Document Type : Review article
A theory of the epidemiology of population change was first raised by Abdel R. Omran in 1971 (1-3) and it had originated from the demographic transition model (4,5). Before that, it was suggested other disciplines like fertility, mortality, and migration are influencing factors for population change (6). But progression in science particularly health and deep recognition of diseases demonstrated that epidemiology is remarkably influenced by distribution of disease and death also their outcomes in population groups (1,7,8).
For many years, primary shifts in disease patterns and mortality were categorized in three groups of: 1) The Age of Pestilence and Famine, 2) The Age of Receding Pandemics and, 3) The Age of Degenerative and Man-Made Diseases (1,7,9). The third epidemiologic transition was transition from mortality due to chronic, noncommunicable diseases in comparison to mortality from malnutrition and infectious diseases (10). Therefore, “third stage” of transition has great importance in population aging for example octogenarians (11). Fourth stage of epidemiologic transition was proposed by Olshansky and Ault (2), as the age of delayed degenerative diseases. Mortality from infectious diseases declined and deaths from degenerative diseases prevailed (11,12). Inactivity and obesity was the fifth stage of epidemiologic transition (13). In the last 3 decades, marked increase in overweight and obesity as well as physical inactivity was widespread (14).
COVID-19 pandemic, also known as the coronavirus pandemic with acute lethal pneumonia during late 2019 and early 2020 caused dramatic and eminent epidemiologic alterations around the world (15,16). During this pandemic, dominant pattern of mortality from inactivity and obesity was defeated by COVID-19 induced mortality (15,17-19). The databases including PubMed, Elsevier, MEDLINE, and Google Scholar were assessed regarding COVID-19 and epidemiologic transition separately. The purpose of the study was to discuss about new and ongoing epidemiologic transition, the so called “Corona and Misery“ phenomenon and some of its aspects for population changes and epidemiologic transition particularly in domain of Cardiovascular Diseases (CVD).
Materials and Methods
A literature search was performed between the years 1962 through 2020. PubMed, Elsevier, MEDLINE, and Google Scholar were thoroughly assessed. Also, scientific publications relevant to epidemiologic transition were examined for inclusion in our work. First of all, with the key phrases including “epidemiologic transition” and “epidemiologic transition and cardiovascular” were used. In the third stage, “cardiovascular and COVID-19“ Was used as the key phrase.
Then, some of the articles obtained from the first search strategy were selected, but most of them were related to the second and third search strategy. Published literature regarding epidemiologic trans-
ition and cardiovascular diseases, as well as cardiovascular diseases and COVID-19, including cardiovascular changes in 2020, were reviewed.
Results
Review articles including narrative reviews (n=15), a systematic review and meta-analysis (n=2), cohort studies (n=3), cross‐sectional observational study (n=1), original articles including survey studies (n=4), perspective (n=4), guidelines and guidance (n=3), bulletins including population bulletin, bulletins of WHO and ACC Clinical Bulletin (n=7), clinical investigation (n=1), correspondence (n=2), case reports (n=2), brief report (n=1), position statement (n=1), editorial, editor’s choice and letter to editor (n=9), research papers, social research (n=2), systematic document content analysis (n=1), predictive analytics research (n=2), analytic research (n=1), case series (n=2), scientific reports (n=1), retrospective study (n=1), book chapters (n=1), and position paper (n=1) , were evaluated. Papers without full text, presented at conferences, or published in languages other than English were excluded. Our documentations and review of obtained data revealed significant effects of COVID-19 on various aspects of cardiovascular involvement.
Discussion
Epidemiologic transition in cardiovascular diseases
Shifting burden of CVD has been matter of interest for epidemiologists over years (20).
During recent decade, CVD has been the main cause of death around the world, taking an estimated 17.9 million death per year, an estimated 31% of total deaths worldwide globally (21,22). CVD risk factor data are mentioned as the attributable deaths and attributable Disability-Adjusted Life Years (DALY) by age group, sex, year, and location (22). General increase in global burden of CVD and the distinctive regional shapes, at least in part, have participated in “epidemiologic transition” which encompass these four fundamental stages of Pestilence and Famine, Receding Pandemics, Degenerative and Man-Made Diseases, and Delayed Degenerative Diseases (2,23). During these last two centuries, gradual transition through these basic stages has remarkably shifted the overall mortality from infectious diseases and malnutrition in the Pestilence and Famine (first stage) to death from CVD and malignancy in the third and fourth stages (Degenerative and Man-Made Diseases, and Delayed Degenerative Diseases) (24,25). In recent stage of epidemiologic transition, inactivity and obesity, the raised total caloric intake, and also prevalence of diabetes and obesity increased; but CVD mortality rates decreased slightly in women (Table 1).
