Document Type : Review article
The COVID-19 virus has caused many deaths of people worldwide since the pandemic began. However, no definitive treatment for this infection has been discovered so far. It has been shown that comorbidities such as diabetes, hypertension and cardiovascular diseases are associated with an increased risk of SARS-COV-2 infection. Interestingly, SARS-COV-2, like SARS-COV, uses the ACE2 gene to enter the host cell. Also, changes or imbalance in ACE2.ACE can affect SARS-COV-2 susceptibility, related outcomes and mortality. Regarding the crucial role of ACE2 protein in COVID-19 infection, the effect of different factors such as age, BMI, physical activity levels, nutritional status, altitude, as well as blood group was assessed on the level of this protein. Further, to our knowledge, no study has been conducted to examine factors that increase or decrease the risk of COVID-19 and its related severity and outcome in normal subjects emphasizing the pivotal role of ACE2. Therefore, the primary purpose of this study was to investigate the involved mechanisms of ACE2 protein and other risk factors causing infection in different situations and finally, to introduce a safe, accurate, and cost-effective approach to prevent SARS-COV-2 infection and hard clinical outcomes in normal subjects.
Keywords: Blood group antigens, Body mass index, COVID-19, Nutritional status, SARS-CoV-2
Introduction
The 2019 novel coronavirus (2019-nCoV) was recently named SARS-CoV-2 by the World Health Organization (WHO). The disease caused by SARS-CoV-2 has been named COVID-19 (1). Recent studies have shown that the Renin-Angiotensin System (RAS) plays major physiological roles in the respiratory system and two axes of ACE2/ANG1-7/MAS Receptor and ACE/ANG2/AT1 are the main parts of this system and the balance between the function of these two axes is very crucial (2), because ACE2 is expressed in various human tissues including the lungs, serving as the doorway by which the virus can enter and spread (3). However, it should be noted that there are two kinds of ACE2, the full-length and the soluble. The soluble type of ACE2 does not have the membrane anchor and circulates in small amounts in the blood (4). The full-length type, expressed in various tissues like the lungs, affects the connection between SARS-COV-2 and the RAS system, because it includes a structural transmembrane domain that operates as the receptor for the SARS-COV-2 spike protein which simplifies the entry of the virus into host cells, viral replication and cell-to-cell transmission (4,5). The interaction with the SARS-CoV-2 would result in a diminished ACE 2 enzymatic activity, an imbalance favoring the ANG II and AT1R axis and virus-induced lung injury (6). Among cases infected with SARS-CoV-2, various conditions have been associated with increased virus susceptibility and the burden of COVID-19.
Recently, it has been reported that there is a robust association between obesity, age, sex, physical fitness status, vitamin D levels, living at high altitude and specific blood group with the risks, clinical consequences [Hospitalization or needing treatment in Intensive Care Units (ICUs)] and mortality of COVID-19 infection (7-16). Interestingly, the expression of the ACE2 protein (SARS-COV-2 receptor) is very different in the mentioned groups. For example, the level of ACE2 in the normal elderly is lower than younger people (17,18) or physical training and hypoxia may increase ACE2 levels in people (19,20). Moreover, some differences in this protein are related to biological inheritance. It has well established that ACE2 levels are higher in men than in women (17,21). Besides, type A blood was a risk factor for getting COVID-19 while O blood type had a protective effect (22,23).
Regarding the recent evidence about COVID-19 susceptibility and outcomes in mentioned subjects, the crucial role of ACE2 protein in SARS-COV-2 infection and the variety of ACE2 expression levels in these people, it can be assumed that changes or imbalance in ACE2/ACE levels can affect COVID-19 susceptibility and outcomes in these subjects. Therefore, the primary purpose of this study was to investigate the relationship between ACE2 protein and other risk factors of the disease in different conditions and finally introduce a safe, accurate and cost effective approach to prevent SARS-COV-2 infection and hard clinical outcomes in normal subjects.
Materials and Methods
Data collection
Three electronic data bases of google scholar, Pub Med/MEDLINE and EMBASE were comprehensively evaluated (From its earliest inception to November 20,2020) using keywords including combination of “SARS-COVID-2”, “COVID-19 and ACE2”, “RAAS system and COVID-19”, “SARS-COVID-2 risk factors”, “High risk COVID-19 patients and “COVID-19 susceptibility”. All articles published in English were evaluated and references of selected papers were scrutinized to find other relevant papers.
