attention to these issues in evaluating the quality of information sources (35). In the previous studies, it was reported that the quality of information sources was evaluated with a tool called DISCERN with 16 items, which is in line with the present study and demonstrates the importance of paying attention to quality dimension. Although, unlike the current research, only the face and content validity of this tool has been done. This tool has also been used in many studies to evaluate the quality of a PEIM (36).
Formatting dimension has 4 items and refers to the way of arranging the text, using images and diagrams to simplify the content, and it has been confirmed in other researches. However, in Clayton and Dauk, Dauk and Root, this dimension was considered a subset of suitability and has not been considered as a separate dimension (38).
The reliability dimension with three items is based on the trustworthiness and honesty of the PEIM and it refers to the extent to which the source has provided information without prejudice and bias. It is considered in other researches and is consistent with them (35,37).
In this study, in evaluating the internal consistency, the Cronbach’s alpha coefficient was calculated and the results showed that all the dimensions as well as the whole instrument have high reliability. The acceptable reliability for the questionnaire by Cronbach’s alpha coefficient indicated that the measuring instrument had the acceptable accuracy and that in similar condition the same and reliable results can be expected. In this research, in the test-retest method, the questionnaire was performed in a short time interval (2 weeks) under the same conditions and on a group of faculty members and the results of implementation of a questionnaire were confirmed to be stable over time.
Unlike DISCERN and PEMAT, the items of the Persi-PEIMET do not cover a special area of PIM effectiveness criteria. They considered content-related, structural and graphical requirements, whereas DISCERN focuses on reliability and completeness of information, and PEMAT on understandability and actionability. The PERSI-PEIMET addresses a critical gap in the evaluation of patient education materials by providing a comprehensive and user-friendly tool. Its practical applications include improving the quality of PEIM, enhancing patient understanding, and supporting healthcare providers in selecting appropriate resources. One of the strengths of the study was that items of questionnaire were based on a qualitative study and experiences of experts and patients in preparing, evaluating and using a PEIM as well as a scoping review. However, this study has limitations, including the sampling of the participants from a single country, which may limit the generalizability of the findings. Future research should explore the tool’s applicability in diverse cultural and linguistic contexts, as well as its use in digital health education platforms. Another limitation of the present study was that convergent and divergent validity were not conducted. Given the developmental nature of this research, it is suggested that other psychometric indicators such as convergent and divergent validity be conducted in future studies.
Innovation
The innovation of Persi- PEIMET relies on its comprehensiveness and simplicity. Persi- PEIMET comprehensively evaluates all the characteristics and variables affecting a patient education information material, and it is no longer necessary to measure a patient education resource by different tools in order to evaluate different criteria. In addition to being comprehensive, Persi- PEIMET is also easy to use, and even in addition to nurses and patient education professionals, patients themselves can use it to evaluate a patient education material.
Conclusion
The finding of the study indicated the appropriate validity and reliability of the scale’s factors related to evaluating a PEIM. For health professionals who develop their own PEIMs, Persi- PEIMET serves as a comprehensive standard for creating a high-quality product. Also, to select an appropriate written PEIM for the patients, nurses and other healthcare professionals that need a valid and reliable evaluation mechanism, Persi- PEIMET is an efficient guide to evaluate materials. It overcomes the limitations of previously developed instruments and was found to be easy to use, able to be completed in less than 15 min, and giving a comprehensive review of the educational material.
The PERSI-PEIMET is a valid and reliable tool for evaluating patient education materials, offering a comprehensive and user-friendly approach. Its development addresses a significant gap in the field, providing healthcare professionals with a scientifically grounded tool to optimize patient education.
Further research needs to be conducted and other members of the healthcare professions need to evaluate its validity and reliability, including its use internationally. Also, future research should focus on validating the tool in diverse populations and exploring its use in digital health education. These efforts will further enhance the tool’s applicability and impact patient care.
Practice implications
With the Persi- PEIMET, a PEIM evaluation tool has become globally available, which appeared to be reliable and valid. It is aimed to support all groups involved in the development, optimization or evaluation of PEIM, i.e., nurses, and healthcare professionals, research and policy.
Funding
This work was supported by Isfahan University of Medical Sciences with project number 398308.
Acknowledgement
The authors would like to thank all the participating faculty members and patients who helped the researchers carry out this study. They confirm that all the methods were performed in accordance with the guidelines and regulations of the Isfahan University of Medical Sciences Research Ethics Committee approval reference number IR.MUI.RESEARCH.REC.1398.309.
