Document Type : Case report
Subjects
Abstract
Background: In this study, treatment of maxillary deficiency through posterior maxillary miniplates connected to facemask was presented. Using skeletal anchorage rather than tooth-borne device, facilitated maxillary protraction with minimum dental changes. Also, the patient exhibited vertical growth pattern, which could be aggravated through tooth-borne devices. But through skeletal anchorage, clockwise rotation of mandible and counterclockwise rotation of maxilla were prevented. Desired results were obtained after 9 months of treatment including positive overjet, without any mandibular backward rotation and improved midface deficiency, followed by 10 months of retention period through using facemask only night time. Then, fixed orthodontic treatment was initiated to stabilize the results.
Keywords: Mandible, Masks, Micrognathism, Overbite, Rotation
Introduction
Class III malocclusion caused by maxillary deficiency is one of the orthodontic problems which requires early treatment, most common by protraction face mask appliance. It is suggested to start the treatment before the age of 10 in order to obtain more skeletal changes rather than dental (1,2). Normaly, face mask is used along with tooth-borne anchorage appliances, which beside its positive skeletal changes, it can cause many side effects such as: backward rotation of mandible, forward rotation of maxilla, proclination of maxillary incisors and retroclination of mandibular incisors, mesial movement and extrusion of maxillary posterior teeth (3,4). Thus, in order to overcome the side effects, skeletal anchorages such as orthodontic miniscrews or miniplates were introduced to be used instead of tooth-borne devices (5,6).
Miniplates have many advantages during treatment such as possibility of immediate force application after insertion, causing minimum irritation of the surrounding soft tissue, and most importantly providing absolute anchorage (7,8). However, these anchorage devices need to be inserted and then removed after treatment by a trained surgeon, which can be considered as the remarkable disadvantage of this approach (8).
