Document Type : Original article
Introduction
Regarding the National Center for Iranian Statistics, one of the densely populated provinces of Iran is Alborz province, with a population of 2,712,400 people. 93% live in urban and 7% in villages. 96.8% of Alborz population are Iranians (Persian, Turks, Kurds, Lars, Arabs, etc.) and the rest are from other countries such as Iraqi, Afghan, Pakistani, and others, which consists 3.1% of the whole provincial population. The distribution of population by ethnicity in this province was reported to be 47% Persian, 36.1% Turkish, 7.4% Kurdish, 4.4% Northern and the rest from other Iranian ethnicities. Muslims are 99.6% followed by the Christian, Ashura, Zoroastrian, Armenian and other Christians. The number of students aged 6 years and older is 427057. The literacy rate is 92.2% and the marriage rate is 63.83% with 2.58% divorcing.The rate of unemployment is 13.8%.
The number of households in this province is 856,116 and the average family member is 3.17. The total number of individuals aged 6 to 18 years in the province is 596,728 , of which 552,802 are in urban areas1.
About a quarter of psychiatric disorders usually occur by the age of 14, so paying attention to psychiatric disorders is important during childhood and adolescence2
Eidemiologic studies provide estimations of the prevalence of mental disorders and allow planning for appropriate interventions3. The burden of mental health and psychiatric disorders in children and adolescents is one of the major problems in countries with low and middle income levels where there are no apparent policies to eefectively deal with them4. Peterson, in a systematic review on Mental Health Services, carried out a 10-year study (2000-2010) on such services in South Africa. They stated that although progress in the field of epidemiological studies was remarkable during that period, there was no suggestions for interventions and no relevant economic studies to cover the causative factors5.
To our best of knowledge, before the current study, no similar studies on mental health and psychiatric disorders for this age group with appropriate sample size, proper distribution of dispersion of the population under study and the examination of a large number of effective demographic factors in the distribution of mental health and psychiatric disorders have been conducted in Alborz province.
We hope that the results of this study will help reducing the prevalence rate of mental health disorders in Alborz community and provide sufficient information to plan proper policies to identify affected cases, to produce preventative interventions and appropriate therapies.
Materials and Methods
Study design
This cross-sectional study was part of a national project that was implemented in all provinces of Iran, including the province of Alborz6. The National Institute for Medical Research Development (NIMAD) supported this study.
The principal researcher in this study has extensive research experiences in the field of psychiatric disorders and has special expertise in the use of the tools in this study. Principal Investigator and colleagues used the Kiddie-Sads-Present and Lifetime Version (K-SADS) Persian version of the reader’s intuition and reliability toincreased the sensitivity and specificity of the Persian version.
In a community-based study, 1008 children and adolescents aged 6-18 years from the Alborz province were selected by multistage cluster sampling (cluster and randomized sampling). Then, 167 blocks were randomly selected according to the postal codes. From each cluster group, 12 cases were selected and 6 subjects of each sex were grouped based on different ages (6-9 years, 10-14 years old and 15-18 years old).
Inclusion and Exclusion Criteria
Inclusion criteria were: citizens of the Alborz province (individuals must have constantly lived in the province for at least one year), and the age range between 6 and 18 years old. Exclusion criteria were: Children and adolescents with severe physical illness )because of the possibility of causing or influencing effects on psychiatric disorders, especially in this age group).
Data collection
Trained clinical psychologists went to children’s homes and interviewed them. They required the participants to complete the Persian version of the K-SADS-PL. The time required to complete the K-SADS was about 30 to 40 minutes. Also, demographic information (gender, age, education, parental education, and economic status) were collected during the interviews.
Procedure
This study is part of the IRCAP survey which was conducted in different urban and rural areas of Alborz province6. A total of 167 clusters (6 samples each) were selected from each province. In Alborz province, according to the same structure, a survey was carried out on 1008 children and adolescents. Along with the main city of the province, the rural population was also randomized (using cluster sampling). In the next step, the blocks were randomly selected according to the postal codes. Therefore, we expect to see samples of both urban and rural areas in the Alborz province. The data of this study was obtained in Persian.
During screening and diagnostic stages, a random sample of children aged 6 to 18 years was selected to measure the validity of the K-SADS-PL questionnaire. For children under 11 years of age, questionnaires were completed simultaneously and independently by their parents, and older children completed the questionnaires by themselves.
