Document Type : Review article
Background: Community-based interventions can be effective due to the active participations of communities in pre- and post-disaster planning and management. Effective community-based disaster management for health promotion can be achieved by learning from the successful local and international experiences of community participations. Thus, this study is aimed to identify the community active participation approaches which were effective in promoting the health of disaster-affected communities.
Methods: This systematic review was conducted and reported based on PRISMA guideline. Web of Sciences, PubMed and Scopus were searched using the selected keywords. The inclusion criteria were all forms of published articles which studied the approaches of community active participations for improving their health in disasters. The selection of articles was conducted using the titles and abstracts. Data analysis was done based on the categorization of different community-based disaster management approaches.
Results: 10 articles were finally selected out of 2843 documents generated by initial search. Asian countries considered community involvements in disaster management the most (40%). The most community active participations in disaster management were conducted in the recovery phase (80%). Approaches of community-based disaster management for the health promotion were two-way university-community participation, focusing on empowering specific community groups, governance, and localizing community participation as well as strengthening social networks.
Conclusion: Considering the capacities of academic institutions for active participation in community-based disaster management according to the Yokohama, Hyogo and Sendai Framework is highly suggested. Further research is needed to explore the challenges of community communication and information in disasters.
Keywords: Active participation, Community, Disaster management, Health
Introduction
Reducing the vulnerability and improving the capacities of at-risk communities are important measures of the community-based approach to disaster management (1,2). Based on this approach, participations of the community members in planning and implementing disaster risk management is a main criterion (3,4). The community uses a significant amount of its skills, abilities, and resources for managing disasters before, during, and after crisis (2,4,5). Community-based disaster management approach offers less bureaucracy and more flexibility due to the participations of community members, volunteers and Non-Governmental Organizations (NGOs). Thus, the community-based affairs are usually conducted more quickly (3,6). Furthermore, the community participation is more cost-effective approach rather than government management since such voluntary activities of people and NGOs can provide some financial resources, equipment and manpower needed for disaster management (7-10).
Community participations in disaster management can be changed from passive participation to active one (11). Community-based interventions can be effective due to the active participations of communities in pre- and post-disaster planning and management (11). On the other hand, there are important challenges in community-based participations including lack of national laws on activity and accountability, insufficient knowledge and facilities, poor communication and information, lack of coordination between communities and government sections, doubled and parallel disaster management actions, competition for access to the limited resources, and lack of efficiency and productivity (6,11-17).
Community-based disaster management has been increasingly considered at international levels. Promoting the participation of local communities in disaster risk management has been emphasized in the Yokohama strategy as well as the Hyogo and Sendai frameworks (1,18,19). The Yokohama’s strategy focuses on strengthening vulnerable groups and their capacity-building at all phases of crisis management as well as transferring local experiences, knowledge and culture. On the other hand, the Hyogo and Sendai frameworks emphasize the one-way flow of knowledge from experts towards local communities as recipients of assistance (1,18-20).
