Document Type : Original article
Introduction
In December 2019, a novel human coronavirus (COVID-19) was reported in Wuhan, China, caused by severe acute respiratory syndrome coronavirus 2 (SARS CoV-2) (1,2). Its incubation period is about 14 days, and it causes a wide range of symptoms from a mild cold to severe life threatening pneumonia (3). In just a few months, it spread to other countries and emerged as a global public health crisis. In March 11th 2020, World Health Organization (WHO) announced it a pandemic (4). Despite all efforts, the virus is still spreading. To date (December 15th, 2020), more than 70 476 836 cases are infected, resulting in 1 599 922 deaths (5). Due to COVID-19 pandemic, surgical practices have changed worldwide and our country is not an exception. Many guidelines have suggested to postpone elective surgeries to the end of pandemic (6-9). For less virus exposure, hospitals have reduced the number of non-emergent surgical practices. Conducting safe surgery during this pandemic is an important concern. There is a risk of transmitting the virus during open and laparoscopic surgeries. Based on postoperative outcomes of many diseases, minimally invasive surgery is preferred to open surgery (10). The typical advantages can be faster recovery time after surgery, short hospital stays and less complications after surgeries (11).
In this study, postoperative complications and pneumonia development were evaluated in patients undergoing laparoscopic surgery in this pandemic era.
Materials and Methods
Study design and participants
This is a prospective cohort study with four weeks follow up in the laparoscopic surgeries department of teaching hospitals of Tehran University of Medical Sciences including Sina Hospital, Imam Khomeini Hospital, Shariati Hospital, Laleh Hospital, and Amiralam Hospital.
This study was reviewed and approved by ethics committee of Tehran University of Medical Sciences (IR.TUMS.VCR.REC.1399.396). Oral consent was obtained from all patients.
All patients undergoing laparoscopic surgeries from February 20th to May 13th, 2020 were included in this study.
Demographic and clinical data including sex, age, history of cancer, diabetes, high blood pressure, cardiovascular diseases, pulmonary diseases, smoking or substance abuse, as well as related symptoms and predisposing factors of COVID-19 such as fever, cough, myalgia, dyspnea, contact history with a person diagnosed with COVID-19 or traveling history were obtained with a researcher made data collection form by trained physicians at admission time. No exclusion criteria were considered for this study. Preoperative chest x-rays (CXRs) were performed routinely for all patients. Due to COVID-19 pandemic situation, Reverse Transcription Polymerase Chain Reaction (RT-PCR) on nasopharyngeal sample was performed for all patients before the surgery. When diagnostic kits were not available, clear CXR and absence of symptoms such as fever, cough, myalgia, and dyspnea were the evidence of not being infected with COVID-19.
All patients underwent laparoscopic surgeries for their specific problems. Types of the laparoscopy and its duration, days of hospital or ICU stay were all recorded.
After hospital discharge, all patients were followed up by phone calls by the same trained physicians weekly during four weeks to assess the appearance of symptoms including fever, cough, myalgia, and dyspnea. If the patients didn’t respond, the physicians were required to contact them for three times. At the end of the 4 week follow up, patients were asked to have RT-PCR test to confirm whether they are negative for COVID-19 or not.
Statistical analysis
Descriptive data are expressed as mean and standard deviation and for qualitative variables, frequency and percentage were used. All statistical analyses were performed with IBM SPSS Statistics 18 (IBM Inc., New York, USA).
