Document Type : Short communication
Abstract
Background: Since the outbreak of coronavirus 2019 (COVID-19), identifying risk factors associated with in-hospital mortality has been a global priority. In this study, the purpose was to evaluate the clinical, laboratory, and radiological characteristics of hospitalized patients with COVID-19 to develop a predictive model and scoring system for in-hospital mortality.
Methods: In this retrospective cohort study, 611 adult patients with COVID-19, admitted to Sina hospital were enrolled and followed up.
Results: Out of the total number of 611 patients, 104 patients (17%) deceased during hospitalization, including 75 (12.2%) deaths in ICU and 29 (4.7%) deaths in the wards. After multivariate logistic regression analysis, several characteristics including age >55 years, previous history of malignancy, history of cerebrovascular accident, tachypnea on admission, CRP>54 on admission, D-dimer>1300, and bilateral pulmonary consolidation on chest Computed Tomography (CT) were shown to be the main determinants for stratifying the risk for in-hospital death. The factors were finally considered for introducing a new predictive scoring system for COVID-19 related death.
Conclusion: In-hospital mortality rate in patients with COVID-19 is estimated to be 17%. A new scoring system for predicting in-hospital mortality in such patients was structured based on determinant factors of advanced age, history of malignancy, cerebrovascular accident, tachypnea, raised CRP, raised D-dimer on admission, and bilateral pulmonary consolidation on chest CT scan.
Keywords: COVID-19, Mortality, Risk factors, SARS-CoV-2
Introduction
The 2019 novel Corona Virus (2019-nCoV) was the cause of unexplained viral pneumonia in Wuhan, China in December 2019, and was acknowledged by the World Health Organization (WHO) on January 12, 2020 (1-5). On March 11, 2020, the WHO announced the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) outbreak as a pandemic (6). There have been 133,538,036 laboratory-confirmed cases reported worldwide until April 9, 2021, and 2,894,010 of these patients deceased (7).
Approximately 14% of patients with coronavirus disease 2019 (COVID-19) develop a severe disease needing hospitalization and oxygen support. Further- more, 5% of this population need admission to an Intensive Care Unit (ICU) (8). According to recent studies, the mortality rate is higher among elderly patients and those with a history of comorbidities such as hypertension, diabetes mellitus, and coronary artery disease (1,9,10). Since there is no definitive cure for this disease, early identification of risk factors associated with severe disease and poor clinical outcome can lead to the earlier initiation of appropriate supportive care, thereby reducing mortality. Awareness of patients’ initial characteristics and outcomes is pivotal for health and government officials involved in planning efforts to address local outbreaks.
As one of the hotspots of the disease, Iran has reported 2,006,934 confirmed cases with 63,884 deaths until April 9, 2021 (7). Although many articles have established the clinical features of COVID-19 patients so far (1,2,5,9-16), there are scarce reports regarding the clinical characteristics, incidence, and risk factors associated with in-hospital mortality of Iranian patients diagnosed with COVID-19 (17). In this study, an attempt was made to evaluate the clinical, laboratory, and radiological characteristics of hospitalized patients with COVID-19 to develop a predictive model and scoring system for in-hospital mortality.
Materials and Methods
In this study, 611 adult patients were recruited who were hospitalized with COVID-19 diagnosis in Sina hospital, one of the major tertiary teaching hospitals affiliated to Tehran University of Medical Sciences and a government-designated hospital for COVID-19 treatment. This study was approved by the Ethics Committee of Tehran University of Medical Sciences (IR.TUMS.VCR.REC.1399.005).
