Document Type : Original article
Abstract
Background: Breast cancer is a chronic disease that leads to many psychological problems that are involved in treatment and adherence to treatment. The aim of this study was to evaluate the effect of psychoeducational group intervention on psychological factors that help the patients in the treatment process.
Methods: In this study, 80 patients were selected by using convenience sampling at Imam Khomeini Hospital. They were randomly allocated either to the intervention group or to the control group. All participants completed the questionnaires of post-traumatic growth, quality of life, subjective well-being, adherence to treatment and social support. The results were analyzed by SPSS-18 software using univariate and multivariate analysis.
Results: According to the results, the applied intervention had a significant effect on post-traumatic growth as a primary outcome, and also on subjective well-being and adherence to treatment as secondary outcomes.
Conclusion: Psychoeducational group intervention in women with breast cancer can affect the treatment and provide better response to treatment through the improvement of post-traumatic growth, subjective well-being and adherence to treatment.
Keywords: Breast cancer, Educational intervention, Post traumatic growth, Randomized clinical trial
Introduction
Cancer is one of the major causes of death in the world and the third cause of death in Iran (1). Common complications of cancer, such as fear, loneliness, death anxiety, alteration in relationships, tolerance of painful medical procedures, and uncertain future may lead to distress in cancer patients (1). Breast cancer, the second most common cancer in the world (2), accounts for 25.1% of all cancers with a prevalence of 1.67 million cases worldwide (3). In Iran, breast cancer is the first diagnosis among all cancers and its incidence rate is higher than other cancers (4).
The survival rate of breast cancer has increased significantly over the past 20 years. Though most breast cancer patients face a variety of problems after treatment, they return to daily life withappropriate psychosocial interventions (2,5). However, the response to the disease may vary in some individuals and some cases require a catalyst to achieve higher levels of psychological growth. This is called post-traumatic growth, and in recent years, researchers have gradually shifted their focus from traumatic eventto positive outcomes.
The occurrence of incurable illness requires the reinforcement of positive psychological aspects of individuals and strengthening their skills in dealing with traumatic events throughout their lives. Such problems may not destroy the whole life of individuals; quite contrary, these stressful events, along with negative consequences, may bring positive consequences for their individual and social lives (6).
Several studies have investigated the necessity of psychological interventions for breast cancer patients and the role of these interventions in reducing the effect of illness on well-being and quality of life as well as facilitating post-traumatic growth. Group support, individual counseling, stress management, and psychological training are examples of psychological interventions that have been shown to have significant effects on these variables in women with breast cancer (7).
Subjective well-being is an important prognostic factor for breast cancer adherence to treatment. It refers to individuals’ assessment and perception of their quality of life, including the quality of their social, psychological, and emotional actions. In other words, subjective well-being implies how individuals evaluate their lives, including variables such as life satisfaction, marital satisfaction, positive moods, lack of depression and anxiety (8).
Social support,in particular, facilitates recovery, enhances access to medical treatment, and enhances the overall quality of life (9). A sense of social support in the face of uncertainty about life events reinforces a sense of self-control (10). Social support is considered an active stress management strategy that may reduce stress levels (11). some other studies have shown that access to social support during and after a traumatic event can reduce levels of depression, anxiety, and other physical and mental disorders among those exposed to some traumatic events (12). In relation to post-traumatic growth, social support is seen as a direct predictor of positive change after unpleasant experiences (13).
Based on existing research literature such as the studies of Shorey et al (14) and Brand et al (15), psychoeducation can increase social support. Social support can also increase post-traumatic growth, according to Scrignaro et al (16), Schroevers et al (17), and Bozo et al (18). Therefore, in this study, the role of social support as a mediator variable was examined.
Since there is no comprehensive study about any positive psychological feature that affects treatment of cancer, this study aimed to assess the effectiveness of psychoeducational group intervention on post-traumatic growth, quality of life, subjective well-being, and adherence to treatment for women with breast cancer by examining the mediating role of social support.
Materials and Methods
Study design
The present study was a randomized controlled trial. Post-traumatic growth was the primary outcome and quality of life, subjective well-being,and adherence to treatment were secondary outcomes. In addition, the mediating role of social support variable was examined.
