Document Type : Review article
Introduction
Influenza is an acute respiratory infection with different severity in children. There is a range of upper and lower respiratory tract infections caused by the virus 1,2.
Influenza viruses are mainly spread by droplets during sneezing, talking and coughing. Less often, touching the solid objects with hands that are contaminated with nasal secretion can transmit the virus. This viral infection can be transmitted before beginning of symptoms until about 5-7 days after symptoms appear 3,4.
The common symptoms of influenza are fever or feeling feverish/chills, runny nose, sore throat, coughs, muscle or body aches, headache, and fatigue. Some patients may have vomiting and diarrhea, which are more commonly seen in children than adults. Most people completely recover, with exception of patients from high risk groups 5,6. People at higher risk for developing flu-related complications include; young children (less than 2 years old), older people (65 years of age and older), pregnant women, and people with certain chronic health condition including; history of asthma or other chronic pulmonary disease (e.g. cystic fibrosis), hemodynamically significant cardiac disease, neurological and neurodevelopmental conditions, immunosuppressive disorders or therapies, sickle cell anemia and other hemoglobinopathies, chronic renal dysfunction, metabolic disease (e.g. diabetes mellitus), weakened immune system due to other diseases or medications, people younger than 19 years of age who are receiving aspirin therapy, increased risk of aspiration and extreme obesity (BMI≥40) 7.
Four types of influenza viruses are A, B, C, and D. Influenza types A and B cause human infection annually during the epidemic season. Influenza A has several subtypes according to the combination of hemagglutinin (H) and the neuraminidase (N) proteins that are expressed on the surface of the virus. There are 18 different hemagglutinin subtypes and 11 different neuraminidase subtypes (H1-18 and N1-11). Influenza A virus can be categorized as the H and N types (H1N1 and H3N2). Influenza B virus is classified into lineages and strain types. Currently circulating influenza B virus belong to one of two lineages: B/Yamagata and B/Victoria 7,8.
The WHO’s Global Influenza Program (GIP) collects and analyses virological and epidemiological influenza surveillance data from around the world. This regular sharing of quality influenza surveillance and monitoring data by countries allows WHO to support the selection of influenza strains for vaccine production 9,10.
The periodic replacement of viruses in influenza vaccines is necessary in order for the vaccines to be effective because the constant evolving nature of influenza viruses, including those circulating and infecting humans; so based on such a data, the next year vaccine can be manufactured. Type C influenza cases are much less frequent than that of A and B. Therefore, only influenza A and B viruses are usually included in flu vaccines every year by the World Health Organization (WHO) 11-13.
In Iran, same as the other countries in northern hemisphere, seasonal influenza typically occurs in autumn and winter, mainly from October to March 14.
The symptoms and signs of influenza varies so children with flu may show mild to severe symptoms according to their co-morbidity, medical and vaccination history. Infant less than 3 months old with influenza may present with sepsis and shows symptoms like illness, apnea or cyanosis, irritability, tachypnea, moderate to severe dehydration, lethargy, protracted vomiting, severe diarrhea, floppiness and convulsion 8.
In infants and toddlers between 3 months to 5-years of age complex febrile convulsion, loss of consciousness, biphasic illness, protracted vomiting, sudden onset of anorexia, inability to take fluid, high grade fever of more than 3 days, chest or abdominal pain, asthma not responding to usual treatment, and hemodynamics instability, need extra evaluation 8.
Definite diagnosis of influenza needs nasopharyngeal PCR genetic test and the choice for treatment of this viral respiratory tract infection is Oseltamivira. Findings from researches for those needing PCR and medical treatment is still controversial 8.
Preventing transmission of influenza viruses within health care settings requires a multi-disciplinary approach that includes: vaccination, laboratory testing, infection control, antiviral treatment, and antiviral chemoprophylaxis 8.
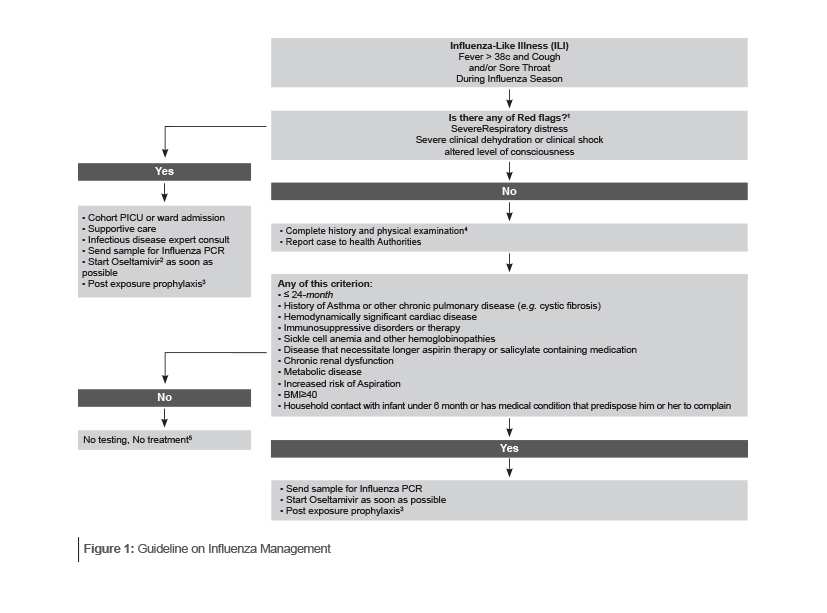
According to several guidelines and our experiences in Iran we suggest following the clinical algorithm for evaluation, diagnosis, treatment and antiviral chemoprophylaxis of infants and children who are suspected for influenza (Figure 1).