No information was lost in the diagnostic aspects, but we lost a limited number of demographic information (five items in the field of father education, four in the field of maternity education, as well as six items and four items in the field of father’s and mother’s jobs).
Statistical analysis
We used descriptive analysis and 95% confidence interval and a p value of
Scales
Kiddie-SADS-Present and Lifetime (K-SADS-PL):
KSADS-PL is a type of interview to study mood disorders and schizophrenia in school-aged children. The Present and Lifetime version is a semi-structured psychiatric interview that is based on the DSM-IV criteria, which includes 5 diagnostic groups including emotional disorders7, psychotic disorders8, anxiety disorders;9, disruptive behavioral disorders10, and substance disorder11, eating disorders and elimination disorders (enuresis/encopresis)12.
The interview starts with questions about basic demographic information followed byquestions about present complaints and prior mental health status and psychiatric problems13.
The reliability of the Persian version of this questionnaire was 0.81 and the inter-rater reliability was 0.69 using test-retest. The sensitivity and the specificity of the Persian version of K-SADS have been found to be high14.
Ethics
The consent form was given to individuals participating in this study. The consent of participants aged less than 15 years old was given by their parents. All information about children and adolescents and their families was kept confidential. If a psychiatric disorder was diagnosed by psychiatrists, the children and adolescent cases from the IRCAP project were treated for free. However, if participants or their parents were not willing to use free treatment, they would refer to children and adolescent psychiatrists working privately. The National Institute for Medical Research Development (NIMAD) supported this study (IR code: IR.NIMAD.REC.1395.001).
Result
The aim of this study was to determine the profile of mental health problems in children and adolescents aged 6 to 18 years old living in urban and rural areas of Alborz province. The sample consisted of 1008 children and adolescents, including 501 boys (49.7%) and 507 girls (50.3%) . 96.2% of the participants lived in urban and 3.8% in rural areas.
Mental health disorders were diagnosed in 75 (15%) boys and 61 (12%) girls that 133 were from urban (13.7%) and 3 from rural areas (7.9%).
The highest prevalence of disorders was among fathers of children with bachelor education (21.4%) and the mothers of those with MSc or higher degrees (23.4%), while the highest prevalence of parental education among all the participants was diploma degree.
The most mental health disorders were found among the children of fathers and mothers with a public sector job (15.9 and 25.4%, respecttively) (Table 1).