Start of COVID-19 crisis in China and wide-spread distribution throughout the world
In last days of 2019, COVID-19 infection was started from China and it spread all over the world, especially South-East Asia, Europe (mainly Italy) and also in some other countries particularly Iran (26,27). Several names were considered for this disease, including Novel Wuhan Coronavirus, 2019 novel coronavirus (2019- nCoV), and COVID-19 (28,29). Finally, World Health Organization (WHO) called this virus as severe acute respiratory syndrome coronavirus 2 (SARS- CoV-2). From clinical point of view, the main target of this virus is respiratory system, which has been explained and described extensively in recent literatures and publications. Common complaints at presentation were dry cough, fever, myalgia, fatigue, dyspnea, anorexia, and diarrhea and nausea as atypical presentations. As the disease progressed, some major complications like ARDS, arrhythmia, and shock were reasons for death in some patients (30).
In addition to huge health damages, it had great harmful social, political, economic, and cultural impacts, which were very ominous and troublesome.
Far-reaching consequences of economic impact of COVID-19 infection around the world
Beyond the widespread outbreak of COVID-19 infection itself and to the efforts to quarantine, this pandemic is regarded as the most pivotal culprit of human health in contemporary century. But apart from all these, COVID-19 had very deep economic impacts in global economy. Extensive efforts for social and physical distancing and prohibiting all transactions from a normal purchase and sales within the community to extensive business exchanges significantly paralyzed the world economy. For example, many international flights were canceled and also local and domestic transfers were tightly controlled and restricted. On the other hand, because of these problems, the tourism industry was severely damaged. This strange lockdown of transports and transactions (domestic and international) hurts the economies of most countries, especially developing ones, so that during these few months, the people of these countries became poorer and poorer.
In parallel with the above-mentioned problems, entire restaurants, commercial, educational and sports institutions were closed and still after a few months, some of the restrictions on these institutions have remained. In summary and undoubtedly, COVID-19 has had a devastating effect on the economic life of all human societies and also on the world economy (31), and this economic turmoil can involve at least part of the epidemiological transition.
Social, health, and hygiene damage of COVID-19 infection
Obtained information from the World Health Organization suggest that the respiratory droplets and contact are the two principal routes of transmission of COVID-19 virus (32). Shortly after the COVID-19 crisis, the world was faced with a crisis of Personal Protective Equipment (PPE) like face masks, as well as disinfectant solutions. In a short time, these became scarce and as a result, their prices skyrocketed. Because of these plights, some special legislation was created. For example, supplying and provision of mask for public access and prohibiting the distribution of masks to unauthorized individuals were some strategies (16). The high cost of alcohol-based solutions as well as disinfectant solutions was another problem that was considered health obstacle of this crisis. In spite of the fact that this crisis (the lack of health and hygiene equipment) has been partially addressed by governments and health officials, the problem is still persisting and it’s getting worse with the start of the next waves .
Another important issue was lack of serious treatment resources in affected countries. Shortage in critical care particularly lack of ventilator and ICU beds were a great disaster. Finally, unfair allocation of medical resources during this crisis was a great challenge in all societies (33). Changes in behavioral habits, such as excessive hand washing, excessive use of disinfectant solutions and detergents, increased skin sensitivities and exacerbation of lung problems caused by these substances are other global harms of these days; so all of them are ongoing outcomes of COVID-19 pandemics.
Six epidemiologic transition, corona and misery
With more scrutiny, a new epidemiological shift seems to be taking place in the world. This is perhaps the sixth epidemiological transition. Because of the problems that arise at this stage, including health, economic and social issues, which caused a lot of misery in the world, it is better to consider a title for this era that expresses these problems. “Corona and Misery“ is perhaps the best description that can be assigned for this stage. Figure 1 shows the list of changes that occurred in sixth epidemiologic transition.
