Document Type : Original article
Abstract
Background: Chronic Obstructive Pulmonary Disease (COPD) is an airway obstructive disease that is often caused by smoking. The disease is currently the third leading cause of death worldwide. The current therapeutic approach is based on Non-Invasive Ventilation (NIV) therapy, which can reduce mortality, the need for hospitalization in the intensive care unit, and to some extent therapeutic complications. Therefore, this study was performed to determine the effect of non-invasive ventilation along with routine treatments on respiratory markers, inflammation, and clinical status of patients with COPD.
Methods: A total of 30 patients with COPD referred to Masih Daneshvari Hospital were divided into control and intervention groups. In the intervention group, 15 patients underwent non-invasive ventilation in addition to the usual treatments, and in the control group, the patients underwent only the usual treatments. After completing the mMRC (Modified Medical Research Council) questionnaire and evaluating FEV1 (Forced Expiratory Value in one score), 5 ml of blood samples were taken from these patients at the beginning of the study, on the seventh to tenth day, and also in the third month, and the results of this evaluation were compared between the two groups.
Results: Based on the results of this study, the mMRC score of the intervention group was significantly lower than the control group in the first week (p=0.043) and three months after treatment (p=0.049). However, indices such as FEV1, and IL-8(Interleukin-8) did not change significantly in both groups.
Conclusion: The use of non-invasive mechanical ventilation along with standard treatments can play a relative role in improving patient outcomes.
Keywords: Chronic obstructive pulmonary disease, Interleukin-8, Non-invasive mechanical ventilation
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is an inflammatory disease of the airways that is more common in smokers. Genetics, air pollution, and respiratory infections that occur in childhood can also affect the risk of developing this disease (1). Inflammatory changes of COPD have transformed this disease from a limited disease to systemic inflammatory disease and in its pathogenesis, inflammatory changes and processes, cell proliferation, apoptosis, alteration of lung cell characteristics, and extracellular matrix regeneration have been identified (2,3). Exacerbation of COPD is associated with the presence of a combination of epithelial cells, acute and chronic inflammatory cells, as well as large numbers of neutrophils in the airway mucus. Also, in the inner layer of the airways, the thickness of the muscular layer is increased and mild and complex inflammatory infiltration is observed (4).In such cases, CD8+ T-cell, eosinophils, and neutrophils are found in the bronchial biopsy of these patients. Besides, signs of inflammation are visible in the areas around the bronchi, especially in people with chronic bronchitis (5,6). Also, airways smaller than 2 mm contain mucus and can lead to airway obstruction and FEV1 changes (7). Following smoking and exposure to other respiratory stimulants, inflammatory cells migrate to the lungs and airways. As a result, lung damage and impaired normal lung repair will be predictable (8). Neutrophils, eosinophils, macrophages, and lymphocytes are inflammatory cells produced in response to COPD (9,10). In patients with COPD, interleukin-8 levels also increase due to an increase in neutrophils (11,12). Interleukin-8 is produced by stimulation of smoking, TNFα, and LPS. This chemokine is a potent chemoattractant for neutrophils. Advanced COPD often occurs due to infection, and patients need routine treatments including the use of bronchodilators and inhaled and injectable steroidal anti-inflammatory drugs at various doses, besides other treatments to prevent hypoxemia and hypercarbia (13).
Non-Invasive Ventilation (NIV) can significantly reduce mortality, the need for intubation, treatment complications, and hospital stays. There are several types of this method, including bi-level Positive Airway Pressure (BiPAP) and Continuous Positive Air Pressure (CPAP) (14).
In the present study, the effect of NIV treatment and specifically BiPAP was investigated in patients with COPD referred to Masih Daneshvari Hospital in Tehran before receiving treatment, 7 and 10 days later, and also 3 months after receiving treatment. This study aimed to evaluate the therapeutic effect of NIV on inflammatory factors and clinical parameters in these patients.