Table 1. Frequency of demographic variables in children and adolescents (6-18 years old) of Alborz province and prevalence of psychiatric disorders in terms of these variables
|
CI (95%) |
With disorder |
Total |
|
|||
|
P(%) |
N |
P (%) |
N |
|||
|
12.1-18.4 |
15 |
75 |
49.7 |
501 |
Boy |
Sex |
|
9.5-15.2 |
12 |
61 |
50.3 |
507 |
Girl |
|
|
8.4-15.3 |
11.4 |
38 |
33 |
333 |
6-9 |
Age (years) |
|
9.9-16.8 |
13 |
48 |
36.7 |
370 |
10-14 |
|
|
12.7-21 |
16.4 |
50 |
30.3 |
305 |
15-18 |
|
|
12-16 |
13.7 |
133 |
96.2 |
970 |
Urban |
Place of residence |
|
2.7-20.8 |
7.9 |
3 |
3.8 |
38 |
Rural |
|
|
|
0 |
0 |
2.2 |
22 |
Illiterate |
Father’s education |
|
0.8-9.7 |
2.8 |
2 |
7.1 |
71 |
Primary school |
|
|
5-13.4 |
8.3 |
14 |
16.8 |
169 |
Guidance & high school |
|
|
8.9-15.6 |
11.9 |
43 |
36.1 |
362 |
Diploma |
|
|
17.2-26.3 |
21.4 |
66 |
30.8 |
309 |
Bachelor |
|
|
7.9-24.3 |
14.3 |
10 |
7 |
70 |
MSc or higher |
|
|
|
|
1 |
|
5 |
Missing |
|
|
|
0 |
0 |
2 |
20 |
Illiterate |
Mother’s education |
|
2.3-11.7 |
5.3 |
5 |
9.5 |
95 |
Primary school |
|
|
7.9-18.1 |
12.1 |
19 |
15.6 |
157 |
Guidance & high school |
|
|
8.9-15.1 |
11.6 |
47 |
40.2 |
404 |
Diploma |
|
|
14.7-23.8 |
18.9 |
53 |
28 |
281 |
Bachelor |
|
|
13.6-37.2 |
23.4 |
11 |
4.7 |
47 |
MSc or higher |
|
|
|
|
1 |
|
4 |
Missing |
|
|
12.4-20.2 |
15.9 |
54 |
33.8 |
339 |
Public sector |
Father’s job |
|
10.1-15.3 |
12.5 |
79 |
63.3 |
634 |
Private sector |
|
|
1.9-22 |
6.9 |
2 |
2.9 |
29 |
unemployed |
|
|
|
|
|
|
6 |
Missing |
|
|
18.7-33.5 |
25.4 |
33 |
12.9 |
130 |
Public sector |
Mother’s job |
|
6-25.2 |
12.8 |
6 |
4.7 |
47 |
Private sector |
|
|
9.6-14 |
11.6 |
96 |
82.4 |
827 |
unemployed (Housewife) |
|
|
|
|
|
|
4 |
Missing |
|
|
11.4-15.6 |
13.4 |
135 |
100 |
1008 |
Total |
|
Odds Ratios (95% CI) for total psychiatric disorder in term of demographic variables have been shown in table 2.
Table 2. Odds Ratios (95% CI) for total psychiatric disorder in term of demographic variables
|
Variables and their categories |
OR (crude) |
CI (95%) |
p-value |
OR (adjusted) |
CI (95%) |
p-value |
||
|
Demographic variables |
Sex |
Male |
1.00 Baseline |
|
|
|
|
|
|
Female |
0.777 |
0.540-1.117 |
0.173 |
0.767 |
0.525-1.120 |
0.170 |
||
|
Age group |
6-9 |
1.00 Baseline |
|
|
|
|
|
|
|
10-14 |
1.157 |
0.735-1.822 |
0.528 |
1.343 |
0.836-2.157 |
0.222 |
||
|
15-18 |
1.522 |
0.967-2.397 |
0.070 |
1.794 |
1.106-2.910 |
0.018 |
||
|
Locus of life |
Urban |
1.00 Baseline |
|
|
|
|
|
|
|
Rural |
0.539 |
0.164-1.779 |
0.311 |
|
|
|
||
|
Father’s education |
Primary school |
1.00 Baseline |
|
|
|
|
|
|
|
High school |
4.110 |
0.913-18.493 |
0.066 |
3.379 |
0.706-16.163 |
0.127 |
||
|
Diploma |
6.133 |
1.458-25.803 |
0.013 |
5.811 |
1.219-27.707 |
0.027 |
||
|
Bachelor |
12.358 |
2.966-51.497 |
0.001 |
10.996 |
2.202-54.912 |
0.003 |
||
|
MSc or higher |