The diagnosis of COVID-19 was based on a positive result obtained using real-time reverse-transcriptase polymerase-chain-reaction (RT-PCR) and a routine oropharyngeal swab or endotracheal specimens. Also, some highly suspicious patients were enrolled according to the WHO’s interim guidance and Iranian National Committee of COVID-19 (5,18), including patients with ground-glass opacity alone or ground-glass opacity accompanied with consolidation on chest Computed Tomography (CT), along with symptoms compatible with those in COVID-19 disease. The algorithm of patient care for individuals presenting with respiratory symptoms to Sina hospital emergency department has been published before (19). Demographic characteristics, clinical information (history of hypertension, diabetes mellitus, ischemic heart disease, malignancy, cerebrovascular accident, chronic kidney disease or kidney transplantation), laboratory data, as well as evidence of pulmonary defects on CT were all obtained from the electronic registry record.
The severity of CT scan findings was estimated by visual assessment (mild: ≤25%, moderate: 26-49%, severe: 50-74%, very severe: ≥75% involvement of both lungs). The clinical classifications are as follows: (a) mild to moderate, with mild symptoms up to mild pneumonia; (b) severe type with dyspnea, oxygen saturation ≤ 93%, or >50% lung involvement on imaging; and (c) critical type with respiratory failure, shock, or multiorgan organ dysfunction (20). Patients with at least two complications were considered to have multiorgan damage. The study endpoint was to assess in-hospital mortality defined as the death that occurred during hospitalization due to the development of COVID-19 without other specific reasons.
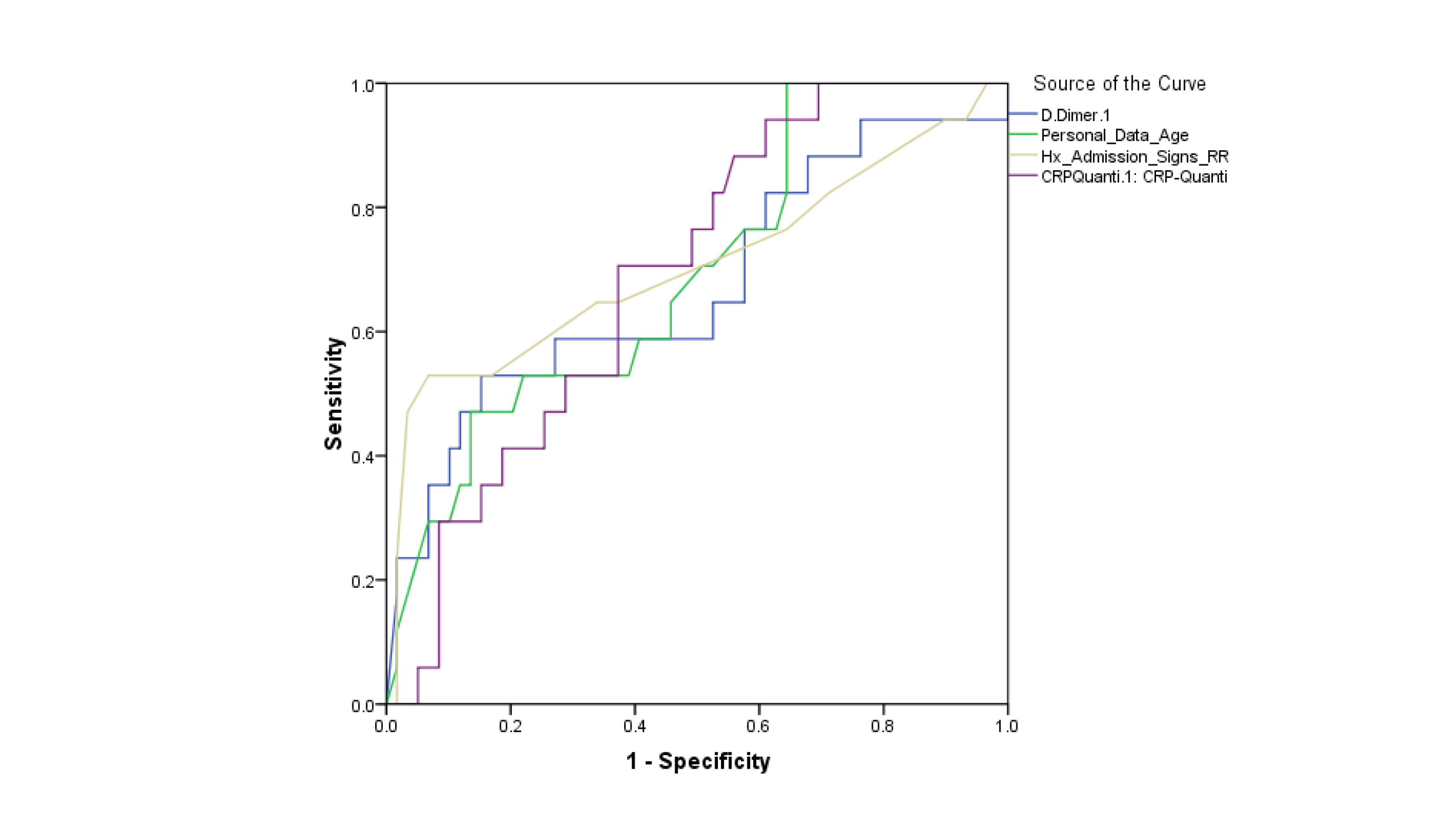
Descriptive data were expressed as median (interquartile range) for continuous variables and number (percentage) for categorical variables. Means of continuous variables were compared using independent group T-tests. Proportions for categorical variables were compared using the Chi-square. Also, univariate and multivariate regression was used to identify risk factors associated with death in patients with COVID-19. The Odds Ratio (OR) along with 95% CI was reported. Variables used in the multivariate model were based on the univariate analysis results (p<0.05). Other significant variables in univariate analysis were excluded due to collinearity or lack of sufficient data in most cases. In order to develop scoring system for risk stratification, the final logistic regression model was used as the method previously described by Sullivan et al (21). In this regard, all study variables obtained to be significant in the multivariate logistic regression model were considered as the categorical binary variables (even continuous variables based on the best cut-off value for each variable with the optimal sensitivity and specificity determined by the area under the Receiver Operating Characteristic (ROC) curve). For all variables structured as categorical, the distance between a variable and its base (reference) category in regression coefficient units was equal to the coefficient’s size. To obtain final scores for each risk factor, the constant corresponding to one point was considered in the risk scoring system. Each risk factor’s point value was calculated by dividing the distance of each risk factor from the base category in regression coefficient units by this constant. The total risk score was obtained by adding up the points for all significant risk factors. The predicted risk associated with each risk score was recalibrated by multiplying it by the observed mortality rate ratio and was finally re-scored as low, moderate, high, and very high risk according to the percentage of quartile of predicted risk. Our recently updated databases with 906 samples were used to evaluate the scoring system’s usefulness and the mortality probability in different groups by using the Kaplan-Meier analysis and the bootstrapping technique. All statistical analyses were performed using SPSS software v22.0 (IBM, USA), and STATA software v13.7 (StataCorp, USA), and P<0.05 was considered statistically significant.
Although the data regarding demographics and history of comorbidities were complete and the rate of missing data for drug history and most laboratory data was less than 15%, the data for Lactate De Hydrogenase (LDH), the high-sensitivity assay for troponin I (hs-cTnI), calcium and phosphorus, chest CT scan, and Erythrocyte Sedimentation Rate (ESR) were not available in 37.1%, 36.3%, 27.3%, 26.4%, and 19.3% of patients.
Results
In this study, the demographic and clinical features of 611 patients were evaluated. They were admitted to the emergency room with COVID-19 diagnosis, with the median age of 57 years (interquartile range: 44-69 years old), and 68.7% of patients were male. Polymerase Chain Reaction (PCR) test was done in 327 patients among whom 140 (42.8%) had positive PCR for COVID-19, with a 27.1% (38 out of 140) mortality rate in patients with a positive PCR test. The rest were highly suspected according to clinical and imaging findings. Almost three-fourths of the patients (75.4%, 343 of 611) were categorized as severe or critical.