Table 1. Example of applied search syntax in PubMed database
|
Database |
Search syntax |
|
PubMed
|
((Community[tiab]) OR (Communities[tiab]) OR (Community-Based[tiab]) OR (Communities-Based[tiab]) OR (“Community Engagement”[tiab]) OR (“Communities Engagement”[tiab]) OR (“Community Involvement”[tiab]) OR (“Communities Involvement”[tiab]) OR (“Community Involvements”[tiab]) OR (“Communities Involvements”[tiab]) OR (“Community Participation”[tiab]) OR (“Communities Participation”[tiab]) OR (“people Engagement”[tiab]) OR (“people Involvement”[tiab]) OR (“people Involvements”[tiab]) OR (“people Participation”[tiab]) OR (“public Engagement”[tiab]) OR (“public Involvement”[tiab]) OR (“public Involvements”[tiab]) OR (“public Participation”[tiab]) OR (“population Engagement”[tiab]) OR (“population Involvement”[tiab]) OR (“population Involvements”[tiab]) OR (“population Participation”[tiab]) OR (“local Participation”[tiab]) OR (“local Engagement”[tiab]) OR (“local Involvement”[tiab]) OR (“local Involvements”[tiab])) AND ((Health[tiab]) OR (Healthcare[tiab])) AND ((Disaster[tiab]) OR (Disasters[tiab]) OR (Crisis[tiab]) OR (Crises[tiab]) OR (earthquake[tiab]) OR (earthquakes[tiab]) OR (Flood[tiab]) OR (Floods[tiab]) OR (Drought[tiab])) AND ((“Disaster Management”[tiab]) OR (“Disasters Management”[tiab]) OR (“Disaster Prevention”[tiab]) OR (“Disasters Prevention”[tiab]) OR (“Disaster Mitigation”[tiab]) OR (“Disasters Mitigation”[tiab]) OR (“Disaster Preparedness”[tiab]) OR (“Disasters Preparedness”[tiab]) OR (“Disaster Response”[tiab]) OR (“Disasters Response”[tiab]) OR (“Disaster Recovery”[tiab]) OR (“Disasters Recovery”[tiab]) OR (“Crisis Management”[tiab]) OR (“Crises Management”[tiab]) OR (“Crisis Prevention”[tiab]) OR (“Crises Prevention”[tiab]) OR (“Crisis Mitigation”[tiab]) OR (“Crises Mitigation”[tiab]) OR (“Crisis Preparedness”[tiab]) OR (“Crises Preparedness”[tiab]) OR (“Crisis Response”[tiab]) OR (“Crises Response”[tiab]) OR (“Crisis Recovery”[tiab]) OR (“Crises Recovery”[tiab]) OR (“Emergency Management”[tiab]) OR (“Emergencies Management”[tiab])) AND (2000/01/01:2020/12/31[dp]) |
Effective community-based disaster management for improving the health of disaster-affected people can be achieved by learning from the successful local and international experiences of community participations. Such lessons can be helpful in identifying the issues and challenges of community-based disaster plans and management. Thus, the present systematic review is aimed to identify the community participation approaches which have been effective in promoting the health of disaster-affected communities. Accordingly, various dimensions of community-based approach to disaster management was determined to help researchers, policy makers and managers for development of effective health promotion plans and policies.
Materials and Methods
This study was a systematic review which was designed and implemented based on the PRISMA protocol. The databases and the search strategy as well as inclusion and exclusion criteria were determined according to this protocol. Then, after the initial search, screening and selection of articles, the quality appraisal of the selected articles was performed and finally the data were extracted and analyzed.
Databases
ISI Web of Sciences, Scopus, and PubMed databases were searched to find the related articles. The keywords were selected using the experts’ opinions as well as relevant articles, documents, and references. The final search strategy was applied based on the framework of each database using AND/OR operators (Table 1). The databases were searched from January 1, 2000 to December 31, 2020. The keywords included Community, Community-Based, Community/ people/ public/ population Engagement/Involvement/ Participation, Health, Healthcare, Disaster, Crises, Emergency, Disasters Management, Disasters, Prevention/ Mitigation/ Preparedness/ Response/ Recovery, earthquake/ Flood/Drought.
The research team applied inclusion and exclusion criteria to select the relevant studies, as the following:
Inclusion criteria
- All forms of the published articles
- Disaster due to natural hazards
- Community-based studies include health services in the disaster management phases
- Community-based studies focused on active participation of community members or various NGOs in providing services during the disaster management phases.
Exclusion criteria
- Disaster due to man-made hazards
- Studies in which people or NGOs did not participate and were merely samples of research (e.g., filling the questionnaires)
- Studies on the participation of healthcare providers in the provision of health services during disaster management phases
- Animal health or veterinary services
- Non-English language articles
Selection of studies
Resources from the initial search of the databases were collected using EndNote 7 software. After removing duplicate articles, the documents were screened based on the title and abstract as well as inclusion and exclusion criteria. Accordingly, the articles that met inclusion criteria were selected and the studies which met one of the exclusion criteria were removed from the study. Two researchers separately investigated and analyzed the full text of the selected articles for the final decision. Conflicted articles were finalized by a third independent researcher.