Participants
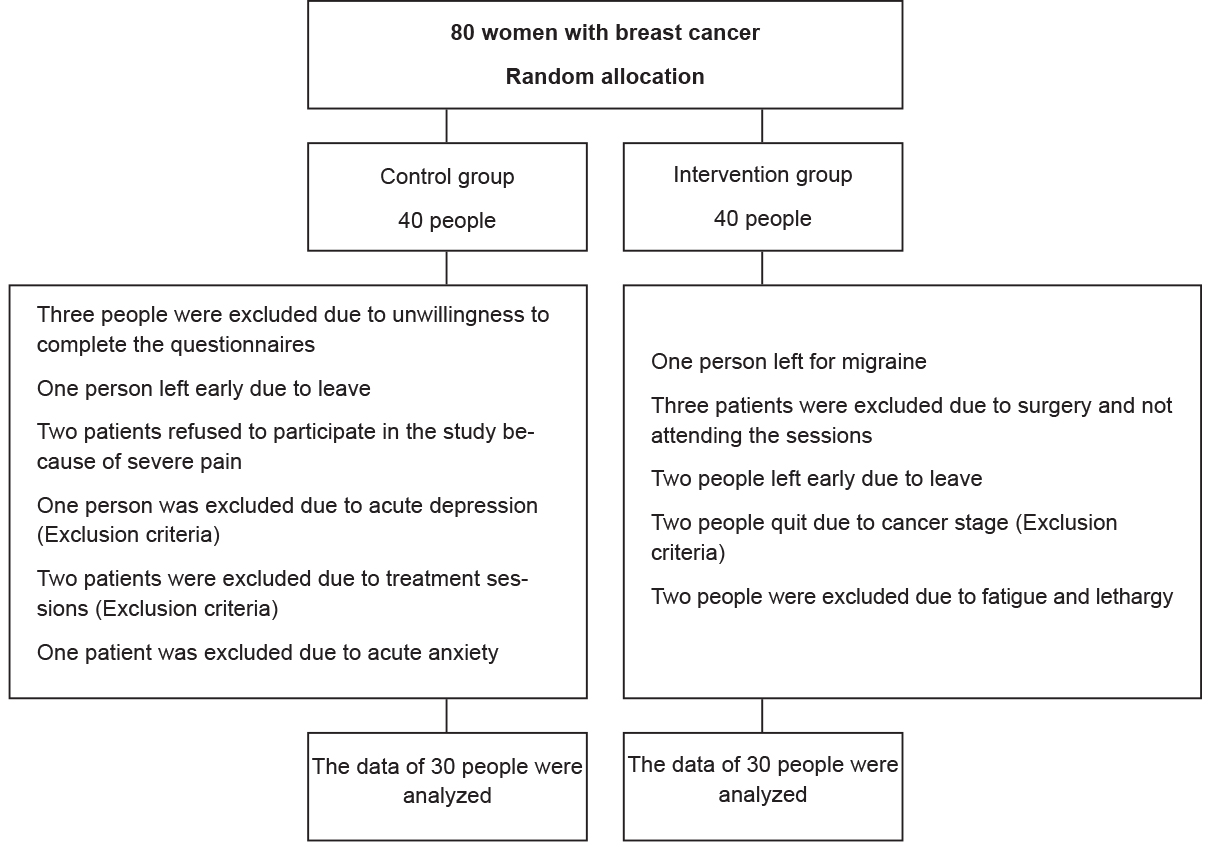
Eighty women with breast cancer at stages one and two in the 1st and 3rd wards of Cancer Institute at Imam Khomeini Hospital were selected after obtaining informed consent. The sampling method was convenience sampling. Then, they were allocated to the intervention and control groups using block randomisation. Figure 1 shows the initial number of cases and the cause of losing the individials in the final sample.
Inclusion criteria were being at least 20 years of age, cancer diagnosis by breast cancer specialist at stage 1 and 2, minimum basic literacy and willingness,and consent to participate in the study. Exclusion criteria included less than two weeks duration of illness, history of known psychiatric disorder, clinical symptoms of anxiety and depression, incomplete answering to questions, participation in some psychological intervention to alleviate the psychological symptoms associated with the disease, having a co-morbid condition or cognitive disorder.
Measurements
First, socio-demographic measures were recorded (age, education, employment, marriage status, kind of therapy, and stage of cancer). Patients completed validated Iranian versions of the following questionnaires. The Posttraumatic Growth Inventory (PTGI) developed by Tedeschi and Calhoun was used to investigate the concept of post-traumatic growth. The tool has 21 items that evaluate five areas of psychological development after facing a stressful trauma (new situations, relationships with others, appreciation and appreciation for life, personality strengths, and spiritual change) (19). In Iran, the obtained Cronbach’s alpha for this inventory was 0.92 and its reliability was 0.94 (1).