7.583 |
1.605-35.828 |
0.011 |
6.240 |
1.058-36.798 |
0.043 |
||
|
Mother’s education |
Primary school |
1.00 Baseline |
|
|
|
|
|
|
|
High school |
3.029 |
1.096-8.370 |
0.033 |
1.814 |
0.620-5.310 |
0.277 |
||
|
Diploma |
2.896 |
1.124-7.462 |
0.028 |
1.081 |
0.369-3.170 |
0.887 |
||
|
Bachelor |
5.114 |
1.988-13.154 |
0.001 |
1.358 |
0.435-4.240 |
0.598 |
||
|
Msc or higher |
6.722 |
2.189-20.646 |
0.001 |
1.720 |
0.433-6.839 |
0.441 |
||
|
Father job |
Public sector |
1.00 Baseline |
|
|
|
|
|
|
|
Private sector |
0.751 |
0.517-1.092 |
0.134 |
1.225 |
0.788-1.904 |
0.367 |
||
|
unemployed |
0.391 |
0.090-1.693 |
0.209 |
0.795 |
0.172-3.661 |
0.768 |
||
|
Mother job |
Public sector |
1.00 Baseline |
|
|
|
|
|
|
|
Private sector |
0.430 |
0.167-1.105 |
0.080 |
0.572 |
0.205-1.591 |
0.284 |
||
|
Unemployed (Housewife) |
0.386 |
0.246-0.605 |
<0.0001 |
0.582 |
0.324-1.048 |
0.071 |
||
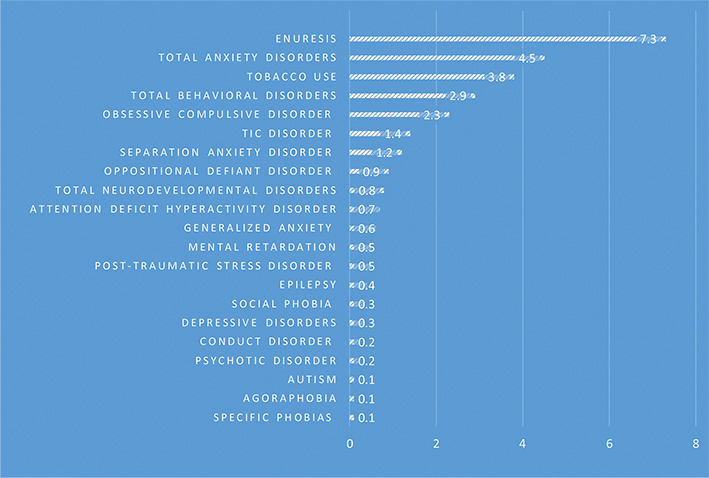
The most commonly diagnosed disorder was enuresis (7.3%) followed by anxiety disorders (4.5%), tobacco use (3.8%) and behavioral disorders (2.9%) (Table 3, Figure 1).
Table 3. Prevalence of Psychiatric Disorders in the Alborz province children and adolescents (6-18 years old)
|
Psychiatric Disorders |
Number |
Percent |
CI (95%) |
|
|
Depressive Disorders |
3 |
0.3 |
0.1-0.9 |
|
|
Psychotic disorder |
2 |
0.2 |
0.06-0.7 |
|
|
Anxiety disorders |
Separation Anxiety Disorder |
12 |
1.2 |
0.7-2.1 |
|
Social Phobia |
3 |
0.3 |
0.1-0.9 |
|
|
Specific Phobias |
1 |
0.1 |
0.02-0.6 |
|
|
Agoraphobia |
1 |
0.1 |
0.02-0.6 |
|
|
Generalized Anxiety |
6 |
0.6 |
0.3-1.3 |
|
|
Obsessive Compulsive Disorder |
23 |
2.3 |
1.5-3.4 |
|
|
Post-Traumatic Stress Disorder |
5 |
0.5 |
0.2-1.2 |
|
|
Total Anxiety Disorders |
45 |
4.5 |
3.3-5.9 |
|
|
Behavioral Disorders |
Attention Deficit Hyperactivity Disorder |
7 |
0.7 |
0.3-1.4 |
|
Oppositional Defiant Disorder |
9 |
0.9 |
0.5-1.7 |
|
|
Conduct Disorder |
2 |
0.2 |
0.06-0.7 |
|
|
Tic Disorder |
14 |
1.4 |
14 |
|
|
Total Behavioral Disorders |
29 |
2.9 |
0.8-2.3 |
|
|
Neurodevelopmental disorders |
Mental retardation |
5 |
0.5 |
0.2-1.2 |
|
Autism |
1 |
0.1 |
0.02-0.6 |
|
|
Epilepsy |
4 |
0.4 |
0.2-1.02 |
|
|
Total Neurodevelopmental disorders |
8 |
0.8 |
0.4-1.6 |
|
|
Tobacco use |
38 |
3.8 |
2.8-5.1 |
|
|
Enuresis |
74 |
7.3 |
5.9-9.1 |
|
|
Total Psychiatric disorders |
136 |
13.5 |
11.4-15.6 |
|
The most common conditions in the subgroup of anxiety disorders were obsessive compulsive disorder (2.35%) and separation anxiety disorder (1.2%). In the subgroup of behavioral disorders, the most common conditions were tic disorder (1.4%) and oppositional defiant disorder (0.9%).
Over all, the prevalence of mental health disorders in the subgroups was enuresis (7.3%), tobacco use (3.8%), obsessive compulsive disorder (2.3%) and tic disorder (1.4%) (Table 3).