Quality appraisal
To evaluate the quality of articles, the critical appraisal checklists were used for the observational studies. Other types of articles that did not have a valid evaluation checklist were evaluated by a researcher-made checklist. The final selected articles were subjected to a preliminary analysis and the information form consisting of 4 sections of setting, study design, findings and implication was compiled for all the articles. All the data were extracted in the form of tables containing title, year of publication, participating group, type of hazard and their frequency and evaluated by the research team members.
Results
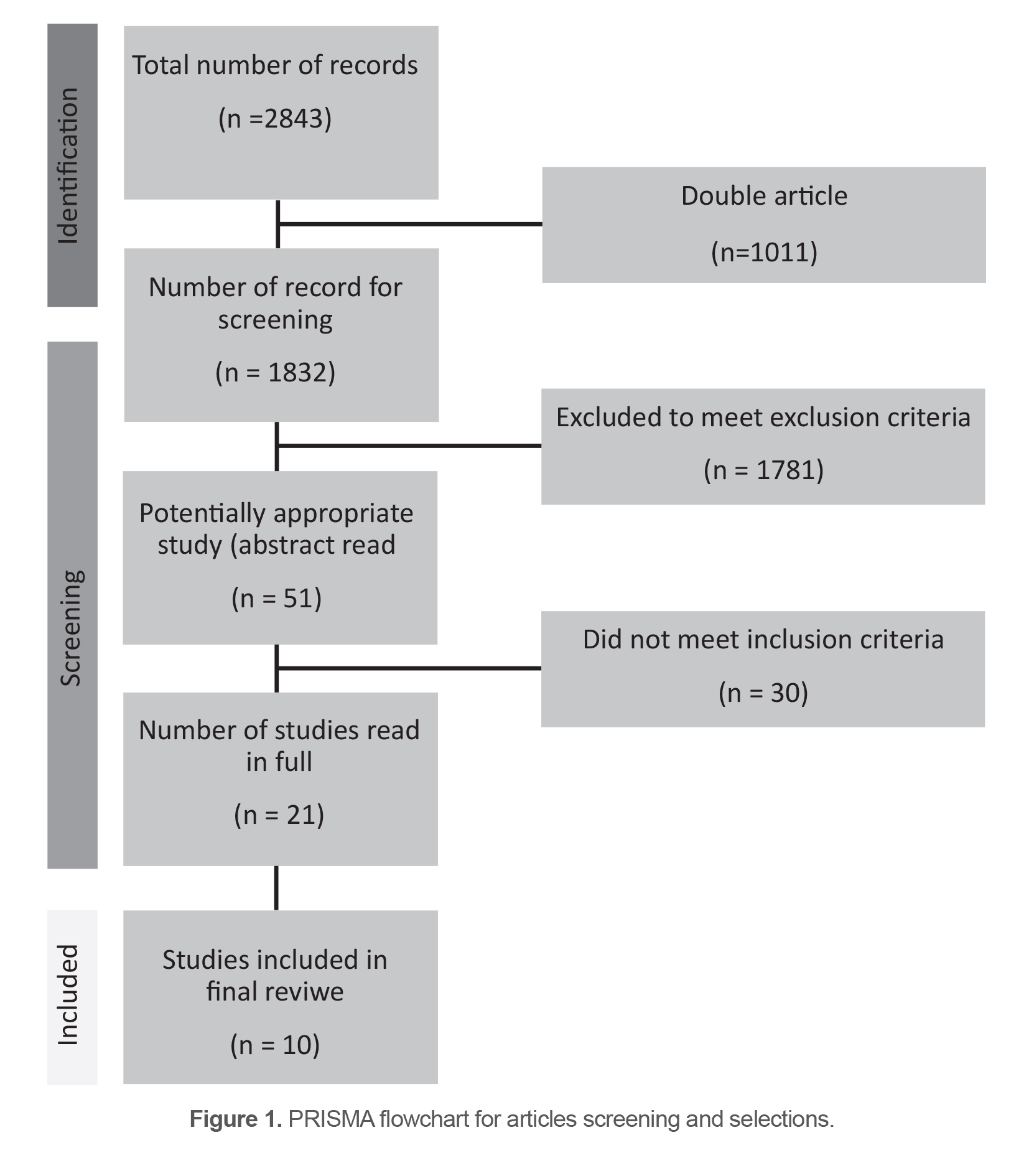
A number of (2843) relevant references were generated through initial search. After removing duplicate references, 1832 articles were considered for screening. At this stage, the title and abstracts of references were read and 1781 papers were eliminated due to meeting the exclusion criteria. The full-text of the remaining 51 articles was read and after assessment of the articles by critical appraisal tools, 10 studies were selected for final analysis (Figure 1). All the studies which used community members as research samples or conducted any intervention defined by researchers in community settings were excluded.
