Document Type : Original article
Abstract
Background: Following the outbreak of coronavirus and its impact on the educational process of medical students, attention was paid to e-learning due to the importance of education and research. The aim of the present study is an evaluation of virtual and actual education models on the learning of internal interns during the COVID-19 pandemic.
Methods: The present study is a trial that was performed on 112 internal interns of hospitals from January to December 2020. Each participant was randomly assigned to one of the actual or virtual educational model groups with personal consent. Educational method was case-based discussion in both groups. The learning outcomes of the interns of these two groups were compared in 9 areas with 95% confidence level and 5% random error. Data about age, sex, type of residence (home or dormitory), pre-internship score (≤150 or >150) and entrance exam rank (≤300 or >300) were collected. Data were analyzed using SPSS Version 20.
Results: The mean ±SD age of the participants was 24.9±2.3 years, 46% of participants were men and 54% of them lived in dormitories. The results of the study show that the difference in pre-test and post-test scores with actual and virtual education models in the male and female is significantly different (p-value=0.020). Virtual education for men and actual education for women have resulted in higher difference scores in pre-test and post-test. Actual and virtual education models were not different in academic achievements of the participants. Thus, the scores obtained in 9 areas did not make a significant difference between the two types of educational models.
Conclusion:The comparison of virtual and actual education demonstrated that there is no significant difference between these two methods in student output. Given the conditions that have been created by COVID-19 in the world, it seems that the use of virtual education can be a good alternative to educating medical students so that education does not stop.
Keywords: Actual education, COVID-19, Model of learning, Virtual education
Introduction
Evaluating and inventing desirable educational models is one of the most important tasks of educational system. Development and access to internet caused expansion in the virtual education and virtual universities in the field of education (1). Following the outbreak of coronavirus and its impact on the educational process of medical students, attention was paid to electronic-learning (e-learning) due to the importance of education and research. Since social distance is the best way to prevent COVID-19, this issue definitely involves medical students as well. In this regard, medical schools, in response to COVID-19 pandemic, have tried to hold the training of this course virtually, and in some schools, clinical skills training classes have been held online. Evaluation is also carried out online. There are also challenges due to the suddenness of this change in the training process and the attention paid to web-based (virtual) distance learning.
At this time, the challenge facing medical schools is to train externs and interns and create appropriate clinical experiences for them in dealing with patients, which does not seem to be easily achieved with virtual and online training (2). Therefore, it is necessary to evaluate the courses that are presented virtually in order to better prepare educational activities in cyberspace. On the other hand, because student evaluation methods in Iran have been more face-to-face, there are shortcomings in virtual evaluation along with virtual education (3-5).
One of the main foundations of the virtual education process is the evaluation of educational outcomes. In fact, evaluation and measurement is an essential component of the educational system through which the performance of learners is observed and evaluated. Inclusive evaluation is an important part of the distance education program (6). Effective evaluation allows examining the effectiveness of the virtual teaching method and comparing it with the actual teaching method, which has been considered in the project (7).
In today’s fast-paced world, many teaching methods are slow and inefficient and do not have the power to convey new concepts to learners, thus it is necessary to use new technologies in this regard. The move to new approaches to education has led many universities around the world to use e-learning technology in their courses, and this is more important these days in the shadow of the COVID-19 pandemic (8).
Comparing the effectiveness of virtual and actual training is one of the most important design principles of virtual training. Knowing in which areas e-learning is likely to be less sufficient for learners to learn, or what factors may affect the effectiveness of e-learning, will help to establish the best e-learning practices.
Given the situation in the COVID-19 pandemic and the need to create a physical distance between people, the need to use virtual training is much more important than before. Moreover, the pandemic caused a significant decrement in hospitalized internal cases which made us simulate the case presentation sessions. In this regard, the aim of present study is to evaluate virtual and actual education models on the learning of internal interns during the COVID-19 pandemic.
Materials and Methods
The present study is a trial that was performed on 112 internal interns of hospital from January to December 2020. In each season, 28 interns were present in the internal department for 3 months, and they were randomly assigned to one of the actual or virtual educational model groups with personal consent.
Ethical committee approved all experimental protocols (approval ID:IR.IUMS.REC.1400.120). Informed consent was obtained from all subjects involved in this study.