The most common symptoms on admission were cough (68.7%) and dyspnea (54.2%), followed by fever at pre-admission (53.5%), myalgia (41.7%), malaise (28.2), gastrointestinal symptoms (25.4%), headache (15.7%), chest tightness (9.7%), loss of consciousness (5.9%), and sore throat (4.3%). Comorbidities were found in 59.2 % of cases, the most significant being hypertension (44.2%), diabetes (37.8%), and cardiovascular disease (23.3%). Severe lung involvement in CT scan was observed in 345 of 455 patients (75.8%). In imaging assessment by CT, bilateral and unilateral ground-glass opacities were revealed in 70.1% and 5.8% of cases, respectively. In addition, bilateral and unilateral consolidation was also found in 10.2% and 6.2% of cases, respectively. Leukocytosis [White blood cells (WBCs more than 10×109/L)] was detected in the initial test in 22.1% of patients, leukopenia (WBCs less than 4×109/L) in 9.7%, and lymphopenia (Lymphocyte count lower than 1.1×109/L) in 42.5% of patients. Thrombocytopenia (Platelet count lower than 100×109/L) was seen in 5.6% of patients. Regarding the medications prescribed during hospitalization, various types of antibiotics were used in 62.2%, antiviral drugs in 93.1%, antioxidants in 12.4%, immunomodulators in 3.6%, and antifungal drugs in 1.0% of the patients.
Out of the total number of 611 patients, 455 (74.5%) patients were hospitalized, 21.1% were admitted to the ICU, and 156 (25.5%) patients were discharged from the emergency room. Almost three-fourths of the patients (75.4%) were classified as severe or critical on admission, and 104 patients (17%) deceased during hospitalization, including 75 deaths (12.2%) in ICU and 29 deaths (4.7%) in the wards. In-hospital mortality rates for COVID-19 were estimated to be 1.0% (2 of 210) in non-severe patients. The mean duration of hospitalization was 5 days (interquartile range:1.0-6.0 days).
Univariate comparison of in-hospital survived and non-survived patients showed the difference in average age, history of hypertension, diabetes mellitus, ischemic heart disease, malignancy, previous lung disease, cerebrovascular accident, the history of metformin or aspirin use, tachycardia or tachypnea on admission, oxygen saturation on admission, and bilateral consolidation of the lung in CT. Among laboratory indices, deceased patients had significantly higher WBC count, higher neutrophil count, blood urea nitrogen (BUN) levels, creatinine, higher potassium, calcium, phosphorus, LDH, ESR, C-Reactive Protein (CRP), serum Aspartate aminotransferase (AST), and D-dimer (p=0.017) on admission (Table 1).
In the multivariate logistic regression, advanced age (p=0.039), history of malignancy (p=0.034), history of cerebrovascular accident (p=0.034), tachypnea (p=0.018), raised CRP (p=0.023), raised D-dimer (p=0.023), and bilateral pulmonary consolidation on CT (p=0.046) were the main determinants of in-hospital mortality (Table 2). In addition, Hosmer and Lemeshow’s test result (Chi-square=3.62, p-value=0.890) indicated a proper fit for this model. In a subgroup analysis of patients with a positive PCR test (N=140), the multivariate regression model indicated similar findings to the main model, except for D-dimer (Table 3) using Hosmer and Lemeshow test result (Chi-square=8.06, p-value=0.427), which indicates a good model fit. For categorizing four continuous variables of age, CRP, D-dimer, and respiratory rate, the area under the ROC curve was analyzed, yielding the best cut-off values of 55 years for age, 18/min for respiratory rate, 1300 μg/L for D-dimer, and 54 mg/L for CRP (Figure1).