Quality of life was measured using the Quality of Life Questionnaire (EROTC QLQ-C30).This questionnaire belongs to the European Organisation for Research and Treatment of Cancer to assess the quality of life in cancer patients. It measures nine areas of symptoms (Fatigue, nausea and vomiting, pain, shortness of breath, sleep deprivation, loss of appetite, constipation, diarrhea, and financial problems) and one general area of quality of life (20-23). The validity and reliability of this questionnaire have been evaluated by Marashi T et al (22). The patients also completed Breas Cancer-Specific Quality of Life Questionnaire (QLQ-BR23). The questionnaire consists of 23 questions measuring four functional domains (sexual function, sexual pleasure, and body image and prospects) and four symptom domains (hair loss discomfort, treatment side effects, arm symptoms, and breast symptoms). The validity and reliability of this questionnaire in Iran have been assessed by Shobeiri F et al (24).
Patients were also assessed by Subjective Well-being Scale (SWS) designed by Keyes CL (8).This scale includes three dimensions of emotional well-being (12 questions), psychological well-being (18 questions) and social well-being (15 questions). Adherence was assessed using the 8-item Morisky Medication Adherence Scale (MMAS-8). The range of average scores is zero to 8. The score of less than six is classified as poor compliance, 6 to 8 is moderate and 8 is appropriate compliance. Validation of the Persian version of this tool in Iranian patients with hypertension was performed by Moharamzad Y et al (25).
Intervention
The present study utilized structured psychoeducational intervention for cancer patients developed by Fawzy FI and Fawzy NW (26) to investigate the effectiveness of group psychological training intervention on post-traumatic growth, quality of life, mental well-being, and evaluation. Table 1 presents the contents of this protocol. The intervention group received six sessions of group training for 90 minutes twice a week by a psychotherapist trained in the field of patient education. The control group received common treatments including chemotherapy, surgery and medical consultation.
Ethics approval
At the beginning and before the actual implementation of the research, the purpose of the study and the method of training for both the intervention and control groups were explained,and their consent to participate in the study was obtained. This study was approved as a minimal-risk research by the Ethics Committee of Iran University of Medical Sciences (Approval reference number: IR.IUMS.REC.1397.276).
Table 1. The content of psychological training sessions
|
Sessions |
Agenda |
|
1 |
Referrals and explanation of the structure of the meetings |
|
2 |
Health Education Health care information ,including types of cancer Different treatment methods (Lumpectomy, mastectomy, radiation therapy, chemotherapy, and tamoxifen) Good follow-up routines (Monthly self-examination of breast, annual mammography,and annual medical examinations) Group discussion |
|
3 |
Stress management Identifying sources of stress Personal reactions to stress (Physiological, psychological and behavioral reactions) Problem-solving Change of attitude Group discussion |
|
4 |
Relaxation training Explanation of relaxation exercises Progressive muscle relaxation followed by guided imaging Group discussion |
|
5 |
Coping skills Active behaviors Active cognitive methods Avoidance methods Coping scenarios (with picture) group discussion |
|
6 |
Summary Group discussion |
Results
The mean age of the intervention group was 48±9, and in the control group was 51 ± 8. The mean duration of disease in the intervention group was five months and in the control group was six months. Table 2 shows the baseline characteristics of the two study groups.
In the univariate analysis, as shown in table 3, changes in outcome variables were significantly different between the study groups in the variables of post-traumatic growth, subjective well-being and adherence to treatment.
To evaluate the mediating effect of social support and potential confounding variables (demographic variables), the crude effect of intervention variable in a regression model with only outcome variables (post-traumatic growth, subjective well-being, quality of life and treatment adherence) and the main
independent variable (intervention) was calculated. The effect size was 29.06, 24.76, 4.49 and 1.3 respectively. The p-value was less than 0.001 in post-traumatic growth and subjective well-being, 0.01 for adherence and was not statistically significant for the quality of life (p-value=0.24)
Then, the effect size mentioned above for the post-traumatic growth, subjective well-being, and treatment adherence variables was recalculated in the presence of social support variables and potential confounding variables in separate models (adjusted model). The size of the primary crude effect was compared with the effect size calculated in the secondary model. Table 4 shows the result of multivariate analysis. Due to the difference between the crude effect size and the adjusted as less than 10%, there is not a mediator and potential confounder variable.