Description of the included studies
The included references were studied and the community active participation and involvement for the health promotion were reported in natural disaster. All the selected articles were published between 2006 and 2020. The settings of the research included different developed and developing countries (Table 2). Of these, Asian countries considered community involvements in their health improvement during disaster management the most (40%). Various groups of communities participated and involved in disaster management including NGOs, Faith-Based Organizations (FBOs), youths and elderly people as well as rural communities. Of these, local/rural communities were the most ones involved in their disaster management affairs (50%). In addition, the most community participations in disaster management were conducted in the recovery phase (80%) and 20% of the involvements were done in preparedness and 40% in response stage of disaster management (Table 3).
Table 2. The characteristics of the final selected articles
|
Title |
Year |
Setting |
Participatory group |
Disaster/hazard type |
|
How community gardens may contribute to community resilience following an earthquake |
2019 |
New Zealand |
Gardener |
Earthquake |
|
Rationale and methods for a cross-sectional study of mental health and wellbeing following river flooding in rural Australia, using a community-academic partnership approach |
2019 |
Australia |
Rural community |
Flood |
|
A First Nation Framework for Emergency Planning: A Community-Based Response to the Health and Social Effects from a Flood |
2019 |
Canada |
Siksika Nation |
Flood |
|
How bonding and bridging networks contribute to disaster resilience and recovery on the Bangladeshi coast |
2014 |
Bangladesh |
Coastal villages |
Cyclone |
|
Collective action by older people in natural disasters: the Great East Japan Earthquake |
2016 |
Japan |
Elderly people |
Earthquake |
|
Community capacity-building in disaster mental health resilience: A pilot study of an academic/faith partnership model |
2012 |
USA |
Faith-based Organizations (FBOs) |
Natural disasters |
|
Understanding youth disaster recovery: The vital role of people, places, and activities |
2017 |
USA and Canada |
Youths |
Tornado, flood, wildfire |
|
Role of panchayat (Local self-government) in managing disaster in terms of reconstruction, crop protection, livestock management and health and sanitation measures |
2018 |
India |
Panchayat (Local self-government) |
Natural disasters |
|
Natural disaster management: experience of an academic institution after a 7.8 magnitude earthquake in Ecuador |
2017 |
Ecuador |
Academic institution |
Earthquake |
|
Psychosocial interventions after tsunami in Tamil Nadu, India |
2006 |
India |
NGOs |
Tsunami |
Table 3. The frequency of setting, participatory group and disaster type
|
No |
Subjects |
N |
(%) |
|
|
1 |
Setting |
USA/Canada |
3 |
30 |
|
Ecuador |
1 |
10 |
||
|
Asian countries |
4 |
40 |
||
|
Australia |
1 |
10 |
||
|
New Zealand |
1 |
10 |
||
|
2 |
Participatory group |
NGOs |
1 |
10 |
|
FBOs |
1 |
10 |
||
|
Rural/local community |
5 |
50 |
||
|
Youth/elderly people |
2 |
20 |
||
|
Academic institution |
1 |
10 |
||
|
3 |
Disaster type |
All natural disasters |
2 |
20 |
|
Flood |
2 |
20 |
||
|
Tornado/cyclone |
2 |
20 |
||
|
Earthquake/tsunami |
4 |
40 |
||
Thematic analysis
The articles of community active involvements related to their health improvement during disaster management were classified into five categories as follows:
- The approach with two-way university-community participation
- The approach focused on empowering specific groups of the community
- The governance approach
- The approach of localization of participation
- The approach focused on strengthening social networks.