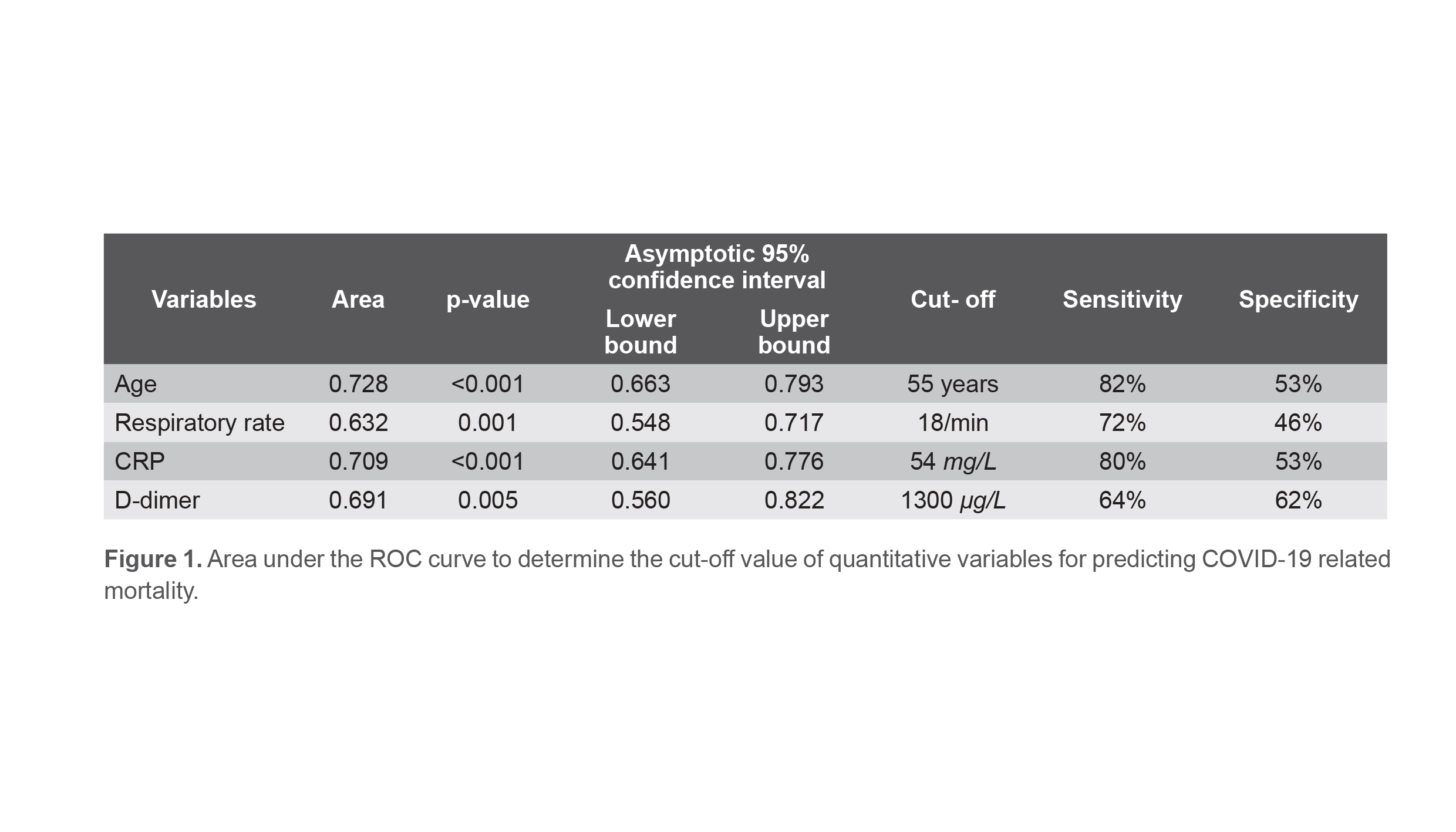