Conflict of Interest
There was no conflict of interest in this manuscript.
Patient Education Information Materials Evaluation tool (Persi- PEIMET) are presented here in the format of a rating scale to facilitate your rating of the PEIM. Read the patient education material and use Persi- PEIMET to determine if this resource meets the affecting criteria on efficacy of a patient education resource. Each of these criteria is expressed as phrases, and the score of each phrase is a number between one and five, which is as follows:
The scale:
0 = Not applicable (Na)
1= Not met
2 = Met some of the ime
3 = Met most of the ime
4 = Met all of the im
Appendix 1. English version of persi- PEIMET
|
Dimensions |
|
Items |
0 Does not apply to this resource 1 Does not apply at all 2 Slightly applies 3 Largely applies 5 Completely applies |
||||
|
Readability |
1 |
Drawings/illustrations are recognizable to the target group with or without explanatory text |
|
|
|
|
|
|
2 |
The PEIM emphasized the important points |
|
|
|
|
|
|
|
3 |
The PEIM displays information in the form of charts or images when needed |
|
|
|
|
|
|
|
4 |
A PEIM contains concise and coherent summaries of the messages to be conveyed |
|
|
|
|
|
|
|
5 |
Necessary health terms are defined |
|
|
|
|
|
|
|
6 |
Ambiguous and unfamiliar words are not used for the audience |
|
|
|
|
|
|
|
7 |
Visual assistants have been used to simplify the instructions |
|
|
|
|
|
|
|
8 |
The information load of the material (amount+novelty/obscurity of information) is appropriate for the target group |
|
|
|
|
|
|
|
9 |
The most important information is highlighted in bold |
|
|
|
|
|
|
|
Design |
10 |
The distance between the lines is such that it is easy to read the content |
|
|
|
|
|
|
11 |
The type of font is such that it is easy for the audience to read the content |
|
|
|
|
|
|
|
12 |
The font size is such that it makes it easy for the audience to read. |
|
|
|
|
|
|
|
13 |
Distances and arrangement of text and images are eye-catching for the viewer |
|
|
|
|
|
|
|
Structure |
14 |
The source has used visual aids (such as bolder font, highlighting, arrows, framing, etc.) |
|
|
|
|
|
|
15 |
Color is used as a cueing agent to highlight material and promote learning |
|
|
|
|
|
|
|
16 |
Important information is organized as lists and categories |
|
|
|
|
|
|
|
Coherence |
17 |
The ideas presented in the PEIM are logically related and present a coherent structure for the information being conveyed |
|
|
|
|
|
|
18 |
The information flows in a natural sequence from the general to the specific |
|
|
|
|
|
|
|
19 |
The material moves from simpler to more complex content in a manner that is logical |
|
|
|
|
|
|
|
20 |
The PEIM does not contain information or content that would cause a deviation from the objective |
|
|
|
|
|
|
|
Suitability |
21 |
The recommendations provided are appropriate to the beliefs, values and culture of the target audience of PEIM |
|
|
|
|
|
|
22 |
The PEIM is appropriate to community standards |
|
|
|
|
|
|
|
23 |
The examples used in the PEIM contain the central characteristics of the ideas and concepts under discussion |
|
|
|
|
|
|
|
24 |