The approach with two-way university community participation
Longman et al studied the population mental health through a community-academic partnership in a rural community of Australia 6 months following a severe flood in 2017. The involvement of the community was in the forms of recruiting staff from the community in the research team and establishment of two Community Advisory Groups (CAGs). Furthermore, the affected community was involved into the design, development and implementation of the study. The community experiences were applied for capturing the factors affecting mental health and well-being outcomes after floods. In addition, the community members advised research team for any voluntary role related to the well-being and mental health in the context of the flood-affected community. Involving community members into the research team led to eliminating the gap between evidence and action as well as identifying key opportunities for emergency planning, and resilience to natural hazards in rural communities (21).
Montesanti et al documented the Siksika First Nation (SFN) community-based response to the health impacts of the flood through a community-university partnership. SFN, located on the Bow River banks, is a member of the Blackfoot Confederacy and benefits from the second largest reserve land base in Canada. SFN encountered forced evacuation and displacement of about 1000 residents at the time of the flood in 2013. Siksika presented a rapid community-based response to the flood due to their frequent experiences with prior floods. Their plan included the phases of initial response, recovery, mitigation and preparedness using the indigenous knowledge about the river history and community capacities. Different aspects of determinants of health were considered in the plan including domestic and gender-based violence in the temporary shelters, mental health support groups for the displaced people and schools as well as parenting program and involvement of spiritual elders for promoting the community resilience. Thus, regarding the cooperation of the community and the university and using the knowledge and meaningful participation of the natives in planning and decision-making, a framework was accepted by the native community, policy makers and service providers (22).
Mosley A et al described an academic-faith partnership which can improve the capacity of communities at the time of disasters and other mass casualty events. The leaders of Christian-, Jewish-, and Muslim FBOs in USA were involved in designing, preparing and evaluating the train-the-trainer program to improve the individual competencies for providing psychological first aid for affected communities and community training by faculty members and key managers of several Academic Health Centers (AHC). Furthermore, the FBOs leaders and members received training for disaster planning interventions as well. This program used the established relationships between community members and FBOs leaders to improve the community resilience by partnership capacity-building approach. The outcome of this collaboration was the development and implementation of a joint daily curriculum including psychological first aid strategies and disaster-related spiritual values (23).
Cordero-Reyes et al described a disaster relief plan intervention developed by USFQ’s Medical School for the affected community. An academic institution, as a part of the local community, made a six-phase plan for addressing mental, physical and environmental health of the community after the earthquake. The management plan phases included induction phase, establishing a base camp, crisis management and mental health aid, creation of multidisciplinary teams, creation of multi-agency teams, and reconstruction. By developing multi-disciplinary teams to implement plan during response and recovery phases, the academic institution was able to provide proper health and communication infrastructure in the affected regions (24). It was a suitable example of a successful academic institution intervention in disaster management.
The approach focused on empowering specific groups of the community
Yotsui et al studied the elderly support system developed in Minamisanriku city following the Great East Japan Earthquake in 2011. Accordingly, elders were involved in the community program including visiting the temporary housing as well as daily visits of vulnerable elderly people who lost their home and livelihood. This community-based program enabled the older people to establish a strong social support for the other vulnerable elders. The study showed that social participation of older people improved their well-being and empowered the community after the earthquake. Valuable opportunities for older people’s social participations were assessed in four categories of revision of social identity, positive self-representation, ownership of life and future of the elderly, and building bridges between government institutions and social capital. This assessment showed that creating a social space for conversation and the desire of the elderly for participation increase their self-confidence and security and social relations with other generations. In addition, access to local knowledge of the elderly leads to improve welfare and power dynamics in the community (25).