Changes in the pattern of cardiovascular diseases due to COVID-19 infection
In addition to respiratory system as mentioned above, cardiovascular involvement is the utmost important issue in victims of this disease, especially in severe forms. Range of acute cardiac injury in different articles was from 7.2% in severe form of COVID-19 infection and up to 44% in previous studies (30,34). Comprehensive reports of ACC Clinical Bulletin 2020 showed 40% of hospitalized patients with confirmed COVID-19 infection had cardiovascular or cerebrovascular disease (35). On the other hand, with the start of the COVID-19 pandemic, outpatient cardiology visit was dramatically impacted. Despite the administration of telehealth in 2020, there was a fundamental drop in outpatient cardiology care during the first wave of COVID-19 pandemic compared with the same period in the previous years (36).
So, regarding the importance of cardiac involvement in severe form of this infection and accelerated mortality in this subgroups, identification of SARS- CoV-2-induced heart injuries is very precious and it became very important in early detection and effective treatments for these complications. Shortly after the onset of this disease, some changes were happened in presentation and follow up of patients with chronic disease. In field of cardiovascular disease, perceptible changes have occurred that appear to have altered the epidemiology of cardiovascular diseases. Here are some important examples of these modification in epidemiology of cardiovascular diseases.
Reduction in the number of admitted patients with acute heart problems in hospitals
Acute coronary syndrome
Around the world, the COVID-19 pandemic has vigorously influenced cardiology wards, healthcare professionals and particularly poor cardiac patients (37). COVID-19 prevented hospitalization of more than half of patients with heart attacks (due to delayed presentation and also physician reluctance to hospitalize patients) (38-41). Fear of COVID-19 was one of the most significant reason for patients to seek medical attentions (42). A survey by the European Society of Cardiology (43), showed valuable data on the aftermath of the COVID-19 pandemic on hospital admissions for a serious and lethal cardiovascular emergencies, such as ST-Elevation Myocardial Infarction (STEMI), as reported by interventional cardiologists as well as cardiovascular nurses.
This international survey showed at least an 80 % reduction in STEMI presentations based on self-reported perceptions of respondents but 40 % reduction in STEMI presentations by objective evidence from European and the US registries during the COVID-19 outbreak. Lower rate of hospitalization and therefore less patient’s treatment with acute cardiac events, especially acute coronary syndromes is troublesome. For example, reduced admission rate for STEMI in Italy during the COVID-19 pandemic was accompanied by an increase in mortality and also adverse complications (40). Delayed presentations increase incidence of complications, both acute coronary events as well as other cardiac problems like acute decompensated heart failure (44).
Acute heart failure
Second example is deferral of patients with acute heart failure or decompensated heart failure as another great reason for increase in cardiovascular mortality (45,46). In addition, many of these cases were mistaken for COVID-19 infection (47), and it was diagnosed when it was too late to manage acute or exacerbation of heart failure.
Acute problems related to inadequate or poorly controlled anticoagulation
There are other cases related to this late presentation. Postponement of patients taking warfarin in their regular schedule for control of INR caused a lot of problems. For instance, there were some patients with transvalvular gradients of mechanical heart valves due to inadequate use of warfarin and subtherapeutic INR, or some patients with hemorrhage due to high doses of warfarin, inappropriate to INR level. In the meantime, drug interactions related to COVID-19 drugs also increased the susceptibility to bleeding (48-53).
In summary, this issue is a very serious and challenging problem which increases the mortality of heart patients and also imposes high costs on medical systems. In fact, it seems that despite the increase in scientific progress in the field of cardiology, this pandemic has pushed patients back from cardiovascular care. As this crisis continues, these epidemiological changes in cardiovascular disease may be more obvious and furthermore sophisticated to deal.
Shift in management of cardiovascular disease (downgrading of specific therapies)
Primary Percutaneous Coronary Intervention (PCI) by immediate restoration of blood flow to coronary bed is the standard of care for STEMI patients (54).Today, most centers around the world are improving their cardiovascular systems to activate it in all catheterization laboratories (55). Early in the corona crisis, the Centers for Disease Control and Prevention (CDC) recommended postponing elective cardiac procedures (coronary angiography and percutaneous coronary intervention) for preserving resources particularly PPE and hospital beds (56). Preliminary analysis from US and Spain demonstrated about 40% reduction in STEMI activations of cardiac catheterization laboratory in primary PCI capable centers during the early stage of the COVID pandemic (56,57). In fact, in some centers, a shift to thrombolytic treatment increased. This regression from mechanical reperfusion to less effective methods by thrombolytic therapy was parallel with reemergence of some uncommon complications of STEMI and increase in mortality of these patients (44). In spite of ESC guidance (58), and other recent statements (59), for preference of primary PCI over thrombolytic therapy in STEMI, unfortunately this downgrading still continues in some centers explicitly due to fear staff or patients infection with COVID-19.