The content is respectful of the customs and traditions of the target group. |
|
|
|
|
|
|
|
Appro -priateness |
25 |
Questions are posed throughout the PEM to encourage the readers to engage |
|
|
|
|
|
|
26 |
The title of a PEIM conveys the purpose of the resource |
|
|
|
|
|
|
|
27 |
Educational content covers learning objectives |
|
|
|
|
|
|
|
Actionability |
28 |
In self-care activities, the steps are explained with examples |
|
|
|
|
|
|
29 |
The PEIM describes how each treatment works |
|
|
|
|
|
|
|
30 |
The content focuses on what the target group should do as well as what they need to know |
|
|
|
|
|
|
|
31 |
Audiences can easily find what they need in the information source |
|
|
|
|
|
|
|
Reliability |
32 |
It is clear what information sources have been used to collect information |
|
|
|
|
|
|
33 |
The production time of the PEIM is known |
|
|
|
|
|
|
|
34 |
In preparing the PEIM, the latest sources and reliable scientific evidence have been used |
|
|
|
|
|
|
|
35 |
The PEIM provides details such as sponsoring organizations or websites for more audience information |
|
|
|
|
|
|
|
Formatting |
36 |
The PEIM uses clear and simple visual elements |
|
|
|
|
|
|
37 |
Images and diagrams have been used to simplify the content |
|
|
|
|
|
|
|
38 |
The size of the PEIM is one that is easily handled by the target group (5x8 is easy to handle, 8x11 is easy to file) |
|
|
|
|
|
|
|
39 |
A table of contents is provided for PEIMs that are lengthy |
|
|
|
|
|
|
|
Quality
|
40 |
The patient education material stated that there may be more than one treatment choice |
|
|
|
|
|
|
41 |
The patient education material has outlined the benefits and side effects of each treatment modality |
|
|
|
|
|
|
|
42 |
A patient education material has stated what will happen if no treatment is used |
|
|
|
|
|
|
ابزار زیر جهت ارزشیابی منابع آموزش بیمار (بروشور، پمفلت، کتابچه و مانند آن) طراحی شده است. بروشور پیوست را مطالعه نمایید و با استفاده از ابزار زیر مشخص کنید که آیا این منبع معیارهایی را که در تهیه و ارزشیابی یک منبع آموزش بیمار باید مدنظر قرار گیرد را برآورده میکند یا خیر. هر کدام از این معیارها به صورت عبارتهایی بیان شده است و امتیاز هر عبارت عددی بین یک تا پنج میباشد که به صورت زیر است:
1. درباره این منبع کاربردی ندارد، 2. اصلا برآورده نمیکند، 3. کمی برآورده میکند، 4. تا حد زیادی برآورده میکند، 5. کاملا برآورده میکند،
-1 سن، -2 جنس، -4 رشته تحصیلی، -5 آخرین مقطع تحصیلی، -6 رتبه علمی، -7 دانشگاه محل کار.
|
بعدبعد
|
ششماره گویه ماره گویه |
گویه ها
|
0 درباره این منبع کاربرد ندارد 1 اصلا بر0 درباره این منبع کاربرد ندارد 1 اصلا برآورده نمیکند 2 کمی برآورده میکند 3 تا حد زیادی برآورده میکند 5 کاملا برآورده می کندآو |
||||
|
خوانایی |
1 |
|
|
|
|
|
|
|
2 |
منبع آموزش بیمار، بر نکات مهم تاکید کرده است |
|
|
|
|
|
|
|
3 |
منبع آموزش بیمار در صورت نیاز، اطلاعات را در قالب نمودار یا تصویر نشان می دهد |
|
|
|
|
|
|
|
4 |
منبع آموزش بیمار دربردارنده خلاصههای دقیق و منسجمی از پیامهایی است که قرار است انتقال داده شود |
|
|
|
|
|
|
|
5 |
اصطلاحات پزشکی ضروری تعریف شده است |
|
|
|
|
|
|
|
6 |
از کلمات مبهم و ناآشنا برای مخاطبان استفاده نشده است |
|
|
|
|
|
|
|
7 |
برای سادهسازی دستورالعملها از کمککنندههای تصویری استفاده شده است |
|
|
|
|
|
|
|
8 |