On the other hand, Cox et al studied the youth experiences during the recovery phase in four disaster affected communities in Canada and USA. Accordingly, the youth (13-22 years old) were participated to workshops where they applied music, art and other methods to show their post-disaster recovery experiences. Youth experiences revealed different resources which can support their recovery after disasters. For instance, they needed social support from key adults such as parents and teachers, safe and natural spaces as well as opportunities for distraction and emotional expression in order to return to their normal lives after disasters. Safe environments such as home and school for creating a sense of stability, comfort, security and privacy can evoke positive emotions for the youth rehabilitation (26).
The governance approach
Mondal et al assessed the considerable roles of Panchayats (local self-governing institutions) in disaster management of cyclone affected regions in the West Bengal in India. Accordingly, the reconstruction of destructed houses, management of livestock, health and sanitation services as well as crop protections were the main roles played by Panchayats in the area affected by cyclone. In addition, Panchayats established and arranged health camp and temporary shelters as well as involvement in rescue actions. Based on the research findings, although Panchayats are the most suitable grass root level entities for involving people in disaster preparedness, their functions were evaluated as poor after the cyclone due to inadequate involvement of villagers’ representative (27).
The approach of localizing the participations
Vijaykumar et al reported the roles of two NGOs for providing psychosocial services for tsunami-affected regions in India. Accordingly, the NGOs roles were influenced by two challenges including lack of being familiar with the native language, especially among two groups of students, and non-native volunteer staff. They used training materials for training volunteers in order to handle the survivors’ mental health needs. One NGO prepared educational materials and videos and trained volunteers and native people with strong ties to the community. This educational approach led to being aware of local customs, language and culture, and working continuously in the region. A training manual and training program for teachers, youth, and other field staff were developed by second NGO to provide interventions. In addition, the community members were involved in the psychosocial activities. For example, women were participated in the actions such as drawing and sewing. Sports such as cricket, football and volleyball were organized and held for all community groups (28).
The approach focused on strengthening social networks
Islam and Walkerden investigated the contribution of bonding and bridging networks in the recovery of two Bangladesh villages affected by Cyclone Sidr. Accordingly, bonding (family and relatives) and bridging (neighbors and friends) were applied for handling the disaster during the initial response phase. Such supports included emotional care, shelter and food sharing, helping in reconstruction and collaborative affairs. However, bridging network was broken down during recovery phase and needed the involvements of NGOs and community-based organizations for long-term recovery. The difference between social networks in short-term and long-term rehabilitations, the situation of population growth, poverty and vulnerability and resilience of the target population were considered by the researchers. For example, the role of social networks in bonding and bridge relationships during short-term rehabilitation included search and rescue, food and temporary shelter, medical assistance, creating communication channels, and emotional support. Livelihood support, development and reconstruction, loans and grants were mentioned as long-term rehabilitation measures (29).
Shimpo et al studied the roles of an established community garden in New Zealand following the 2010-2011 earthquakes. The garden was established in 2005 and funded from different sources including NGOs. The gardeners are the community volunteers who use the common space for growing flowers and vegetables. Providing a safe place for physical actions and social interaction which increased after the earthquakes was obtained as one of the important roles played by the garden in life of the local residents. In other words, the socializing and meeting people were the major motivators which attracted the volunteers to the garden following the earthquakes. At the times of disasters, the social garden plays important roles not only in improving resilience but also in effective rehabilitation of the community through increasing social functions. These safe gathering places reduced the stress of people by keeping them busy and providing opportunities for social bonds between local residents and new individuals. Due to less damage to green outdoor space than building infrastructure, the promotion of resilience is achieved by planning social activities in social gardens, supporting social capital and self-management (30).
Discussion
According to our findings, 5 approaches of community-based disaster management which were effective for the health promotion of the affected people were extracted from the data including approaches with two-way university-community participation, focusing on empowering specific community groups, governance, and localizing community participation as well as strengthening social networks. The approaches have been discussed according to the Sendai and Hyogo frameworks as well as Yokohama strategy.