Use of mechanical circulatory support particularly Extra Corporeal Membrane Oxygenation (ECMO) for COVID-19–related cardiac collapse, as well as respiratory, or combined cardiopulmonary failure (60) was promising, but due to significant number of involved and eligible cases, including COVID-19 related or other non-COVID-19 conditions, fair allocation of resources for pure cardiac patients faced a crisis. So, a shift to traditional medical management for pure heart failure patients was observed again.
Recent analysis of heart transplant patients demonstrated some challenging issues in era of COVID-19. For examples, there was fear of going to hospitals in this group of patients, and immunosuppression-related troubles which could predispose patients to an increased risk of infections as well as adverse consequences of infection. All these limitations have altered classic management of patients waiting for a heart transplant; therefore delays in heart transplants can significantly increase their mortality (61,62).
Another downgrading in interventional cardiology was postponing of all percutaneous valvular interventions with start of COVID-19 pandemic. In spite of incredible improvement in structural heart intervention in recent decade, restriction of these procedures due to this inauspicious outbreak was an undeniable fact.
Stumbling block in Transcatheter Aortic Valve Replacement (TAVR) had negative impact on immediate and short-term survival of patients with critical Aortic Valve Stenosis (AS). In addition, cumulative effect of halt in these kinds of non-emergent procedures had created great assistance in education of the interventional fellows (63,64). In seems that with starting the every peak of COVID-19 infection, the world is witnessing the collapse of these organized programs of structural heart intervention again.
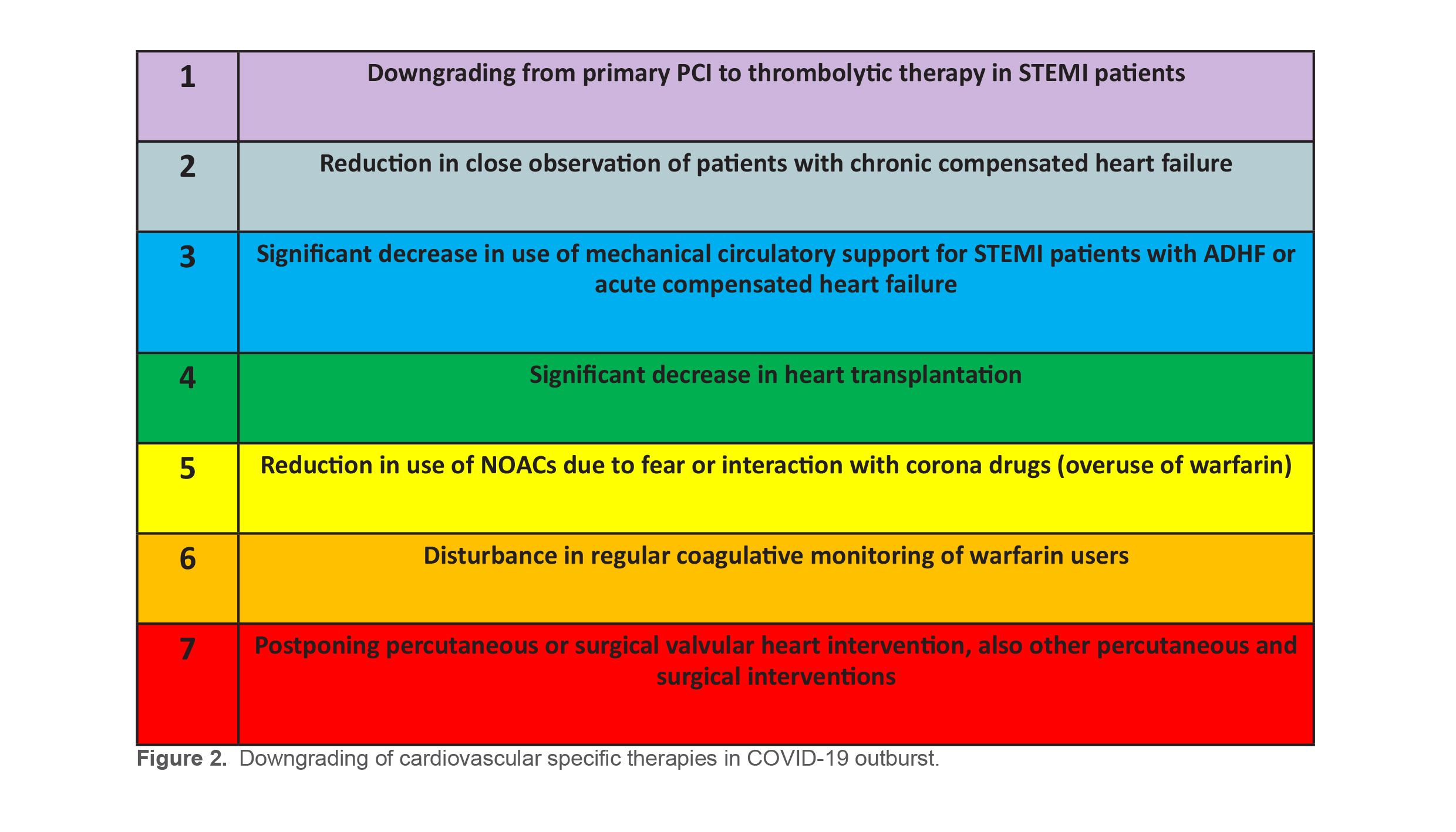
Another concern is anticoagulation options for different circumstances in patients infected with COVID-19. Based on valid recommendations, all admitted patients with COVID-19 must receive pharmacologic thromboprophylaxis against thrombotic com-plications of COVID-19. Low-Molecular-Weight Heparin (LMWH) is necessary for all hospitalized patients with COVID-19 infection (58). LMWH is preferred over heparin and it could be continued ( unless fibrinogen is less than 0.5 g/L or platelet counts are less than 25×109/L) (63). In recent years, Direct Oral Anticoagulants (DOACs) are recommended for many indicated anticoagulation settings, instead of warfarin (64). Despite the preference for DOACs in patients infected with COVID-19, due to the potential and serious interaction of these drugs with COVID-19 drug treatment including Favipiravir, Kaletra (lopinavir/ritonavir), Azithromycin and Hydroxychloroquine, switch to warfarin will be mandatory in recipients of these agents (65). This is a therapeutic dilemma which is also a challenging issue in contemporary era. However, with the continuation of this pandemic or its subsequent peaks, the outlook for management of cardiovascular diseases could be changed to less specific therapies or taking one step back. Figure 2 illustrates downgrading of cardiovascular specific therapies in COVID-19 outburst.