Previous studies have suggested inserting miniplate anchorage at lateral nasal wall of maxilla or infrazygomatic crest for the best results during facemask therapy (9-12). Any of them would transmit the orthopaedic forces directly to the circummaxillary sutures, without any inadvertent dental changes despite using tooth-borne appliances (13). Many of the previous studies have used anterior miniplate anchorage for maxillary protraction and suggested them for promising results (10,14-16). It has been claimed that anterior miniplates provides force vector nearer to the center of resistance of maxilla and subsequently lesser counterclockwise rotation of the nasomaxillary complex, in comparison to posterior miniplates (9).
In this case report, a 10-year-old patient was presented with maxillary deficiency and vertical growth pattern, treated with facemask besides miniplates in infrazygomatic crest, showing satisfying results after 9 months of treatment.
Case presentation
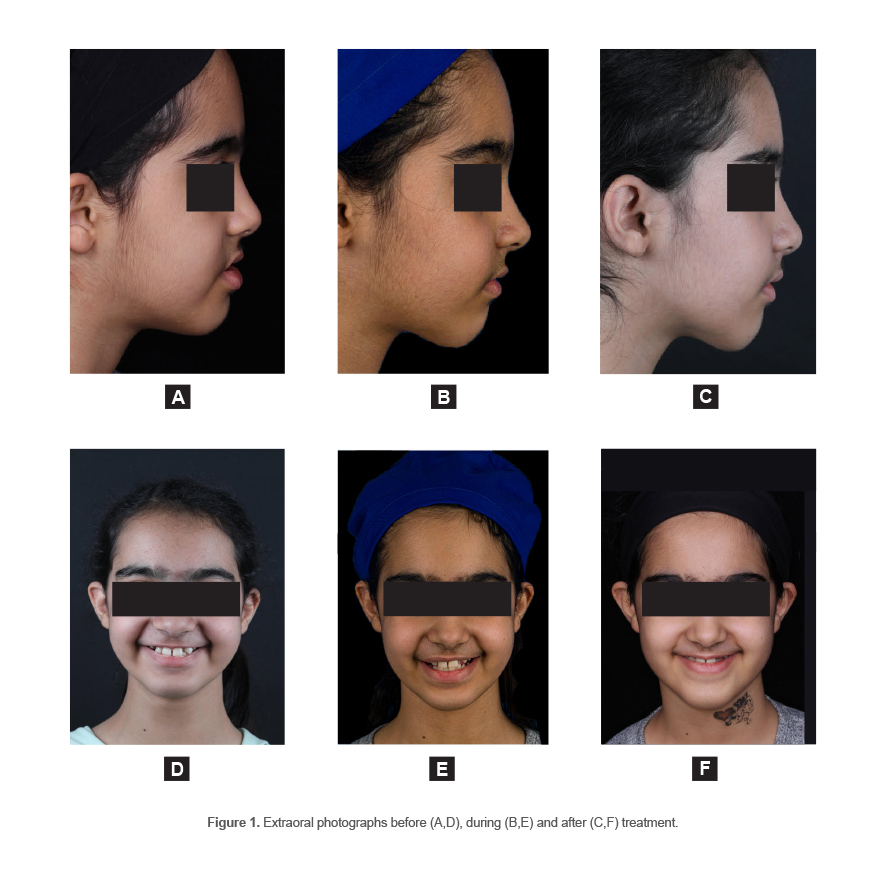
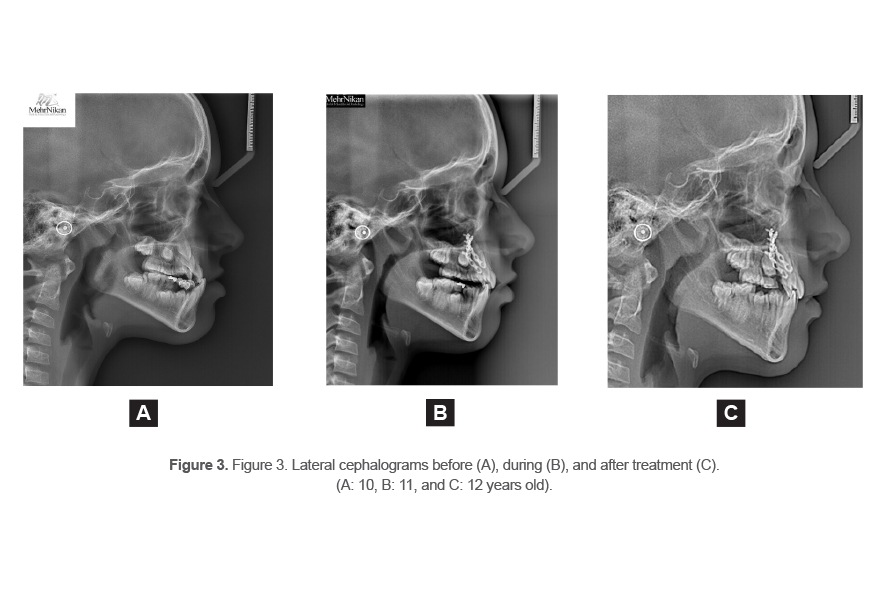
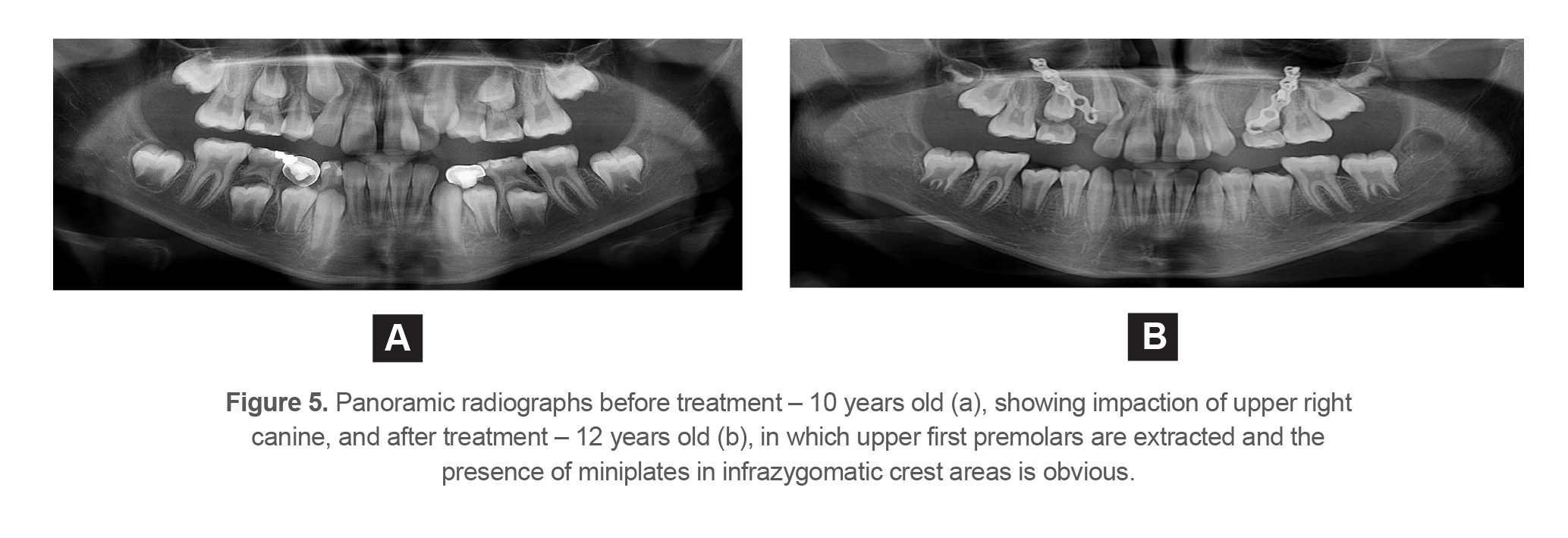
A 10-year-old girl referred to the private clinic of the first author with chief complaint of irregularity of teeth and imbalance of the jaws. In preliminary extraoral examination, straight profile with midface and upper lip retrusion, leptoprosopic face, and decreased incisor show during smile were observed. Also, in intraoral examination, reverse overjet, severe space deficiency in upper arch and deviation of upper dental midline were observed. Accordingly, radiographic records were obtained. In panoramic view, impaction of upper right canine with proximity of its crown to the root of the adjacent lateral incisor was obvious, which was also confirmed by cone-beam tomographs. In lateral cephalogram, the patient was skeletally class III with maxillary retrognathism and also had vertical growth pattern with backward rotation of mandible. Also, retrusion of maxillary incisors and retroclination of mandibular incisors was observed. According to the cervical vertebral maturation staging (17), the patient was in late CS2.