The approach with two-way university-community participation
Participations between universities and rural communities were considered as an important approach in the literature (21-24). Accordingly, both the Hyogo Framework’s strategies for transferring knowledge to local communities as well as the Yokohama’s strategy for improving the self-confidence of local people and respecting their values and culture have highlighted the community-based approach in disasters (1,20). Although promoting the participation of local communities with considering their knowledge has always been emphasized by the Yokohama strategy and Hyogo and Sendai frameworks, types of these participations differ (20). While the Yokohama’s strategy considers strengthening and empowering vulnerable groups in all phases of disaster management, Hyogo and Sendai Frameworks emphasize the one-way flow of knowledge from experts to local communities as “recipients of assistance” (20). Based on the IFRC study, communities have not been effectively involved in disasters’ decision-making (31). UNISDR suggested mapping the local hazards, interactive communication between national and local stakeholders, and community-based planning approach (32). The combination of transferring knowledge to local communities and community participations in disaster management can provide unique opportunities for improving the resilience of poor communities (1,18,20,21).
Community-based disaster planning in local communities have been neglected around the world (22). Insufficient research on community-based disaster management with failure to meet the diverse needs of people in preparedness and response plans were reported as important issues (22). In accordance with our findings, both Hyogo and Yokohama strategies focused on community-based preparedness and response using the participations of local people and NGOs (1,18,20).
One study found that since FBO had the three criteria of regular and direct contact with target communities, reliable leaders, and the ability to mobilize the community covered in support of a particular issue, are suitable as a bridge to link affected community members to mental health professionals (23). This study also demonstrated that in a decentralized approach, by replacing mental health professionals with native and sustainable resources of the faith community and the surrounding social networks, preparedness and responsiveness to community disasters is improved (23). In this study, a combination of the Hyogo Framework solution was done in the form of providing training to religious leaders of faith-based organizations and the Yokohama strategy in the form of selecting organizations based on willingness and ability to participate, training desirability, sustainability in activating and employing volunteers aimed to increase individual competencies of leaders, members and people (1,20).
Another study illustrated the participatory role of the academic institution as a community unit in crisis management (24). This combination for the Hyogo Framework solution was done in the form of developing a disaster preparedness culture in government agencies, the public, the media, and especially academia, and for Yokohama’s strategy in the form of strengthening independence, participatory decision-making, and community participation by building and enhancing capacity and resilience against disasters through encouraging and uniting survivors to overcome their problems (1,18,20). We can conclude that universities play important roles to collect and process local knowledge and then, merge them with modern knowledge. This can lead to achieve sustainable and cost-effective solutions for protecting communities against disasters. Universities need to actively focus on disaster risk reduction, preparedness and recovery plans with the participations of local communities. On the other hand, using the internal resources of universities can help provide necessary services for communities in different phases of disaster management such as basic needs, medical, health and educational services (24). In this regard, based on a study on the college’s earthquake preparedness, the findings showed weak earthquake preparedness. In addition, the SWOT analysis has demonstrated that external factors such as opportunities and threats had a stronger effect than strengths and weaknesses as internal factors on college preparedness (33).
The approach focused on empowering specific groups of the community
According to the findings, although the elderly suffered from physical disabilities, their knowledge, experiences and cognitive capacities can be applied for survivors’ rehabilitation and resilience (25). Accordingly, the Sendai Framework emphasizes the participation of the elderly in policy-making and planning and considers them as valuable social capitals with effective experiences and skills (19,20). This can change the stereotypical image of the elderly as a vulnerable dependent population to the important social group that can take useful steps for optimum use of local resources (34).
On the other hand, supportive people, places and activities can facilitate the rehabilitation of the youth after disasters (26). For example, doing artistic activities strengthened the youth positive emotions, reduced their stress and empowered them in disasters (26). In accordance with this study, Sendai Framework mentions the important roles of children and the youth as the factors of change and emphasizes the necessary conditions, education and space for their participation in disaster risk reduction (19,20).