Positive findings of corona era, emergence of new softwares and different ways of online education
Despite all the problems and troubles, it seems that a novel training is emerging. The growth and invention of new software in corona era is astonishing. Outbreak of COVID-19 strengthened online education within a few months, a huge achievement that e-learning authorities have not been able to establish for years. Synchronous (online) and asynchronous (offline) educations widely developed in schools, universities, and higher education centers. Interestingly, people who were completely unfamiliar with e-learning, quickly got used to it and put its use at the forefront of their training programs.
Different and diverse Learning Management Systems (LMS) were developed in schools and universities allowing interaction with the users. LMS also provides the possibility of uploading many educational contents which can be accessed offline. During this short period, multiple platforms were introduced for online courses especially in universities and also for holding congresses. Among them, Zoom (a scalable, cloud-based video conferencing and web conferencing platform enabling online meetings, webinars, file sharing), 3B or Big Blue Button (an open source web conferencing systems), Microsoft Teams (a collaboration tool designed to improve internal communication) are typical examples. And finally, along with the existing global fears and threats from COVID-19, this virtual model of education (computer and web-based) is further developed. Therefore, COVID-19 is an opportunity, not just a threat for fans and advocates of virtual education.
Conclusion
Undoubtedly the COVID-19 pandemic is the most horrible event after the 2nd World War. Obviously, this great criminal of the present century, is making a tremendous alteration in the whole world. Tenacious human efforts have failed to deal with global COVID-19 induced modifications. And finally, in a nutshell, perhaps the sixth epidemiological transition is emerging.
Acknowledgements
I would like to thank all my colleagues who sacrificed their lives in the treatment of patients with COVID-19 infection.
Conflict of Interest
None to declared.
Funding
No funding has been requested for this study.
N Engl J Med 2020 Mar 26;382(13):1194-1196. https://pubmed.ncbi.nlm.nih.gov/32074416/
Int J Environ Res Public Health 2010 Feb;7(2):675-97. https://pubmed.ncbi.nlm.nih.gov/20616997/