Results
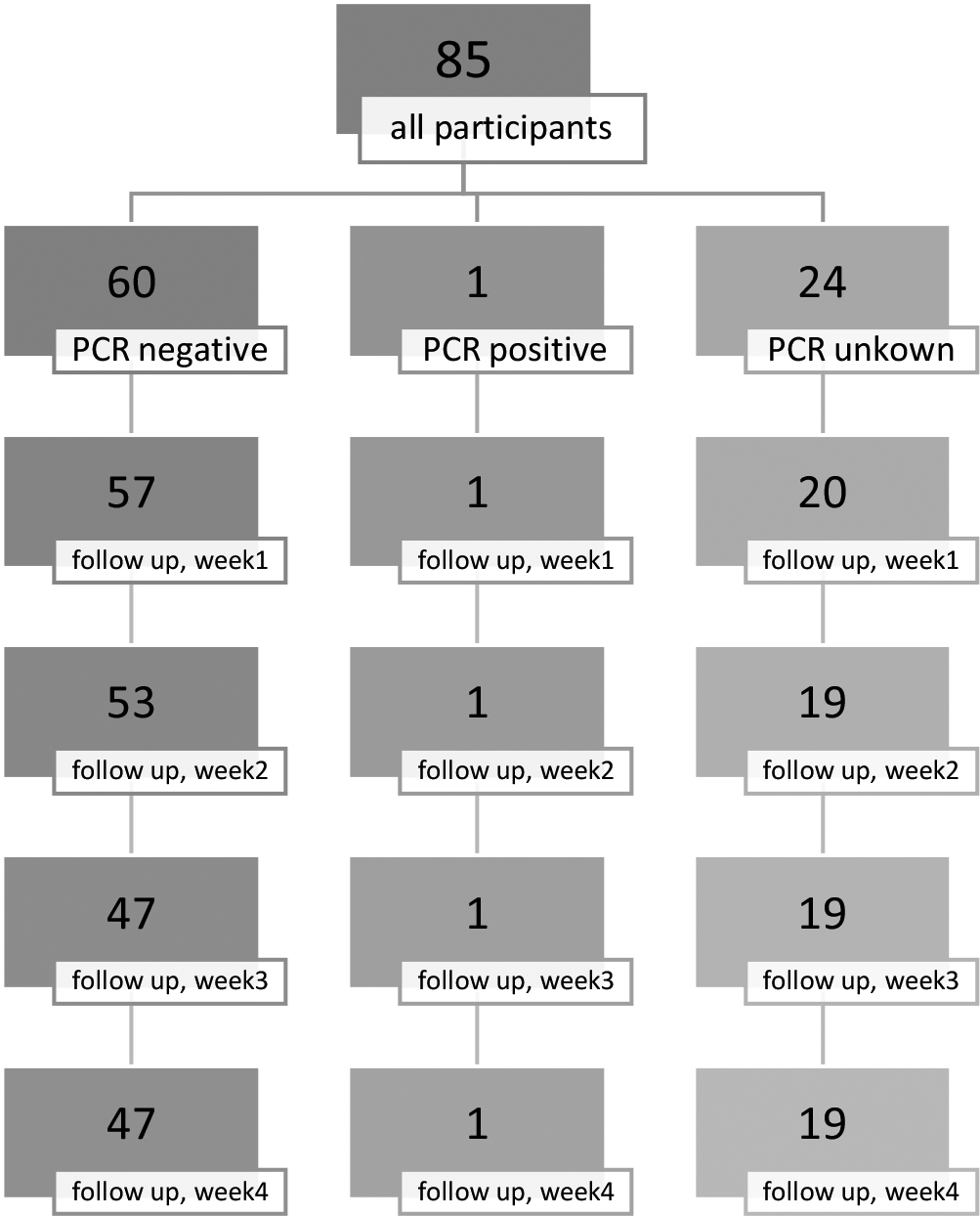
COVID-19 diagnostic kits were not available in some medical centers at the beginning of the COVID-19 pandemic. Of all 85 patients who were candidates for laparoscopic surgeries, RT-PCR was done in 61 patients among whom just one positive test result was recorded. CXR was done for all patients and all had normal CXRs. No patients had the symptoms of fever, cough, myalgia, dyspnea before the surgeries. Overall, 85 patients underwent laparoscopic surgeries.
The mean age was 43.7±15.6 (17 to 84 years). Fifty-seven patients (67%) were women. Comorbidities are shown in table 1. Thirteen patients (15.3%) had one or more comorbidities. Hypertension (8.2%) was the most common comorbidity. Of all patients, 4.7% were smokers and only one patient used opium. Study participants underwent various laparoscopic procedures as shown in the table 1. The mean laparoscopic duration was 94.6±70.8 min. No complication was detected after the surgery. Mean hospital stay was 3.5±4.6 days. No COVID-19 related symptoms such as fever, cough, myalgia, and dyspnea were observed during hospitalization (Table 1).