Group 1 (actual education): 14 interns learned about internal emergencies priorities approved by the internal group with actual educational model (wearing a mask and observing physical distance). In this method, at the beginning of the class, 10 questions were displayed for interns using the online software of Porsline and WhatsApp social network, and after recording the answer by them, online graphs of correct answer percentage were drawn on the class screen without mentioning the name of the examiner. Then, the training was done in the form of case presentation (history, examination, diagnostic and treatment plans, respectively) and at the end, 10 questions were displayed for the interns again using the online software of Porsline and WhatsApp social network. The answers and online graphs of correct answer percentages were drawn on the class screen without mentioning the name of the examiner, and by comparing these two tests, students noticed an increase in their knowledge of the subject taught. During the class, the interns were asked 10 intervention questions that they had to send to the instructor using the online software Porsline and WhatsApp social network.
Group 2 (virtual education): 14 interns learned about internal emergencies priorities approved by the internal group with virtual educational model (using Adobe Connect software). As the same previous model, in this method also at the beginning of the class, 10 questions were displayed for interns using the online software of Porsline and WhatsApp social network, and after recording the answers, online graphs of correct answer percentage were drawn on the class screen without mentioning the name of the examiner. Then, the training was done in the form of case presentation (history, examination, diagnostic and treatment plans, respectively) and at the end, 10 questions were displayed for the interns again using the online software of Porsline and WhatsApp social network. The answers and online graphs of correct answer percentages were drawn on the class screen without mentioning the name of the examiner, and by comparing these two tests, students noticed an increase in their knowledge of the subject taught. During the class, the interns were asked 10 intervention questions that they had to send to the instructor using the online software Porsline and WhatsApp social network.
Educational method was case-based discussion in both groups. The learning outcomes of the interns of these two groups were compared in 9 areas with 95% confidence level and 5% random error.
Average score of multiple-choice theory test at the end of each month (Multiple Choice Theory-MCT)
Average score of descriptive theory test at the end of each month (Exam)
Average score of the recall test 10 days after the end of each month (Recall)
Average score of PMP theory test at the end of each month (PMP)
Average score of “approach to the patient” practical test based on the orders written by the interns on the patient’s bedside in the emergency ward from the course content which is held monthly (Approach)
Average score of “Hx and Ph.E” practical test based on the history and examination performed by interns on the patient’s bedside in the emergency ward which is held monthly (HxandPhE)
Average score of the interns’ survey questionnaire in each month (Form)
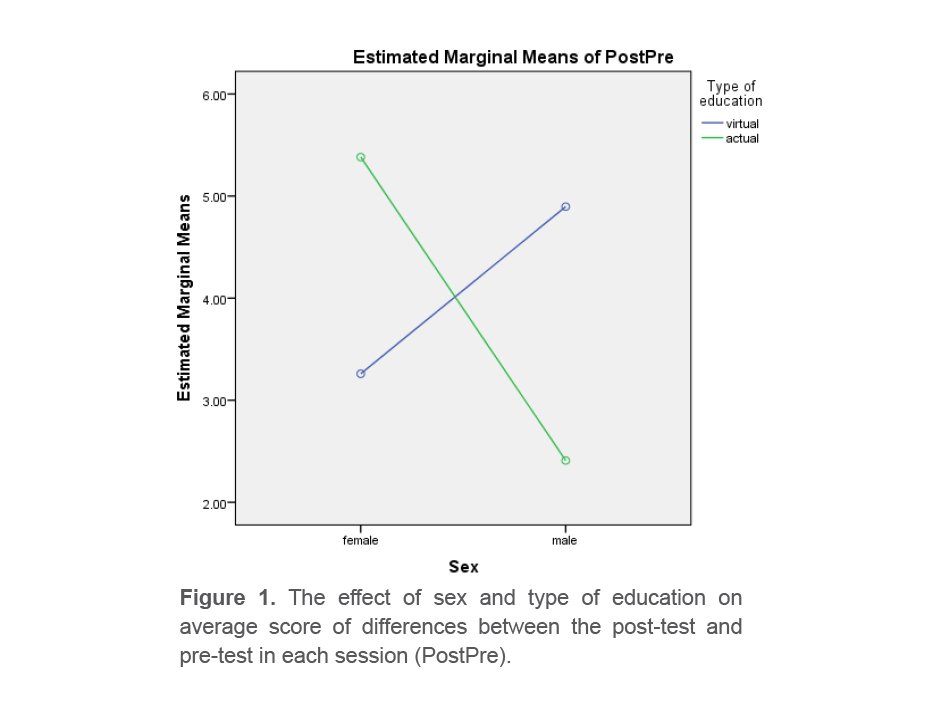
Average score of differences between the post-test and pre-test in each session (PostPre)
Average score of 10 intervention tests per session (Interactive)
Data about age, sex, type of residence (home or dormitory), pre-internship score (≤150 or >150) and entrance exam rank (≤300 or >300) were collected.