The governance approach
Based on the findings, specific problems in rural areas can be effectively addressed by the local community (270. However, the role of self-governing institutions in disaster management was insufficiently assessed and the need to change from a response-based approach to prevention-based approach was emphasized (27). Accordingly, Sendai Framework considers the importance of strengthening disaster risk governance by assigning roles and responsibilities to local communities (19,20). It seems that the implementation of various development programs and disaster management, along with the lack of active participations of communities in decision-making can increase the costs of health programs in the recovery phase.
The approach of localizing the participations
Based on localizing the participation approach, a large part of community can be covered by simple, basic and low-cost health interventions which prevent the heavy and long-term costs of rehabilitation programs for governments and communities (28). The need for encouragement, supporting resilience measures, identifying key community personnel and organizations which were reported by the authors, confirm the effectiveness of Yokohama strategy on respecting for local experiences and values in disaster health recovery management. This is in accordance with the effectiveness of Hyogo Framework in active participation of communities, especially volunteer activities as well as the effectiveness of Sendai Framework in using experiences and traditional knowledge of local peoples for development and implementation of risk reduction plans (1,18-20).
The approach focused on strengthening social networks
Social networks consisting of bonds have strong strength and stability in short-term and long-term post-disaster rehabilitation (29). Although social networks including bridge relationships (relationships with neighbors and friends), are suitable for short-term rehabilitation, it cannot work in long-term rehabilitation due to competition for access to resources (29). This study is consistent with Yokohama strategy which focuses on networking to increase disaster prevention and mitigation activities. Similarly, Hyogo Framework emphasizes promoting community participation through specific policies, and strengthening networking. Sendai Framework highlights building social centers in order to improve public awareness for rescue and relief activities (1,18-20). It seems that the provision and distribution of humanitarian aid in affected communities can lead to increase or decrease in competition for access to resources and thus play important roles in weakening or strengthening social networks.
Based on the findings, garden space positively affected the social environment due to encouraging people to communicate and share their knowledge and experiences. In addition, gardens were used as a source of food after the earthquake (30). This study highlighted the effective participation and interaction between government and people for strengthening social networks 30. Such infrastructures can reduce the stress and improve the rehabilitation and resilience of communities due to strengthening the social communications (30). Accordingly, Sendai Framework emphasizes the establishment of community centers to improve public awareness for effective disaster response (19,20).
Conclusion
Considering community-based approaches in disaster management can help improve the health of disaster-affected people through five concepts of two-way university-community participation, empowering specific groups of community, localizing participation and strengthening social networks. However, the governance approach can have a negative impact on the effective participation of community in disaster management.
Exploring challenges and factors which affect the community-based disaster management can help researchers, policy makers and managers to establish effective community’s active participation in disaster management systems. Considering the capacities of academic institutions for active participation in community-based disaster management according to the Yokohama, Hyogo and Sendai Framework is highly suggested. NGOs and faith-based organizations can strengthen social networks and communications in disaster-prone communities. Empowering the specific groups in community for participation in disaster management and sustainable resilience of community is suggested. In addition, the capacity of the elderly and young people as valuable social capitals needs to be considered for community active participation. They should be empowered for participation in sustainable recovery and development. Further research is needed to explore the challenges of community communication and information at the time of disasters. Furthermore, more research is required to investigate the capacity-buildings of all social groups such as the elderly, the youth, women, men and children in disaster management. In addition, achieving primary healthcare coverage in the affected regions can be facilitated by community participation and involvement.
Limitations
The possibility of missing any related documents due to not publishing the results by researchers or the wide range of journals which published this topic, was the main limitation of the current review. The authors tried to include various related keywords and databases to overcome this limitation.
Ethics approval
This research was a part of a research proposal approved by Shahid Beheshti University of Medical Sciences with the ethics code of IR.SBMU.RETECH.REC.1398.402
Funding
This study was funded by Safety Promotion and Injury Prevention Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Acknowledgements
This research was a part of a research proposal approved and supported by Shahid Beheshti University of Medical Sciences with the ethics code of IR.SBMU.RETECH.REC.1398.402.
Conflict of Interest
There are no conflicts of interest/competing interests.