Materials and Methods
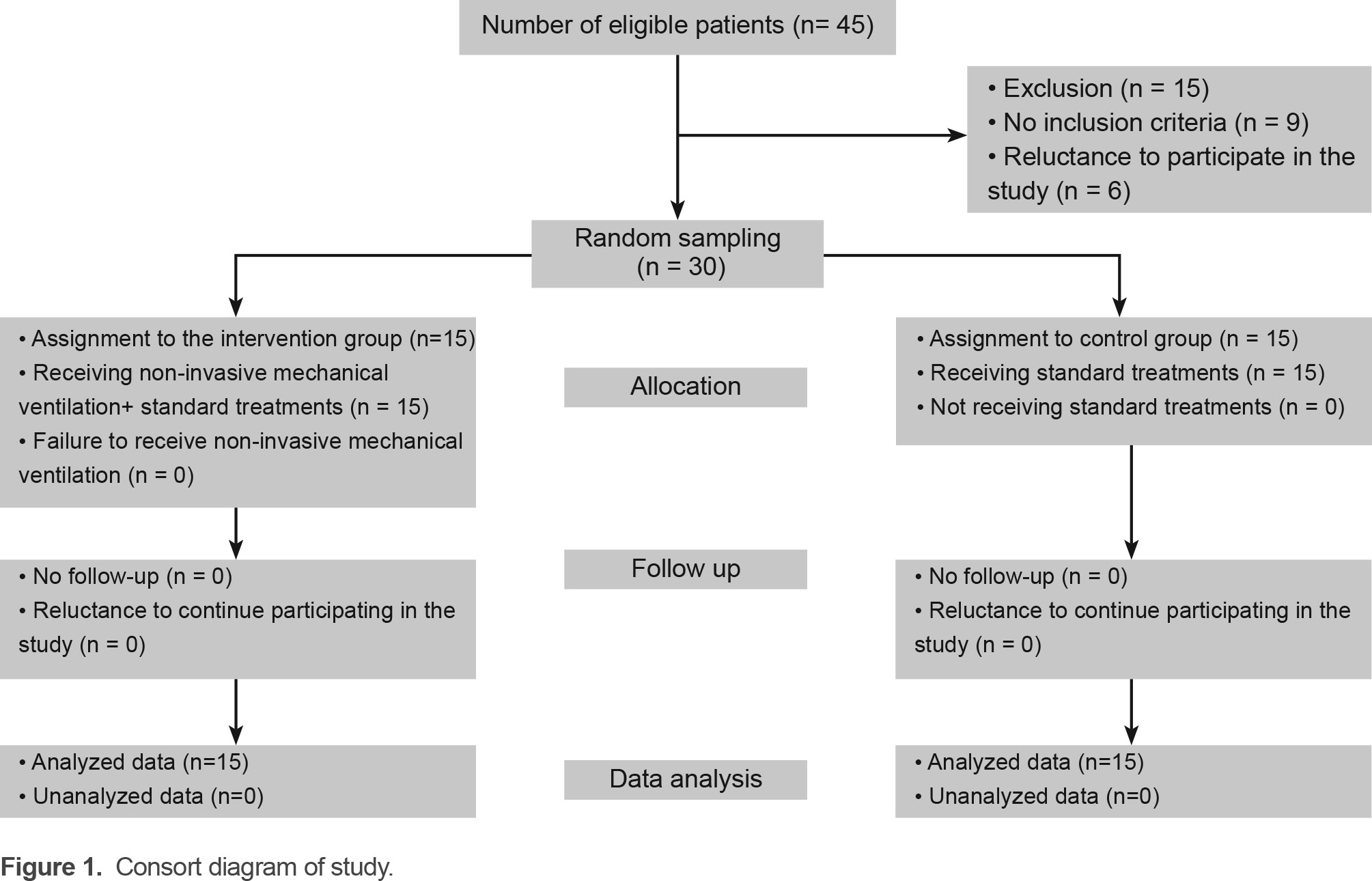
The present study was performed at Masih Daneshvari Hospital in Tehran with the ethical code of sbmu1.REC.1392.21. After obtaining written consent from patients, 30 patients with inclusion criteria (Diagnosis of COPD by a physician, knowledge of study conditions) were divided into two groups using a simple randomization based on codes assigned to each patient (Figure 1).