Continuous variables are reported as mean ±SD. In order to test the difference between mean of 9 test score across demographic variables, Two-way ANOVA was used. Difference between average score of 9 areas in actual and virtual models were assessed by independent sample t-test. Data were analyzed using SPSS Version 20 (IBM Corp, Armonk, NY, USA). For all statistical tests, p values ≤0.05 were considered statistically significant.
Results
The mean ±SD age of the participants was 24.9±2.3 years, 46% of participants were men and 54% of them live in dormitory. Results of the study indicate that difference in pre-test and post-test score with actual and virtual education models in the male and female is significantly different (p-value=0.020). Virtual education for men and actual education for women have resulted in higher difference scores in pre-test and post-test (Table 1).
Actual and virtual education models were no different in academic achievements of the participants. Thus, the scores obtained in 9 areas did not make a significant difference between the two types of educational models (Table 2).
A two-way ANOVA was conducted that examined the effect of age, sex, pre-internship score, entrance exam rank, accommodation type and type of education on scores obtained in 9 areas. There was an only one statistically significant interaction between the effects of sex and type of education on average score of differences between the post-test and pre-test in each session, p=0.020, (Figure 1).
Table 1. The effect of age, sex, pre-internship score, entrance exam rank, accommodation type and type of education on scores obtained in 9 areas
|
|
MCT |
Exam |
Recall |
PMP |
Approach to patient test |
Hx& PHE |
Average survey score |
Post-Pre difference |
Interactive |
|||||||||
|
Virtual |
Actual |
Virtual |
Actual |
Virtual |
Actual |
Virtual |
Actual |
Virtual |
Actual |
Virtual |
Actual |
Virtual |
Actual |
Virtual |
Actual |
Virtual |
Actual |
|
|
Age ≤25 years >25 years p-value |
75.24±21.28 73.46±21.71 70.64±20.78 71.46±23.58 0.786 |
78.31±16.56 80.56±14.76 78.36±12.92 79.53±16.49 0.873 |
67.78±25.26 68.12±24.12 66.85±22.91 63.33±27.29 0.720 |
70.59±19.02 71.41±16.89 68.92±18.08 66.60±22.45 0.697 |
71.24±19.25 70.83±19.33 64.78±23.12 66.06±21.05 0.845 |
77.26±16.11 75.68±15.47 74.14±17.66 75.53±17.56 0.673 |
83.16±16.39 78.34±16.67 72.35±21.58 80.60±17.74 0.084 |
4.35±5.36 4.39±5.01 3.35±5.81 3.73±4.71 0.879 |
74.24±15.28 73.24±15.59 72.71±14.72 70.80±17.59 0.892 |
|||||||||
|
Sex Female Male p-value |
69.33±21.64 74.76±22.23 78.48±20.80 70.09±21.91 0.098 |
74.81±16.35 80.00±16.09 81.58±14.42 80.72±13.78 0.305 |
62.26±25.70 68.61±25.17 72.48±22.65 64.09±24.65 0.120 |
67.78±18.51 72.06±18.08 72.41±18.80 67.13±19.04 0.181 |
66.55±21.42 70.76±18.99 72.48±19.04 67.68±21.12 0.243 |
74.22±16.30 77.17±15.53 78.58±16.49 73.27±16.51 0.184 |
80.44±19.24 81.11±16.16 80.48±17.61 75.59±17.67 0.411 |
3.26±5.53 5.38±5.26 4.89±5.33 2.41±3.72 0.020 |
71.18±17.01 73.20±16.33 76.34±12.70 71.63±15.86 0.261 |
|||||||||
|
Accommodation type Home Dormitory p-value |