The treatment plan was to correct sagittal skeletal relationship through maxillary protraction besides controlling vertical growth and subsequently to correct reverse overjet. Also, it was planned to provide space in maxillary arch and to resolve the impaction of left maxillary canine.
Results
Considering the patient’s age, stage of mandibular growth, and vertical growth pattern, it was decided to use skeletal anchorage for maxillary protraction through face mask therapy. Therefore, at the first step, the patient was referred to oral and maxillofacial surgeon to insert bilateral posterior miniplates inferior to infrazygomatic crest. Next, face mask was prescribed for the patient so that the force magnitude was 250 g at each side with line of force near to the center of resistance of maxilla (18), with at least 14 hours of use per day, which was connected through elastics (5/16 inches, medium size) to the extension of miniplates. Simultaneously, upper removable plate with expansion screw and posterior biteplates was used to correct mild constriction of maxilla.
The patient used face mask fulltime during 9 months with good cooperation. After this period, soft tissue changes were noticeable along with increase in projection of midface and upper lip (Figures 1 and 2). Hence, maxillary protraction was successfully obtained without any mandibular backward rotation, and without dental changes in maxillary arch. Also, reverse overjet was resolved (Figures 3 and 4). The comparison between the results of lateral cephalogram analysis before, during and after treatment is shown in table 1.
In the next step, due to severe space deficiency in upper arch and impaction of the left upper canine, upper first premolars were extracted, which resolved the impaction of canine without any further treatment (Figure 5). During the next 10 months, the patient continued using facemask night-time, to stabilize the results. In the final step, fixed orthodontic treatment got started to obtain stable and functional occlusion.
Table 1. Lateral cephalogram analysis before, during and after treatment
|
|
Norm |
Before |
Progress |
After |
|
FH-SN |
6-8° |
5.3° |
5.6° |
5.6° |
|
Jarabak index |
394° |
398.5° |
399° |
399.5° |
|
Inclination angle |
85° |
85.2° |
85.7° |
83.7° |
|
Mandibular plane-SN |
32° |
38.5° |
39° |
39.5° |
|
Occlusal plane-SN |
14° |
18° |
18.4° |
21.6° |
|
SNA |
82° |
80° |
82.2° |
82° |
|
SNB |
80° |
79.8° |
79° |
78.6° |
|
ANB |
2° |
0.2° |
3.2° |
3.4° |
|
Wit’s appraisal |
-1 mm |
- 4.8 mm |
-2 mm |
-3.5 mm |
|
U1-SN |
102° |
101.7° |
97.8° |
99.4° |
|
IMPA |
90° |
82.9° |
79° |
78.9° |
|
Upper lip to E-line |
-1 mm |
-5 mm |
-2.1 mm |
-2.5 mm |
|
Lower lip to E-line |
0 mm |
0.3 mm |
1.6 mm |
0.2 mm |
FH: Frankfurt plane, S: saddle, N: nasion, Jarabak index: sum of Saddle, Articular and Gonial angel, Inclination angle: the angle between palatal plane (ANS-PNS) and perpendicular line from Se-N’ plane, Mandibular plane: Gonion- Gnathion plane, A: point A, B: point B, U1: Upper incisor, IMPA: Incisor Mandibular Plane Angle, E-line: the line connecting pronasale to soft tissue pogonion.