بار اطلاعاتی (مقدار و تازگی و عدم ابهام اطلاعات) منبع برای مخاطب مناسب است |
|
|
|
|
|
|
|
9 |
نکات مهم به صورت پررنگ مشخص شدهاند. |
|
|
|
|
|
|
|
طراحی |
10 |
فاصـله بین سـطرها به گونهای اسـت که خواندن مطالب را آسـان میکـند |
|
|
|
|
|
|
11 |
نوع قلم به گونهای است که خواندن مطالب برای مخاطبان را آسان میکند |
|
|
|
|
|
|
|
12 |
اندازه قلم به گونهای است که خواندن برای مخاطبان را آسان میکند |
|
|
|
|
|
|
|
13 |
فاصلهها و چیدمان متن و تصاویر برای بیننده چشمنواز و گیراست |
|
|
|
|
|
|
|
ساختار |
14 |
منبع از کمککنندههای تصویری (مانند قلم درشتتر، برجسته کردن، فلش، در کادر قرار دادن و مانند آن) استفاده کرده است |
|
|
|
|
|
|
15 |
رنگ به عنوان یک عامل راهنما برای تأکید بر مطالب و تقویت یادگیری استفاده شده است |
|
|
|
|
|
|
|
16 |
اطلاعات مهم به صورت فهرستها و طبقهبندیها سازماندهی شده است |
|
|
|
|
|
|
|
انسجام |
17 |
ایدههای نشـان داده شـده در منبع اطلاعـاتی آموزش بیمار به منظور انتقال اطلاعات، به طور منطقی ساختاری پیوسته دارد |
|
|
|
|
|
|
18 |
اطلاعات در جملات به طور طبیعی از سطح کلی تا جزئی جریان یافته است |
|
|
|
|
|
|
|
19 |
محتوای منبع به طور منطقی و از سادهتر به پیچیدهتر سازماندهی شده است |
|
|
|
|
|
|
|
20 |
منبع اطلاعات یا محتوایی که باعث منحرفشدن از هدف شود را در بر نمیگیرد |
|
|
|
|
|
|
|
تطابق |
21 |
توصیههای ارائه شده با باورها، ارزشها و فرهنگ مخاطبان منبع آموزشی متناسب است |
|
|
|
|
|
|
22 |
منبع آموزشی با استانداردهای جامعه متناسب است |
|
|
|
|
|
|
|
23 |
مثالهای بکاربرده شده در منبع آموزش بیمار، در برگیرنده ویژگیهای اساسی ایدهها و مفاهیم مورد بحث هستند |
|
|
|
|
|
|
|
24 |
منبع آموزش بیمار به آداب و رسوم و سنتهای مخاطبان احترام میگذارد |
|
|
|
|
|
|
|
تناسب |
25 |
در منبع پرسشهایی به کار رفته است تا مخاطبان را تشوبق به مشارکت کند |
|
|
|
|
|
|
26 |
عنوان منبع اطلاعاتی آموزش بیمار، هدف منبع را انتقال میدهد |
|
|
|
|
|
|
|
27 |
محتوای آموزشی، اهداف یادگیری را پوشش میدهد |
|
|
|
|
|
|
|
عمل پذیری |
28 |
در فعالیتهای خودمراقبتی، گامها با مثال توضیح داده شدهاند |
|
|
|
|
|
|
29 |
منبع روند کار هر درمان را توصیف میکند |
|
|
|
|
|
|
|
30 |
محتوا روی آنچه مخاطب باید انجام بدهد و به همـان اندازه آنچه باید بداند، تمرکز کرده است |
|
|
|
|
|
|
|
31 |
مخاطبان به راحتی میتوانند آنچه را نیاز دارند، در منبع اطلاعاتی بیابند |
|
|
|
|
|
|
|
قابلیت اطمینان |
32 |
مشخص است که برای گردآوری اطلاعات چه منابع اطلاعاتی به کار برده شده است |
|
|
|
|
|
|
33 |
زمان تولید منبع اطلاعاتی، مشخص است |
|
|
|
|
|
|
|
34 |
در تهیه منبع اطلاعاتی از آخرین منابع و شواهد علمی معتبر استفاده شده است |
|
|
|
|
|
|
|
35 |
منبع جزئیاتی مانند سازمانهای حمایتکننده یا وبسایتها را برای اطلاعات بیشتر مخاطبان ارائه میکند |
|
|
|
|
|
|
|
قالببندی |
36 |
منبع اطلاعاتی آموزش بیمار از عناصر تصویری واضح و ساده استفاده کرده است |
|
|
|
|
|
|
37 |
از تصویر و دیاگرام برای سادهسازی محتوا استفاده شده است |
|
|
|
|
|
|
|
38 |
اندازه منبع آموزش به بیمار به گونهای است که به راحتی توسط مخاطب استفاده شود |
|
|
|
|
|
|
|
39 |
برای منابع آموزش بیمار که طولانی هستند، فهرست مطالب تهیه شده است |
|
|
|
|
|
|
|
کیفیت |
40 |
منبع آموزش بیمار بیان کرده است که ممکن است بیش از یک انتخاب درمانی وجود داشته باشد |
|
|
|
|
|
|
41 |
منبع آموزش بیمار مزایا و عوارض هر شیوهدرمانی را بیان کرده است |
|
|
|
|
|
|
|
42 |
منبع آموزش بیمار بیان کرده است که در صورت به کارنبردن هیچ درمانی، چه اتفاقی خواهد افتاد |
|
|
|
|
|
|