76.28±21.44 69.52±23.04 71.85±21.75 75.30±21.32 0.222 |
82.25±14.20 80.26±15.396 74.39±16.22 80.30±14.72 0.177 |
70.46±23.04 63.04±25.81 64.64±25.96 69.48±24.20 0.196 |
73.57±17.23 67.34±19.29 66.78±19.67 72.06±17.89 0.106 |
71.96±20.06 66.91±20.93 67.28±20.55 71.39±18.95 0.233 |
79.10±16.13 73.47±15.57 73.85±16.54 77.15±16.17 0.150 |
81.03±18.69 76.30±18.54 79.89±18.11 80.78±15.55 0.404 |
4.32±4.93 4.39±5.00 3.89±5.99 4.09±4.90 0.949 |
76.14±14.66 70.95±16.52 71.57±15.29 73.72±15.82 0.218 |
|||||||||
|
Pre-internship score ≤150 >150 p-value |
63.70±20.62 64.24±2.22 81.84±18.98 78.14±20.48 0.593 |
70.04±15.23 74.24±16.43 84.53±12.96 83.91±13.19 0.383 |
55.12±24.84 56.38±26.34 76.87±19.93 73.11±21.96 0.572 |
62.16±19.56 61.71±21.60 76.18±15.67 75.17±14.37 0.933 |
60.71±20.14 62.00±19.97 76.31±17.87 74.08±18.40 0.631 |
69.83±16.12 70.38±16.64 81.46±14.99 78.80±14.77 0.592 |
77.37±19.62 74.47±18.12 82.78±17.08 81.63±15.66 0.796 |
4.04±4.89 3.38±4.53 4.15±5.90 4.71±5.11 0.546 |
67.83±17.29 68.19±16.74 78.37±11.38 75.23±15.21 0.547 |
|||||||||
|
Entrance exam rank ≤300 >300 p-value |
76.68±20.58 76.41±21.06 70.58±22.76 67.54±22.87 0.741 |
80.90±14.46 83.2912.04 74.87±16.73 75.63±18.21 0.780 |
71.62±22.92 71.14±22.63 62.12±25.95 60.18±27.13 0.876 |
74.06±15.97 72.17±18.01 65.00±20.93 66.95±19.09 0.587 |
73.93±18.63 70.91±19.89 63.87±21.29 67.45±19.74 0.388 |
80.15±15.12 76.79±15.62 71.58±17.06 73.86±16.51 0.360 |
82.53±16.97 78.67±16.77 77.70±19.84 79.36±17.31 0.418 |
3.53±5.34 3.50±4.43 4.87±5.59 5.31±5.48 0.812 |
76.34±14.37 76.08±15.53 70.54±13.44 67.18±18.38 0.597 |
|||||||||
Table 2. Difference between average score of 9 areas in actual and virtual models
|
|
Actual |
Virtual |
p-value |
|
MCT |
72.93±22.03 |
74.07±21.52 |
0.782 |
|
Exam |
78.32±15.62 |
80.28±15.10 |
0.500 |
|
Recall |
67.55±24.50 |
66.84±24.85 |
0.879 |
|
PMP |
70.18±18.64 |
70.12±18.46 |
0.988 |
|
Approach to patient test |
69.62±20.26 |
69.55±19.73 |
0.985 |
|
Hx & PHE |
76.84±16.40 |
75.64±15.90 |
0.784 |
|
Average survey score |
80.46±18.25 |
78.94±16.83 |
0.684 |
|
Post-Pre difference |
4.11±5.45 |
4.16±4.90 |
0.913 |
|
Interactive |
73.86±15.03 |
72.59±16.02 |
0.667 |
Discussion
The main finding of present study is accepting the null hypothesis that there is no difference between academic achievements of internal interns with actual and virtual education models. In the present study, we assess the learning outcomes in the 9 areas. Surprisingly, we found that different educational models had no effect on student learning. However, results of two-way ANOVA demonstrated that actual education for women and virtual education for men have resulted in higher difference scores in pre-test and post-test.
Following the COVID-19 pandemic, the need for changes in traditional teaching methods became inevitable. Virtual learning, which is mainly web-based, also brings challenges. To what extent learners can keep up with this style of teaching requires precise evaluation and comparison of this new method of teaching with actual training.