Discussion
In this paper, treatment of a 10-year-old girl with class III malocclusion caused by maxillary deficiency along with vertical growth pattern, severe space deficiency and canine impaction in upper arch, was discussed. Conventionally, facemask therapy connected to a tooth-borne fixed or removable device was exerted for correction of maxillary deficiency. However, various factors can affect treatment outcomes, such as patient’s age. Most previous studies have suggested to start treatment in primary or early mixed dentition or chronologically before 10 years old to obtain more skeletal changes (19-21). Our patient was 10 years old and also according to the cervical vertebral maturation staging (17), she was in late CS2. So, conventional facemask therapy with conventional tooth-borne devices could generate greater dental changes rather than skeletal. Also, another important consideration was patient’s vertical growth pattern along with clockwise rotation of mandible. As it is known, conventional facemask therapy has various side effects such as counterclockwise rotation of maxilla and clockwise rotation of mandible (22), which would be disastrous for the presented case. Considering the mentioned factors, it was decided to use skeletal anchorage beside facemask to minimize side effects of the treatment.
Miniplates were inserted surgically in infrazygomatic crest area with external extensions apical to first upper premolars for elastics of face mask. Previous studies have used both posterior miniplates in infrazygomatic crest (23,24) and anterior miniplates in lateral nasal wall of maxilla (15,25) for facemask therapy, and both areas demonstrated promising results. Although, it has been suggested to use anterior miniplates to provide a force vector near to the maxillary center of resistance, in order to decrease counterclockwise rotation of maxilla and better vertical control (9). However, in the presented case, due to unerupted maxillary canines and lower bone density in the anterior region in comparison to infrazygomatic crest, considering patient’s age, in spite of the vertical growth pattern, it was decided to use posterior miniplates. Despite the expectation, lateral cephalogram analysis showed only 1° mandibular clockwise rotation, which is clinically insignificant. Not only counterclockwise rotation of maxilla did not occur, but also slight clockwise rotation of maxilla was obvious. Conclusively, despite using posterior miniplates, vertical growth was controlled successfully. It is suggested to compare the vertical effects of maxillary protraction through facemask connected to anterior and posterior miniplates in later clinical studies.
According to the lateral cephalograms, maxilla was advanced about 2 degrees but unexpectedly, backward mandibular movement was also occurred about 1.2 degrees. Also, retrusion of upper lip was resolved through 2.5 mm forward movement of the upper lip. Similar results were observed by Lee et al (26), showing greater maxillary advancement and lesser mandibular rotation through posterior miniplates in comparison to rapid maxillary expansion devices connected to facemask. Also, Sar et al (14) have shown similar results with skeletal anchorage, suggesting that it achieves satisfying results in shorter treatment time. In the presented case, desired changes were obtained after 9 months.
Despite the conventional facemask therapy which causes proclination of upper incisors (22), in this approach, upper incisors had no proclination after treatment. Similarly, Elnagar et al (24) confirmed that skeletal anchorage eliminates dental changes in upper arch. However, due to the leaning of facemask on chin in both approaches, retroclination of lower incisors has occurred in this patient as well (27). In order to prevent any dental changes during maxillary protraction, the best approach is to use miniplates in infrazygomatic crest along with miniplates in anterior region of mandible, connected with intermaxillary elastics suggested by De Clerck et al (6). Thus, there would be no changes in inclination of mandibular incisors despite facemask therapy. However, mandibular canines should be erupted before insertion of miniplates. While starting the treatment of the presented case, mandibular canines were not erupted, hence this treatment modality was not a suitable choice for the patient.
Previously, it was shown that maxillary protraction through skeletal anchorage is accompanied by advancement of zygoma through the opening of the zygomaticofrontal, zygomaticotemporal, and zygomaticomaxillary sutures (28). Also, in the presented case, advancement of midface and upper lip after treatment was eminent in clinical view and also in lateral cephalogram superimpositions.
Although due to maxillary deficiency in class III malocclusions, it is not preferred to provide space through extractions in upper arch, but in this case, due to severe space deficiency in upper arch and impaction of maxillary canine, it was decided to extract first upper premolars. After extraction, the impaction was resolved without any other treatment. Finally, fixed orthodontic treatment was initiated to provide functional occlusion and stabilize the results.
Conclusion
In this study, a patient with class III malocclusion caused by maxillary deficiency along with vertical growth pattern, was successfully treated with facemask in combination with miniplates in infrazygomatic crest area. In addition to the significant maxillary advancement, vertical dimension was controlled without mandibular clockwise rotation. Also, dental changes in maxillary arch were minimized through avoiding tooth-borne devices and soft tissue changes such as advancement of midface and upper lip was remarkable. It is suggested to investigate the effect of location of maxillary miniplates in facemask therapy on vertical dimension changes in further clinical studies.
Ethical approval
It was a case report.
Consent
Written informed consent was taken from the patient and her parents for publication of this case report and the accompanying images.
Conflict of Interest
There was no conflict of interest in this manuscript.