Table 2. Baseline characteristics of intervention and control group
|
Variable |
|
Intervention |
Control |
||
|
Frequency |
Percentage |
Frequency |
Percentage |
||
|
Education |
Primary school |
9 |
30 |
5 |
16.7 |
|
Secondary school |
18 |
26.7 |
12 |
40 |
|
|
Undergraduate |
2 |
6.7 |
3 |
10 |
|
|
Graduate |
1 |
3.3 |
0 |
0 |
|
|
Employment |
Employed |
4 |
13.3 |
7 |
23.3 |
|
Non-employed |
26 |
86.7 |
23 |
76.7 |
|
|
Marriage status |
Married |
25 |
83.3 |
28 |
93.3 |
|
Single |
5 |
16.7 |
2 |
6.7 |
|
|
Kind of therapy |
Mastectomy |
14 |
46.7 |
11 |
36.7 |
|
Lumpectomy |
16 |
53.3 |
19 |
63.3 |
|
|
Stage of cancer |
1 |
12 |
40 |
15 |
50 |
|
2 |
18 |
60 |
15 |
50 |
|
Table 3. Comparison of changes in outcome variables between two study groups in univariate analysis
|
Outcome variables |
Group |
N |
Average change after - before |
SD |
p-value |
|
Post-traumatic growth change |
Intervention Control |
30 30 |
21.56 - 7.20 |
14.00 14.44 |
0.001> |
|
Subjective well-being change |
Intervention Control |
30 30 |
32.46 7.70 |
16.84 31.36 |
0.001> |
|
Quality of life change |
Intervention Control |
30 30 |
- 13.96 - 9.46 |
9.953 16.78 |
0.24 |
|
Adherence change |
Intervention Control |
30 30 |
1.16 - 0.13 |
2.03 1.94 |
0.01 |
Table 4. Assessing the mediator effect of social support and potential confounding factor of age, education, and occupation (Multivariate analysis)
|
Adherence |
Well-being |
Post-traumatic growth |
|
|
1.30 |
24.76 |
29.06 |
Crud effect size |
|
1.30 |
24.78 |
29.11 |
Social support |
|
1.18 |
23.22 |
29.60 |
Age |
|
29.09 |
24.69 |
1.29 |
Education |
|
28.32 |
23.12 |
1.38 |
Occupation |
Discussion
Based on the result, psychological training has been effective in improving post-traumatic growth. The results are in line with the findings of previous literature (27-30). Garlan et al (31) showed that participants in the intervention group reported more traumatic growth than the control group.
In explaining the effectiveness of psychological training on post-traumatic growth in breast cancer patients, as Lelorain and Bonnaud-Antignac (32) have pointed out, talking to others can stimulate reassessment, facilitate the reconsideration of world assumptions, create meaning, and reinforce emotion expression. Talking and thinking about loss has been associated with finding meaning and post-traumatic growth in other stress-stricken populations. According to the ontological and cognitive processing models, the perceived threat from breast cancer is positively related to traumatic growth (2).
What is important in post-traumatic growth in cancer patients is that they see the stress associated with the disease as a challenge for personal growth, understanding the meaning of life, reviewing their lives,and their connection to the world (32). Lelorain et al showed that positive, active, relational, religious, and partially consistent coping has a significant effect on post-traumatic growth. Coping strategies play an important role in traumatic growth. In many cancer situations, adaptive coping such as religious coping, acceptance, or reinterpretation, has been positively associated with post-traumatic growth, whereas maladaptive coping such as substance use or self-blame is not associated with growth (32).
The perception of the stressful event threatens one’s core belief system. The core beliefs are “A general set of one’s beliefs about the world, how one functions and one’s place in it.” Following a stressful event, one’s core beliefs may be challenged, and the person’s hypothetical world may become unstable, uncontrollable, and unpredictable. To manage distress (as well as challenge towards core beliefs) and reevaluate pre-traumatic cognitive schemas, survivors use various cognitive mechanisms such as coping strategies, social support seeking, cognitive participation (Uninvolved thinking, and meditation). They begin by trying to give meaning to a stressful experience. Group psychosocial interventions may enhance post-traumatic growth by enhancing emotional expression, cognitive processing, and positive evaluation of a stressful event (32).