In the intervention group, patients underwent non-invasive ventilation in addition to common treatments, and in the control group, patients were evaluated by common treatments.
Exclusion criteria included the presence of other conditions associated with COPD, such as pleural effusion, tumor, evidence of pulmonary pneumonia, and pulmonary aspiration. After receiving 5 ml of blood samples, hospitalized patients were treated with BiPAP and routine COPD treatments. During hospitalization, respiratory tests, Body Mass Index (BMI), and PCO2 (Partial pressure of carbon dioxide) were evaluated and the gold stage was determined. Also, a clinical examination was performed and the patient’s mMRC was recorded.
Patients in the intervention group (15 patients) received non-invasive ventilation during their hospitalization. After 10 days of hospitalization, with collection of 5 mls of the blood sample, patients were discharged with instructions for use of O2 and BiPAP. Discharged patients underwent blood sampling again during the quarterly follow-up and were evaluated for IL-8 levels as well as the effectiveness of other treatments (BiPAP, inhaled corticosteroids, Atrovent, B2-agonist). In the control group, patients received only the common treatments.
The present study was analyzed using SPSS 16 (SPSS Inc, USA), taking into account the 95% confidence interval while the significance was
Results
In the present study, a total of 30 patients (15 patients in each group) with COPD referred to Masih Daneshvari Hospital were evaluated, in which 12 patients were male (p=0.990) (Consort flowchart). The mean age of patients in the control group was 67.8±7.7 and in the intervention group was 65.1±9.8 (p=0.400). Findings from the demographic information of patients in the two groups treated with NIV and the control group are shown in figure 2.
The mean of FEV1 in the first week of treatment was 42.9±10.7 in the control group and 40.8±10.1 in the intervention group and there was no significant difference (p=0.880). Also, the results obtained in the first week showed that the mean mMRC in the intervention group was significantly lower than the control group (2.7±0.82 vs. 3.3±0.7) (p=0.043).
On the other hand, the level of serum interleukin-8 in the control group was 1409.3±306.7 mg/dl and in the intervention group was 1425.4±473.8 mg/dl.
The mean difference of this variable in the two groups under study was not statistically significant (p=0.650). The values of these variables are shown in table 1.
Secondary outcome variables
Three months after the intervention, vital signs and FEV1 levels, mMRC scores, and serum IL-8 levels in both groups were assessed. Based on the findings of these evaluations, the mean systolic blood pressure in the control group was 135.3±13.6 and in the intervention group was 124.3±8.8 mmHg (p=0.020). Also, the mean diastolic blood pressure in the mentioned groups was 77.7±5.0 and 78.0±7.3 mmHg, respectively (p= 0.790). The study of patients’ heart rate showed that the mean of the control group was 73.5±7.9 beats per minute and in the group treated with NIV was 73.3±6.1 beats per minute.
Based on the data obtained from this study, the mean heart rate of patients in the intervention and control groups was not statistically significant (p=0.840). Also, the mean of breaths per minute in the control group was 15.2±1.3 and in the intervention group was 15.0±1.5 (p=0.650). Similar findings were observed in the evaluation of central temperature (p=0.410). The mean level of FEV1 in the control group in the third month of treatment was 46.7±12.6 and in the intervention group was 48.7±14.0 (p=0.720).
The mean of mMRC in this evaluation period in the intervention group was significantly lower than the control group (2.1±0.82 vs. 2.7. 0.6) (p=0.049). Besides, the mean serum level of IL-8 in the third month in the control group was 149.8±294.7 mg/dl and in the intervention group was 124.7±420.1 mg/dl (p=0.060) (Table 1).