Inclusion and exclusion criteria
In this narrative review, studies reporting the following items were included: (1) epidemiological research about COVID-19 in normal subjects, (2) ACE2 alterations in COVID-19 patients, (3) high and low risk subjects with COVID-19 and (4) severity and mortality rate of COVID-19 in mentioned groups. Our exclusion criteria were: (1) case reports, (2) articles published in languages except English, (4) pieces of correspondence, (5) local studies and (6) retracted papers. Further, an attempt was made to minimize the possibility of including patients from the same population twice when exploring one outcome.
Screening and data extraction
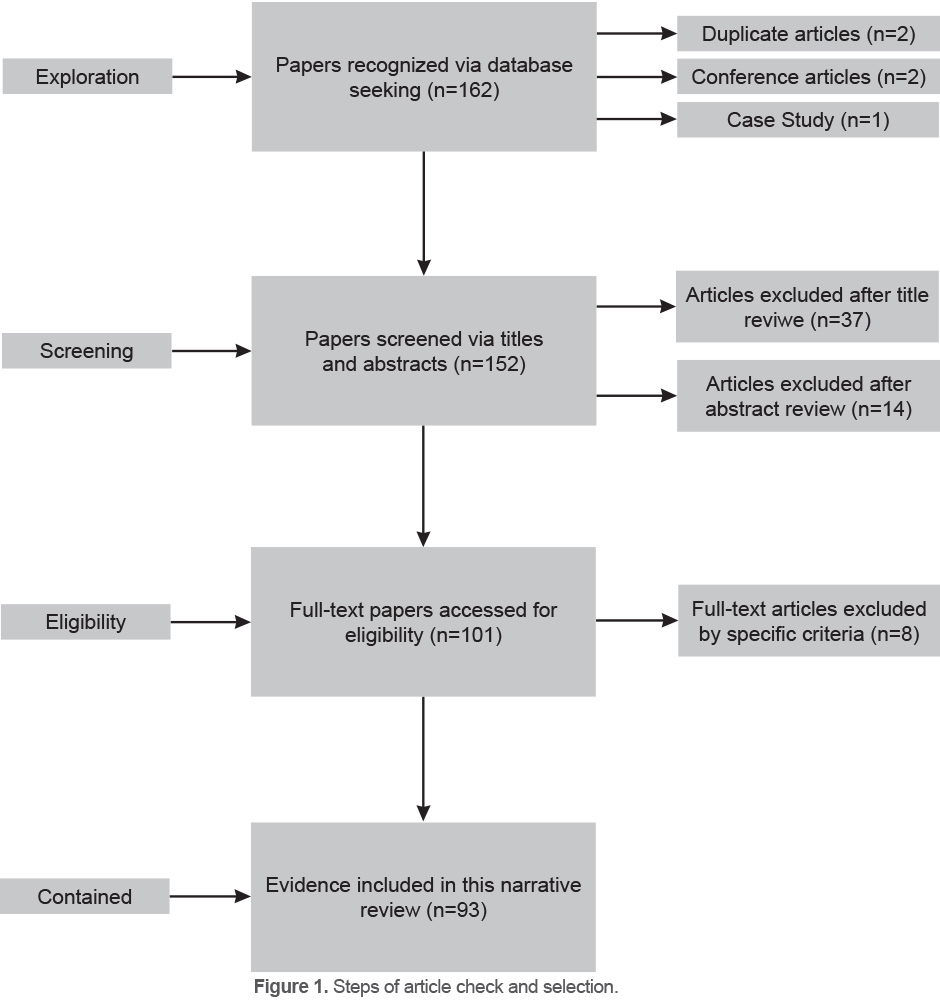
Two researchers independently screened titles, abstracts and full-text articles and selected potentially eligible studies. Data extraction was duplicated for all articles by an independent researcher (CN). Totally, 101 articles (original and review) were eligible regarding the aforementioned criteria. Eventually, after review of full-texts and results and based on the objectives of the research, 93 articles were selected as shown in figure 1.
Results
Experimental components of the papers are shown in figure 1; in general, 162 articles were initially identified from the databases. After removing case studies (1), duplicates (2) and conference papers (7), 152 papers were selected for this review. Then, 37 articles were excluded after the title review and 14 articles were excluded after the abstract review. In addition, 8 articles were excluded following full-text review (Not matched with the purpose of study) and finally 93 papers were selected as the final sample.
Discussion
Regarding the criteria and the selected articles in this review paper, at first, susceptibility of COVID-19 in various normal subjects was evaluated. Then, the involved mechanisms in progression or inhibition as well as severity and mortality of this infection in mentioned groups were described. Table 1 demonstrates all the procedures.