1. Red Flags
Severe respiratory distress:
• Lower chest wall indrawing, sternal recession, grunting, or noisy breathing when calm
• Tachypnea: Birth- 3 m >60/min, 3 m-1 yr >50/min, 1-3 yr >40/min, 3-6 yr >35/min, 6-12 yr >30,12-18 yr >20
• Oxygen saturation ≤92% on pulse oximetry, breathing air or on oxygen
• Respiratory exhaustion or apneic episode (Absence of cyanosis as a ≥20 second pause in breathing)
• PaO2/FiO2 ratio; ≤300 for ALI or ≤200 for ARDS
Sever clinical dehydration or clinical shock:
• Sternal capillary refill time >2 second, reduced skin turgor, sunken eyes or fontanelle
Altered conscious level
• Strikingly agitated or irritable, seizure, or floppy infant
2. Oseltamivira dosage:
• Children ≥12 month by body weight
• ≤15 kg: 30 mg, twice daily
• >15-23 kg: 45 mg, twice daily
• >23-40 kg: 60 mg, twice daily
• >40 kg: 75 mg, twice daily
• Infants 9-11 month, 3.5 mg/kg/dose, twice daily
• Term infants 0-8 month, 3 mg/kg/dose, twice daily
• Preterm Infant: (gestational age + chronological age):
• >40 wk postmenstrual age 3.0 mg/kg/dose, orally, twice daily,
• 38-40 wk postmenstrual age 1.5 mg/kg/dose, orally, twice daily,
• wk postmenstrual age: 1.0 mg/kg/dose, orally, twice daily,
• wk (extremely preterm infants), please consult a pediatric infectious diseases physician.
• Adults 75 mg, twice daily 75 mg
3. Indication of prophylaxis:
In general, it does not recommend pre-exposure antiviral chemoprophylaxis, but antiviral medications can be considered for chemoprophylaxis to prevent influenza in certain situations, such as the following examples:
• Prevention of influenza in persons at high risk of influenza complications during the first two weeks following vaccination, after exposure to a person with influenza.
• Prevention for people at high risk for complications from influenza who cannot receive influenza vaccine due to a contraindication, after exposure to a person with influenza.
• Prevention for people with severe immune deficiencies or others who might not respond to influenza vaccination, such as persons receiving immunosuppressive medications, after exposure to a person with influenza.
• For family members and close contacts of an infected person if those people are at high risk of complications from influenza.
• For children at high risk of complications and their family members and close contacts, as well as HCP, when influenza viruses circulating in the community are not matched with seasonal influenza vaccine strains.
Note that,
1. Antiviral chemoprophylaxis generally is not recommended if more than 48 hours have elapsed since the first exposure to a person with influenza.
2. Patients receiving antiviral chemoprophylaxis should be encouraged to seek medical evaluation as soon as they develop a febrile respiratory illness that might indicate influenza.
Oseltamivir prophylaxis dosage for Children for 7 days
• ≥12 month: by body weight
• ≤15 kg: 30 mg; once daily
• >15-23 kg, 45 mg: once daily
• >23-40 kg, 60 mg: once daily
• >40 kg, 75 mg: once daily
• Infants 9–11 month. 3.5 mg/kg/dose, once daily
• Term infants 0 to 8 month 3 mg/kg/dose once daily
4. Influenza diagnosis symptoms and signs:
A. Systemic (fever, headache, Anorexia, illness, myalgia)
B. Respiratory (cough, rhinorrhea, sore throat, nasal stuffiness, hoarseness)
C. GI (abdominal pain, diarrhea and vomiting)
D. Signs (fever, conjunctival congestion, lymphadenopathy)
Consider these signs and symptoms for influenza in these specific age group:
• Infant ≤3 months: Sepsis like illness, apnea or cyanosis, severe irritability, tachypnea, moderate to severe dehydration, lethargy, protracted vomiting, severe diarrhea, floppiness, and convulsion
• Infant and toddlers between 3 months to 5 years: Loss of consciousness, abnormal behavior, worsening illness, protracted vomiting and sudden onset of anorexia, dizziness, or light headed ness, unable to take fluid, high grade fever more than 3 days, chill, decreased appetite, activity and fluid intake, chest or abdominal pain, asthma not respond to usual treatment, and hemodynamics instability.
Consider H1N1 infection in influenza seasons in any child with atypical CNS, Cardiopulmonary, gastrointestinal or renal symptoms.
5. In any child (birth through 18 year) especially in influenza seasons red flags should be given to parents, to return child back to medical centers and/ or contact the physicians.