Table 1. Comparative study of FEV1, mMRC, and IL-8 before the study, in the first week and after three months from the beginning of the study
|
|
Intervention group Mean ±SD |
Control group Mean ±SD |
p-value |
|
|
Before the study |
FEV1 |
36.9±9.1 |
37.3±9.4 |
0.921 |
|
mMRC |
4.23±1.1 |
4.01±0.9 |
0.720 |
|
|
IL-8 |
1697±304.22 |
1630±279.25 |
0.570 |
|
|
First week |
FEV1 |
40.8±10.1 |
42.9±10.7 |
0.880 |
|
mMRC |
2.7±0.82 |
3.3±0.7 |
0.043 |
|
|
IL-8 |
1425±473.8 |
1409.3±306.7 |
0.650 |
|
|
After three months |
FEV1 |
48.7±14.0 |
46.7±126 |
0.720 |
|
mMRC |
2.1±0.82 |
2.7±0.6 |
0.049 |
|
|
IL-8 |
124.7±420.1 |
149.8±294.7 |
0.060 |
|
Discussion
The results of the present study showed that the use of non-invasive mechanical ventilation has a relative effectiveness in improving the condition of COPD patients compared to standard treatment without non-invasive mechanical ventilation. One-week and three-month follow-up in this study showed that the use of this treatment can significantly reduce the mMRC score and lead to improved respiratory conditions in these patients. However, the use of non-invasive ventilation has no significant effect on FEV1 levels, and interleukin-8 levels as an inflammatory factor.
Numerous studies and meta-analyses have shown that the use of NIV improves short-term outcome in patients (15). The evaluation performed in the present study also reveals the role of this treatment in improving the long-term outcome of COPD patients. However, many patients are unable to tolerate this treatment. Despite the results of this study, Struik et al in 2014 with a one-year follow-up showed that the use of NIV along with standard treatment has no role in improving the outcome of COPD such as mortality, hospitalization, dyspnea and long-term hypercapnia (16). Plant et al also stated that the use of NIV improves acidosis during the first 4 hours, but has no effect on the long-term outcome of patients (17). However, the results of some researches are consistent with the present study, as Confalonieri et al have shown that the use of NIV improves the short-term and long-term outcomes of patients with COPD (18). The reason for the difference in the results was due to the way the groups were selected in these studies.
Systemic inflammation is closely related to the development and spread of comorbidity in COPD patients. Oxidative stress and inflammation of the respiratory tract are seen in patients with COPD. Migration of immune and inflammatory cells into the peripheral airways during COPD and increased levels of interleukin-8 in bronchoalveolar lavage fluid have been demonstrated (19). Inflammation is characterized as a dominant aspect in COPD by the presence of activated neutrophils and macrophages. This increases the level of inflammatory mediators such as interleukin-8 (20). Accordingly, the improvement of inflammation can be considered as a favorable prognostic factor. That is the reason for using serum interleukin-8 levels by researchers as the main evidence.
The present study showed that the serum level of this biomarker in the three months of follow-up did not differ significantly between the two groups treated with NIV and the control group. In this regard, Márquez-Martin et al showed in their research that the combination of exercise and the use of NIV can play a significant role in reducing the level of inflammatory factors such as interleukin-8. However, the use of NIV alone has little effect on the level of these biomarkers (21). Because exercise produces inflammatory factors, it can be concluded that NIV may increase elevated and high levels of inflammatory factors and may not have an effect on the average increase in these factors that occurs during COPD. Further studies in this field are required to support this finding. However, Paone et al in their study which aimed to investigate the role of long-term home use of NIV on the systemic inflammatory response in patients with COPD reported conflicting findings. The researchers have shown that long-term use of NIV increases interleukin-6 levels and tumor necrosis factor alpha (TNF-ɑ) while decreasing interleukin-10 levels (22). The researchers did not study interleukin-8 levels. Interleukin-8 is evidence of innate immunity, and interleukin-6 and interleukin-10 are secreted more than B and T cells (Specific immunity). Therefore, comparing the present study with the findings of Paone et al’s study is somewhat difficult. In general, the role of NIV therapy in patients’ inflammatory response needs further investigation.
Conclusion
The findings of the present study showed that the use of non-invasive mechanical ventilation along with standard treatments can play a relative role in improving patient outcomes. Also, a one-week and three-month follow-up in this study showed that the use of this treatment had no effect on FEV1 levels and interleukin-8 levels as an inflammatory agent but could lead to an improvement in the mMRC score.
Conflict of Interest
There is no conflict of interest in this study.