Obesity
The prevalence of overweight or obese individuals in different countries is greater than 20% (24). The association between overweight and obesity with risk of COVID-19 (9,25,26) and related severity, outcomes and mortality was documented (27-30). Obesity is connected in humans and experimental animals with an irregularity in the RAAS system resulting in an overexpression of the ANG II and AT1R axis at the systemic level (31) and in adipose tissue (32). ACE 2 is expressed in adipose tissue and mainly in visceral adipose tissue rather than peripheral subcutaneous tissue (33). Consequently, obese individuals, especially those with increased visceral adipose tissue mass could develop an explosive systemic response with an increased ANG II and AT1R axis and a huge viral load which likely contributes to the development of a more severe form of the disease (2). Also, the underlying metabolic and inflammatory factors in obesity play a noteworthy role in the manifestation of severe lung diseases. Susceptibility to Acute Respiratory Distress Syndrome (ARDS), the primary cause of COVID‐19 mortality, is significantly higher among individuals with obesity (29,34). It should be noted that obesity independently boosts the risk of influenza morbidity and death, likely by impairing innate and adaptive immune responses (35). Furthermore, since the adipose tissue is the main source of inflammatory molecules, including IL-6, it can exacerbate the COVID-19 (35).
Table 1. The cases mentioned in this article are summarized
|
ACE2
|
Susceptibility to Covid-19 |
Severe outcomes |
Subjects |
References |
|
Increase (Compensatory)
|
Increase |
High |
Obese |
(2,11–16,20,21)
|
|
Decrease (compensatory) |
Contradictory evidence |
High |
Elderly |
(12,16,36-50)
|
|
Increase (physiological adaptation) |
Not-established |
Not-stablished |
Athletes |
(19,20,58-65) |
|
Not established |
Increase (Stronger references) |
High (Most of the references) |
Vitamin D deficiency |
(66-80) |
|
Higher in men (Physiological) |
Higher in men |
Higher in men |
Gender |
(21,50-57) |
|
Decrease (physiological) (Stronger references) |
Decrease (Stronger references) |
Low (Stronger references) |
people living in high altitude |
(8,15,81-87) |
|
Decrease in O and increase in A blood group |
Decrease in O blood group and increase in A blood group |
Higher in A blood group and Lower in O blood group |
Blood group (A and O) |
(22,23,88-93) |
Aging
According to an initial clinical report including 138 COVID-19 cases in Wuhan (36), patients admitted to the in ICU were older than non-ICU patients. In a study including 52 critically ill patients in Wuhan, the average age of non-survivors was 64.6 years (37). Another recent study also showed that old age is a risk factor for in-hospital mortality (38). All these investigations propose the elderly are more susceptible to COVID-19 and likely to have poor outcomes (16,39,40). Remarkably, while aging is associated with many diseases, including geriatric syndrome, healthy older adults are also more likely to have severe outcomes after COVID-19 infection (12,39,41-43). Also, aging itself has been greatly linked with worse outcomes, because of the pathophysiological alterations that characterize the respiratory system (44). It has been reported that there is an age-related decline in the clearance of inhaled particles in the small airway region, which seems to be a determining factor for the huge pervasiveness of respiratory symptoms amongst the elderly (45). Also, a progressive and relatively linear increase in nasal cavity volume with aging coupled with an age-dependent reduction of nasal resistance might represent the determinants for a higher prevalence of COVID-19 in elderly population (46). Moreover, novel data shows that while younger subjects may be more prone to infection, lower levels of ACE2 in older cases may prompt more severe clinical behavior of COVID-19 (47), so that ARDS was seen in the preponderance of patients (96.8% of cases) dying in hospitals (47). Immunosenescence represents a recognized characteristic of aging (48). Older adults exhibit a perpetual production of inflammatory mediators and cytokines, also known as ‘inflamm-aging’ (49). Accumulating researches have reported worse outcomes related to the presence of an excessive number of cytokines and inflammation mediators in SARS-CoV-2 infected patients. On the other hand, in early studies, the impact of weakening immune system responses to viral infections in older adults has been widely reviewed. An inverse relationship between CD4/CD8 T-cell ratio and increasing frailty has been summarized and also the amount of circulating ‘competent’ B cells has significantly declined with aging (50).