Just as actual training has its advantages, such as face-to-face communication, therefore does virtual training. Among the advantages of virtual learning, the following can be mentioned. First, this method of education allows medical students to observe and interact with patients with COVID-19 while eliminating the risk of infection. In the Hofmann et al’s study, 92.9% of the medical students agreed with the virtual methods of teaching (9). Second, virtual education provides the opportunity for other students from different parts of the world to participate and exchange information between them. One of the strengths of this mode of training is active participation of all students in clinical reasoning skills and gets a guide from tutors and peers alike. Murdock et al (10) used the virtual method for holding morning report. Participants stated that this method is an effective and suitable method for using different physician in different physical places and reduced clinical load for the medical team.
In a study conducted by the Imperial College London, interns visited patients virtually. The results of this study show that the interns eagerly attended these visits and the patients’ visits were well done without the physical presence of the patient and the doctor (11).
Like actual training, students’ learning in e-learning is related to the mastery of the teacher and the correct transmission of concepts. Results of one study showed that 97.2% of students were satisfied from virtual teaching and this method was known as the efficiency of the actual method (12). Consistent with present study, Kaur et al’s study also confirmed satisfaction of 983 medical students with virtual teaching during the COVID-19 crisis (13).
In addition to the advantages mentioned for virtual education, this educational method also has disadvantages. One of the most important weaknesses of virtual training is no access to digital technology for some students. Availability of trustworthy internet connection (14,15), hardware and software problems for virtual learning platforms (16,17), problems related to internet speed and quality (18,19), and problems with audio and video playback (20) are the other disadvantages of this mode of teaching. Besides, in some cases, the educational website may become inaccessible due to overloaded, which can make learning difficult for learners (21).
Elimination of face-to-face training and clinical examination by medical students are other weaknesses of e-learning (22,23). Results of recently published systematic review declare that progression of the competencies of a medical student were highly impacted by loss of clinical examinations, loss of bedside training and reduced direct patient care (22). Moreover, other studies have confirmed these findings (14,18,24).
The move to virtual education by means of web-based medical teaching has problems in its nature. Some of these problems can be referred to lose focus and concentration whilst sitting in front of a screen 15. Besides, reduced motivation, poor communication, physical discomfort for instance exhaustion, visual issues, and muscle and joint pain, were associated with virtual education, especially in long period (25). The lack of a real doctor-patient communication was the most important weak point in the whole subject of clinical virtual education. There are some essential behavioral regulations and communication points that can only be learnt in practice. These important principles were not directly included in the medical education curriculum and are known as the “hidden curriculum”. It seems that the virtual medical education program was not able to transfer these valuable skills to the medical students.
Another disadvantage of the virtual learning method is the lack of validity of evaluations and tests. Results of several studies showed that due to the lack of supervision during the exam, many of the scores obtained were significantly higher than the students’ academic level based on their academic records (18,21,24,25). Surprisingly, Lara et al (26) published a study whose results show that the scores obtained by 49 medical students in the Objective Structured Clinical Examination (OSCE) who participated in the teleconference were not significantly different from the scores of the same test in the form of face to face.
This study encompasses several limitations. The most important limitation is using an online method for final assessment which may raise the possibility of fraud and also lower the sensitivity of the results. Intermittent network problems and insufficient accessibility for some members were some other limitations for this study.
Conclusion
Different teaching methods have advantages and disadvantages that by recognizing the mentioned characteristics, the best of them can be selected for teaching medical students depending on condition. In the present study, the virtual and actual education methods for internal interns were examined and the results showed that there is no significant difference between these two methods in student output. Given the conditions that have been created by COVID-19 in the world, it seems that the use of virtual education can be a good alternative to educating medical students so that education does not stop.
Lessons for practice
The best methods of education for medical students should be selected based on their special conditions.
Actual teaching methods did not have priority when compared with virtual education in internal medicine courses.
Societal restrictions following the COVID-19 pandemic do not seem to lower the quality of medical education among medical students.
Acknowledgements
The authors expressed the appreciation to all interns involved in this study.
Ethics approval and consent to participate
The authors received ethical approval from Ethics Board. All guidelines were followed in accordance with ethics approval and written informed consent was obtained from all the participants prior to participation in the study.
Availability of data and materials
The datasets used during the current project are available from the corresponding author on reasonable request.
Funding
The funding agent had no role in design of the study, data collection, analysis, interpretation of data, and writing the manuscript.