Findings show that the elimination, anxiety and behavioral disorders had the highest comorbidity with other psychiatric disorders. Elimination and anxiety disorders had the highest comorbidity with behavioral disorders (10.8%) and substance abuse disorders (13.3%), respectively (Table 4).
Table 4. Comorbidity disorders according to the type of psychiatric disorder in the Alborz province
|
Psychotic Disorder |
Elimination Disorders F(P) |
Substance abuse disorders F(P) |
Neurodevelopmental disorders F(P) |
Behavioral Disorders F(P) |
Anxiety Disorders F(P) |
Mood Disorders F (P) |
Comorbid disorder Main disorder |
|
0 |
1 |
3 |
0 |
0 |
2 |
|
Mood Disorders |
|
1(2.2) |
5(11.1) |
6(13.3) |
0 |
5(11.1) |
|
2(4.4) |
Anxiety Disorders |
|
1(3.4) |
8(27.6) |
4(13.8) |
1(3.4) |
|
5(17.2) |
0 |
Behavioral Disorders |
|
0 |
2(25) |
0 |
|
1(12.5) |
0 |
0 |
Neurodevelopmental disorders |
|
1(2.6) |
5(13.2) |
|
0 |
4(10.5) |
5(15.8) |
3(7.9) |
Substance abuse disorders |
|
0 |
|
5(6.8) |
2(2.7) |
8(10.8) |
5(6.8) |
1(1.4) |
Elimination Disorders |
|
|
0 |
1 |
0 |
1 |
1 |
0 |
Psychotic Disorder |
Discussion
In this study, we evaluated the mental health profile among children and adolescents from the province of Alborz. We also examined the role of demographic factors in the prevalence of psychiatric disorders among them. In this study, the co-morbidity of psychiatric disorders was also evaluated.
In a study by Mohammadi et al in 2013 on the prevalence of psychiatric disorders among Iranian adolescents, the overall prevalence was reported to be 14.2%, which varied among different provinces. Conduct disorder was also reported as the most common condition (24%) out of all disorders9. In our study, the overall prevalence of psychiatric disorders in children and adolescents was found to be 13.5%, which is close to what claimed by Mohammadi in 2013.
In another study by Mohammadi et al in 2005, the prevalence was reported to be 10.8% and the most common disorder was anxiety disorder (8.35%)15. We found a greater prevalence of mental disturbances in our survey than in Mohammadi’s study in 2005. This may be due to clear socioeconomic changes and the expansion of urbanization and its concomitant effect.
Alavi and colleagues in 2010 evaluated the prevalence of psychiatric disorders among children aged 7-12 years in urban areas of Tehran, and the overall prevalence that they found was 17.5% and the most common disorder was attention deficit /hyper active disorder16.
Also, in Shahrivar’s 2008 study in Tehran, the prevalence of these disorders among adolescents between 12 to 17 years old was 14.2%17.
The lower prevalence of psychiatric disorders in Alborz province can be attributed to the lower complexity of the current urbanization, for example frameworks extending media and its negative effects is less than Tehran province in Alborz.
From other provincial studies, there is a study by Saif Hashemi et al in 2012 that investigated the prevalence of mental health disorders among 6-12 year-old children living in urban areas of Semnan Province. They reported a general prevalence of 9.6% for mental disorders18.
We suggest that the higher prevalence of mental disorders in the province of Alborz in our study could be due to the impact of the proximity of the Alborz Province to the metropolitan of Tehran and the cultural diversity and the related problems. The weaker economic condition in Alborz province, could be another reason by lowering the quality of health services.
In a systemic review article by Malhotra et al in 2014, the prevalence of psychiatric disorders in the general population of children and adolescents in India was reported as 6.46%19.
The higher prevalence of psychiatric disorders in our study compared with theirs can be attributed to the acceleration of urbanization and the intensification of social problems and economic challenges in the province of Alborz over the past few years.
In a study by Molafo and colleagues in 2012, the prevalence of psychiatric disorders among Lebanese adolescents was investigated and they reported a prevalence of 26.1% for all mental conditions, while similar to our study they reported anxiety disorders to have the highest prevalence (13.6%). The most important reasons for the difference in the prevalence between two studies are probability caused by the decades of war and the instability of health policies20.