Gender
It has been reported that male gender is a risk factor for higher severity and mortality in patients with COVID-19, independent of age and susceptibility (50). Regarding the most extensive body of publicly accessible sex-disaggregated data from international reports, although no apparent sex diversity exists in the number of confirmed cases, more men than women have died of COVID-19 in 41 out of 47 countries (51) and the overall COVID-19 case-fatality ratio is around 2.4 times greater amongst men than women. A paper on 3,200 COVID-19 related deaths from Italy noted higher death rates among men than women irrespective of age groups, with men accounting for more than 70% of deaths (52). In another research, it was shown that men and women had the same susceptibility, but men were more prone to dying. Jin et al reported that men with COVID-19 are more at risk for worse outcomes and death regardless of age (53). As mentioned, ACE2 protein is an essential factor for entry of coronaviruses into host cells. It has been shown that circulating ACE2 levels are higher in men than in women (21). This could explain why men might be more susceptible to infection with/as a consequences of COVID-19 (54). On the other hand, men and women vary in both innate and adaptive immune responses, conceivably due to sex-specific inflammatory responses as a result of X-chromosomal inheritance. Hence, women (high density of immune-related genes) commonly mount more robust innate and adaptive immune responses than men which are related to differences in sex chromosome genes and sex hormones such as progesterone and estrogen (52). Moreover, compared with women, men tend to engage in more high-risk behaviors such as psychological and social ones that results in developing COVID-19 (55). For example, risky behaviors in men like tobacco use and alcohol consumption more likely increase the chance of COVID-19 infection (54). Further, men observe preventive measures of handwashing, social distancing, wearing masks, seeking medical care less than women (56,57).
Athletes
It has been well established that exercise can influence the risk of infection by its immunity-enhancing and immunosuppresive effects (58). Also, exercise can modulate the ACE2-ANG (1-7) Mas receptor axis while suppressing the ACE-ANG II-AT1 receptor pathway (19,59). In other words, regular exercise can increase the level of ACE2 and decrease the level of ANG2 in athletes or active people (20,58,60). Therefore, athletes and people who regularly exercise and do physical activity indicate less complications and severe symptoms of SARS-COV-2 such as dyspnea, hospitalization, heart disease and mortality owing to high concentration of ACE2 and lower levels of angiotensin 2 as the leading cause of adaptation to exercise. Consist with our statement and mentioned evidence, the results of one original study examining the relationship of exercising and COVID-19 infection showed that from 1701 athletes in various fields who participated in study, just 99 (5%) suffered from SARS-COV-2 and interestingly from 99 athletes just 4 (5%) cases experienced hospitalization. More importantly, the rate of hospitalization was less than half of the expected rate (61). On the other hand, based on open window theory, athletes or individuals who do high intensity exercise are more susceptible to infection (12,58,62) because of immune system suppression. In contrast, there are no studies as of today that show the correlation between strenuous exercise and hard clinical events (61,63). Moreover, some studies have shown that athletes have greater anti-inflammatory and immunological response and respiratory infection rate is low among them (64,65). Therefore, regarding the mentioned evidence in this part and single original paper conducted in the field, it can be concluded that athletes are less susceptible to SARS-COV-2 and related hard clinical outcomes.
Vitamin D status
The important role of vitamin D in the immune system and its association with various diseases including systemic infections has already been established (66,67). The results of a meta-analysis revealed that serum 25(OH)D levels below 50 nmol/l (i.e.<20 ng/ml) increases the risk of community-acquired pneumonia up to 64% (68), Thus, a hypothesis has been put forward that vitamin D deficiency can increase the severity of COVID-19 infection as well as the mortality rate in these individuals (69,70). The association between vitamin D levels and the severity of COVID-19 mortality has already been reported in several retrospective studies (71,72). Vitamin D follows different mechanisms in reducing the risk of viral infections including COVID-19 and its resulting mortality; these mechanisms include maintaining cell junctions and gap junctions, increasing cellular immunity by decreasing the cytokine storm with an influence on interferon γ and tumor necrosis factor α and regulating adaptive immunity through inhibiting T helper cell type 1 responses and stimulating T cells (69). On the other hand, some studies suggest that vitamin D deficiency strengthens the RAS (73), which can in turn increase the severity of COVID-19 outcomes (74). In the meantime, there is strong evidence that vitamin D supplementation can mitigate the risk of acute respiratory tract infection (75,76). In other words, analysis of data collected from COVID-19 patients in 20 European countries showed that although there is no significant correlation between serum 25(OH)D levels and COVID-19 mortality rate, the incidence of COVID-19 is significantly correlated with serum 25 (OH) D levels (77). Nevertheless, some reports in this regard are mostly contradictory. The results of other studies revealed that the severity of COVID-19 is not correlated with serum 25 (OH) D levels (78,79).