Although previous research suggested that psychoeducation had a positive effect on patients’ quality of life (33,34), no such results were found in this study. This may be due to participation of individuals in the post-test which was performed after the surgery, with patients suffering from a variety of physical problems such as pain, and post-operative complications such as fatigue, nausea, and vomiting. Another reason may be related to short-term education because studies that showed an improvement inquality of life after intervention provided long-term education for patients. Long-term interventions are needed to evaluate the effectiveness of other types of psychosocial support in improving the quality of life in early-stage breast cancer patients.
Regarding the third hypothesis of the research suggesting that group training in psychological training is effective on increasing subjective well-being in patients with breast cancer, the findings of the study showed that group psychological training had a significant effect on promoting the mental well-being of women with breast cancer. This is in line with the results of the studies by Al-Sulaiman et al (7) and Dow Meneses K et al (34).
In explaining the effectiveness of psychological education on improving the well-being of patients with breast cancer (35,36), one’s psychological resources influence one’s ability to use social support to improve subjective well-being. In the context of the group, supportiveness can come from group members. Group support for cancer patients is a source of emotional support. And there is evidence that for isolated individuals, the group can play such a role.
Psychosocial interventions can improve patients’ knowledge and awareness of emotional and physical responses to stress and increase their confidence, help manage pain and other physical and emotional symptoms; they can help to reduce uncertainty, stress, anxiety, helplessness and fear of unknown conditions and psychological discomfort through relaxation training and other techniqueswhich consequently improve psychological and physiological adaptation indexes. Health-promoting behaviors such as exercise, diet, sleep, and medication psychosocial skills and the use of interpersonal skills to build and maintain social support, coping strategies in helping to identify and change negative beliefs, beliefs and expectations, increasing ability to control thoughts, beliefs, and attitudes, as well as more positive attitudes to clinical trials all enhance the psychological well-being of patients with cancer.
Concerning the fourth hypothesis of research suggesting that group training in psychological training is effective in increasing adherence to treatment for patients with breast cancer, the findings of the study showed that group psychological training has significant effect on promoting adherence to treatment of women with breast cancer and this is consistent with the results of studies by Jeffries SA et al, (37) and Myers RE et al (38).
In explaining the effectiveness of psychological training on promoting adherence to treatment for patients with breast cancer, it can be said that according to Myers RE et al (38), forgetfulness, anxiety, lack of knowledge and skills, and misconceptions about therapeutic measures can be improved. Interventions in adherence to treatment include patient education strategies, including education about chronic diseases such as cancer, the benefits of treatment, and the serious consequences of non-compliance. And behavioral adjustment strategies include awareness of the benefits of follow-up and the high costs incurred by non-compliance (39). Training these topics can increase adherence to treatment for cancer patients.
Also, the results of this study are inconsistent with the findings of Al- Sulaiman et al (7). In this study, crisis counseling and psychological education did not have a significant effect on adherence to treatment for patients with breast cancer. This may be due to differences in mean age of the groups, instruments used, and duration of intervention.
The fifth hypothesis of the research aboutthe role of group intervention in psychological education and development of post-traumatic social support was not confirmed in this study. Although studies have shown the mediating role of social support, according to the studies of Shorey S et al (14) and Brand EF et al (15), psychological education can increase social support. And social support can also increase post-traumatic growth, according to studies by Cobb (10), Scrignaro M et al (16), Schroevers MJ et al (17), and Bozo O et al (18). Intermediary role failed because there are other variables between psychological education and social support or between social support and traumatic growth. The patients’ conditions in the ward and during the surgery and the short duration of the intervention may also play a role, which requires further research.
The evidence from this study is also consistent with the sixth hypothesis, in line with the researches of Garlan RW et al (31), Rolnick SJ et al (39), and Baglama B et al (40), suggesting that age, education, occupation and marital status of individuals do not have much effect on the benefits of psychological training. While in marriages belonging to an ethnic minority group, higher education, employment, and youth are positively correlated with post-traumatic growth, the results suggest that these socio-demographic variables account for diversity (41). Few have been studied in our sample. In other words, the response to cancer is not determined so much by the concrete properties of the situation and the individual, but by the subjective reactions to the experience (e.g. disability, controllability, a threat to life, etc.) and the perceived interpersonal context (42).
Research limitations
There are some limitations to this study. Short-term intervention due to limited hospitalization of patients inward is the first limitation. Moreover, due to the nature of the intervention blindness is impossible for participants and the researcher. But the person who analyzed the data did not know the cases.
Conclusion
Psychological interventions, such as psychoeducation, have positive effects on traumatic growth, subjective well-being ,and adherence to treatment. However, no positive results were found in this study regarding the impact of psychological education on quality of life.