Among all patients, only one patient was positive for COVID-19 on admission. He was a 55 year old man with no history of previous disease or smoking. He underwent laparoscopic surgery due to gangrenous cholecystitis. The surgery duration was 90 minutes, and no complication or mortality was reported after the surgery. He stayed in hospital for three days.
After discharging, all 85 patients were followed up weekly during four weeks. The number of patients responded is shown in figure 1. No COVID-19 related symptoms were reported within the follow up time. After four weeks of follow up, 27 patients (31.2%) agreed with performing the RT-PCR test for COVID-19; all were negative for COVID-19. Also, for the patient with positive test result for COVID-19 on admission, RT-PCR of nasopharyngeal sample at the end of the follow up showed negative result for COVID-19.
Table1. Demographic and clinical data of patients undergoing laparoscopic surgeries
|
|
Frequency |
Percentage |
|
Woman |
57 |
67 |
|
Man |
28 |
33 |
|
Past medical history |
|
|
|
Hypertension |
7 |
8.2 |
|
Coronary diseases |
2 |
2.4 |
|
Diabetes |
3 |
3.5 |
|
Cancer |
2 |
2.4 |
|
Pulmonary diseases |
2 |
2.4 |
|
Smoking |
4 |
4.7 |
|
Comorbidity≥1 |
13 |
15.3 |
|
Surgery type |
|
|
|
Bariatric surgery |
9 |
10.6 |
|
Cholecystectomy |
39 |
45.9 |
|
Hernia |
11 |
12.9 |
|
Gastrojejunostomy |
2 |
2.4 |
|
Diagnostic |
5 |
5.9 |
|
Ovarian dermoid cyst resection |
1 |
1.2 |
|
Endometriosis cyst resection |
1 |
1.2 |
|
Choledochoduodenostomy |
1 |
1.2 |
|
Fundoplication |
2 |
2.4 |
|
Hydatid cyst resection |
1 |
1.2 |
|
Parathyroidectomy |
1 |
1.2 |
|
Sleeve |
9 |
10.6 |
|
Appendectomy |
3 |
3.5 |
Discussion
The COVID-19 related symptoms will appear if a person is infected. The incubation period of the disease is about 14 days (3). Therefore, the patients were followed during 4 weeks for further evaluation. Based on the result of our study, the patients undergoing laparoscopic surgery did not show any COVID-19 related symptoms including fever, cough, myalgia, and dyspnea after surgery, neither during hospitalization nor during follow up time.
Not much is known about COVID-19 and the outcomes of patients undergoing operation (whether symptomatic or asymptomatic) during this era. As long as there is no definite treatment for the infectious disease, protecting the patients is of paramount importance.
Decisions about each patient must be made before the surgery. Therefore, it is substantial to screen patients in advance. In case of positive test result for COVID-19 and emergent surgery, the availability of Personal Protective Equipment (PPE) should be enhanced to decrease the transmission risk of infection and only the professional staff who are required for the procedure should be in the operating room (6).
Before the COVID-19 pandemic, the main treatment of many diseases such as cholecystitis or appendicitis was surgery, whether open surgery or laparoscopy. But during the epidemic era, some guidelines suggested to treat uncomplicated cases with antibiotics. Many surgeons argued against it because such a conservative treatment results in longer recovery time and hospital stay. Patients may acquire infections during hospital stay. Longer hospital stay may result in getting COVID-19 in hospital (12,13). Since the tissues are less traumatized in laparoscopy, the patients will be recovered faster resulting in shorter hospital stay. Due to shorter hospital stay, the patients’ exposure to infectious diseases will be decreased (14).
Some studies indicated that surgical smoke might contain coronavirus. Surgical smoke is generated in both open surgery and laparoscopy. The point is that the closed cavity in laparoscopy makes it possible to control the smoke during the practice. Even if it is transmitted through the smoke, there is currently no data to confirm its risk of contagion (15).
Conclusion
There was no increased risk of postoperative complications and COVID-19 infection for patients undergoing various types of laparoscopic surgery in this study and laparoscopy was safe for the patients.
Acknowledgements
We are indebted to staff of Research Development Center of Sina Hospital for their technical help.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of Interest
The authors declare that there are no conflicts of interest.
Ethics approval
This study was reviewed and approved by ethics committee of Tehran University of Medical sciences (IR.TUMS.VCR.REC.1399.396).