Also, the results of a recent study carried out using the data collected from various regions of the world showed a 15% reduction in severe outcomes of COVID-19 in people with normal serum 25 (OH) D levels (71). Finally, despite uncertainties in this regard, researchers have recommended the use of vitamin D supplementation to prevent the incidence and severe outcomes of this infection. This is particularly crucial during winter and for people who are less exposed to sunlight. It has generally been reported that vitamin D supplementation should be taken into account to maintain a normal circulating levels of 25 (OH) D (75-125 nmol/L) (80). However, it should be noted that consuming vitamin D is dependent on geographical area and the health status of individuals.
High altitude
Over 140 million people worldwide live at high altitudes (>2500 m) (81,82); the physiological adaptations that are generated in these people can affect the risk of various diseases, including respiratory infections. Noteworthy, the results of an epidemiological study showed that people who live at high altitudes are less susceptible to developing COVID-19 (8). Xi et al reported the prevalence of COVID-19 in people dwelling at high altitudes is low probably because of hypoxia-induced physiological adaptations. Besides other factors such as ethnic and genetic population differences, environmental factors about viral transmission, social structure and norms contribute to infection with COVID-19 (83). Further, the change in ACE2 expression in various tissues that are affected by hypoxia is one of the most momentous elements that can affect individuals’ susceptibility to COVD-19 at high altitudes. There are considerable controversies and differences in the results of conducted studies in this field. Some researchers suggested an increase and decrease in ACE1 and ACE2 expression, respectively, as a result of residence at high altitudes after a few days, while other researchers have reported conflicting results (15). Although long-term exposure to hypoxia can theoretically reduce ACE2 expression in various tissues, changes in ACE2 expression in the airway epithelium of individuals living (born and raised) at high altitudes have not been established in any study so far (15). Interestingly, Dang et al have recently stated that exposure to an altitude of 2800 m for 28 days can lead to decrease of ACE2 expression in the heart tissue of male rats (84). Following the finding of this study, several researchers also reported that this problem can affect the expression of ACE2 in pulmonary epithelial cells and the susceptibility to and risk of COVID-19 infection among people dwelling at high altitudes would be reduced (85-87). Finally, it should be noted that considering the wide range of factors that can affect the susceptibility of individuals to COVID-19, more extensive researches should be carried out with a focus just on the role of altitude-induced physiological adaptations among people living in these areas as well as among people who regularly come to these areas.
Blood group
The relationship between blood group and the risk of infectious diseases such as Norwalk virus and Helicobacter pylori infection has been proven (23). Interestingly, some studies have found an association between ABO blood group and the risk COVID-19 and severe outcomes (88,89). Pourali et al in 2020 reported that A blood type was a risk factor for getting COVID-19 while O blood type had a protective role and B and AB didn’t show any significant relationship with COVID-19 (23). Guillon et al reported that S protein expressed by A-positive infected cells shares epitopes of A histo-blood group, and so adhesion of S protein and ACE2 can be suppressed via anti-A normal antibody. The anti-B and anti-A natural antibodies being generated in subjects with O blood type could potentially suppress viral adhesion to cells leading to decreased risk of COVID-19 infection (90); also, since SARS-CoV and SARS-CoV-2 are from the same genus, the similar mechanism might show less susceptibility of O blood type to this disease (23). Also, individuals with O blood type have a lower level of ACE unlike A blood type (91) and the positive relationship between ACE level with hypertension (one of the risk factor of COVID-19) (92) can justify the lower rate of COVID-19 among individuals with O blood type and higher rate of COVID-19 among individuals with A blood type. On the other hand, it has been shown that SARS-CoV-2 attaches to the carbohydrates that specify the ABO blood groups, which are extensively expressed in mucous membrane of respiratory tract; therefore, AB blood group has maximum connection and O blood group the minimum connection with the pathogen (22,93). Furthermore, a research conducted by Dai manifested A blood group antigens have more adhesion molecules that are attached on the vascular wall and they protect P-selectin and Intercellular Cell Adhesion Molecule 1 (ICAM-1) from cleavage which enhance inflammation and adhesion and consequently cause severe SARS-COV-2 infection (91).
Conclusion
Regarding the increased risk of COVID-19 disease and its consequences in the elderly, obese individuals, and men, recommending special and unique preventive measures such as social distancing, maintaining good personal hygiene, as well as doing sufficient physical activity or regular exercise are very important to prevent and reduce the severity of COVID-19 and related mortality. Besides, in order to control this infection and increase immune functions in mentioned groups, doing regular moderate-intensity exercise seems to be the most beneficial solution.
Acknowledgements
There was no financial support for this study.
Conflict of Interest
The authors declare no conflict of interest, financial or otherwise.