The prevalence of mental disorders from an Egyptian study on children, was 20.6% that was based on the parents’ point of views. This was higher than ours21, and we suggest that different methodologies were the actual reason of it.
In 2012, Cortina et al evaluated the prevalence of mental health problems in sub-Saharan Africa by using a systematic review study. They reported a general prevalence of 14.3% based on clinical diagnostic tools and 19.8% based on screening questionnaires. They also investigated the relationship between sociodemographic factors and psychopathology22.
This indicates a higher prevalence of psychiatric disorders in this population compared to our study (19.8% vs 13.5%). As the study suggests, socioeconomic differences are one of the important factors influencing this difference in prevalence.
In 2007 , Syed et al form Pakistan investigated the prevalence of psychiatric disorders among school children aged 5 to 11 years old. They claimed a prevalence of 34%, which is clearly higher than the results of our study. The difference in socio-cultural structures between two countries and the differences in mental health policies and the levels of implementation of the policies can cause the difference in prevalence23.
In our study, the most common psychiatric disorder was urinary incontinence (7.3%) followed by anxiety disorders (4.5%). Obsessive-compulsive disorder was the most prevalent condition in the subgroup of anxiety disorders (2.3%) (due to DSM 4 criteria).
In some sources, the prevalence of urinary incontinence, has been reported differently according to the age of children. The prevalence of urinary incontinence was differs by children’s age. The prevalence has been reported 1.5-5% in children aged 9 to 10 years and about 1% in adolescents aged 15 years24 that in our study, there is a slight increase in the prevalence.
Although there is no obvious correlation between urinary incontinence and psychiatric disorders, the probability of behavioral and developmental problems in children with urinary incontinence is more than other children24, which needs more accurate attention and evaluation of children with urinary incontinence.
Eszupur et al in 2015 reported the prevalence of urinary incontinence in children aged 5 to 17 years old in southern Nigeria to be 24.4%25.The reason of high prevalence of this disorder can be the impact of socioeconomic factors and less availability to medical treatment in developing countries.
Another study in 2012, Alkot et al reported a prevalence of 11.5% for urinary incontinence among students aged 6-18 years in Menofia governorate in Egypt. They suggested an urgent need for therapeutic measures, especially in developing countries26.
Another common psychiatric disorder in our study was tobacco use (3.8%), which is a major cause of chronic diseases and death27. The association between the use of cigarettes and mental illness is well known28. According to a study by Sheikh et al from Morocco, the prevalence of tobacco use among adolescents aged 13-15 over the period 2006-10 was increased from 3 to 5%29. Our study showed that tobacco use with a prevalence of 3.8% to be the second psychiatric disorder. This show the urgent need to pay serious attention for the controlling programs and increasing.
Establishing the conditions for quitting smoking and focusing on the positive outcomes of its abandonment are among the issues of improving health indicators in the last few years30.
There have been many reports of comorbidity of anxiety disorders with other psychiatric disorders in children and adolescents31,32. In our study, anxiety disorders were one of the most comorbid disorders with others (Table 4) that shows the need of paying more attention to identifying and treating anxiety disorders along with other mental conditionsin children and adolescents.
Conclusion
Our study shows that the prevalence of mental health problems among youth in Alborz province is similar to other previous studies from developing countries. Considering the high prevalence of enuresis, anxiety disorders and tobacco abuse among children and adolescents living in Alborz province, it is recommended to produce effective policies for management of enuresis, prevention and treatment of anxiety disorders and decreasing the rate of tobacco abuse in adolescents in the Alborz province.
Limitations
We believe that the sample selection from children aged 6 and over, may not be able to reflect the disorders of all age groups of children and adolescents. To resolve this limitation, we can extent our study to all age groups of children and adolescents in future studies.
Acknowledgments
This study was supported by the National Institute for Medical Research Development (NIMAD) (code IR.NIMAD.REC.1395.001). Alborz University of Medical Sciences and Psychiatry and Psychology Research Center of Tehran University of Medical Sciences also participated in the project. We thank all the interviewees who participated in this study. We also thank all the participating families for their cooperation.
Conflict of Interest
No conflict of interest.
Funding
This work was supported by the National Institute for Medical Research Development (NIMAD) (Grant No. 940906).