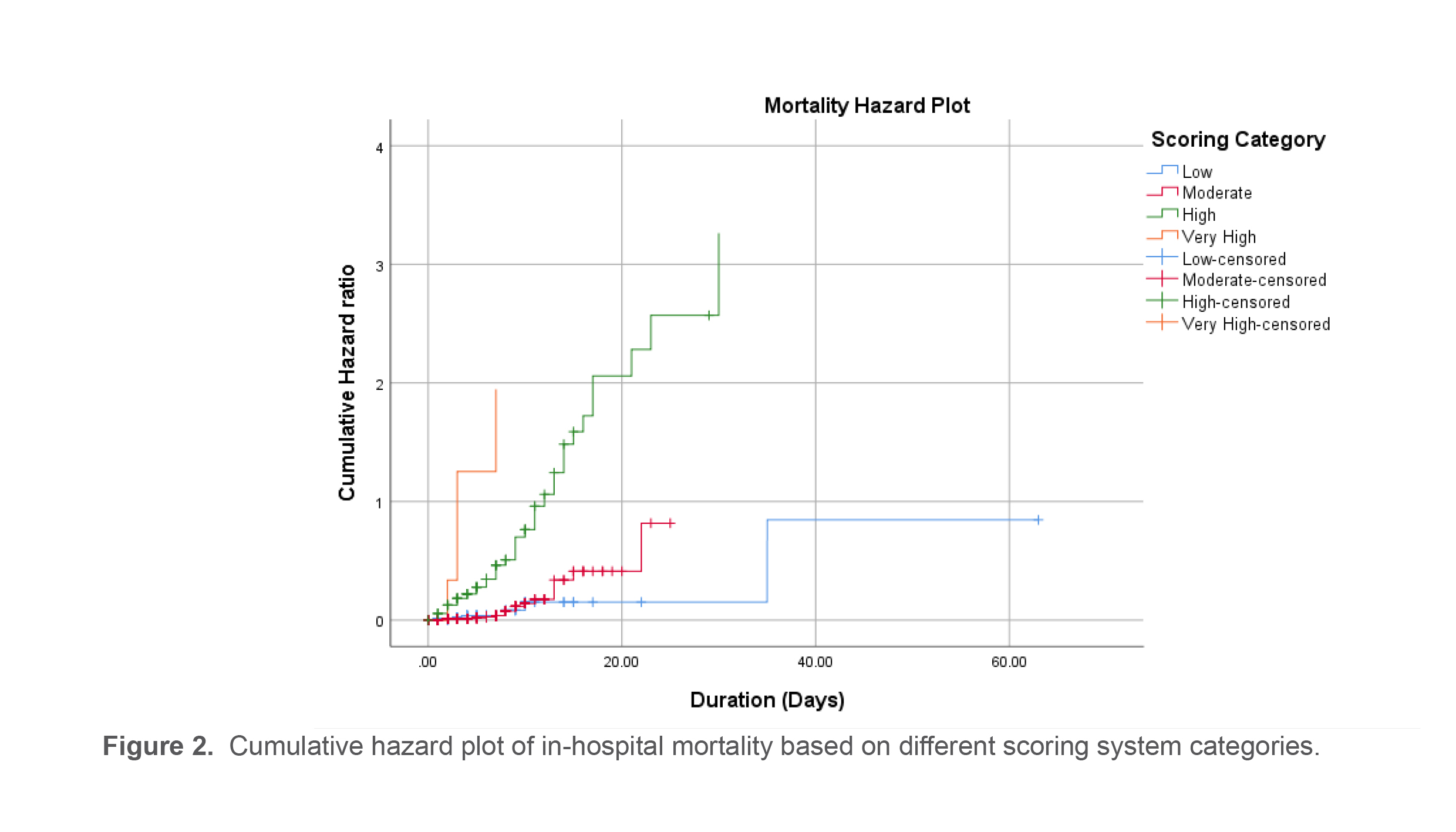
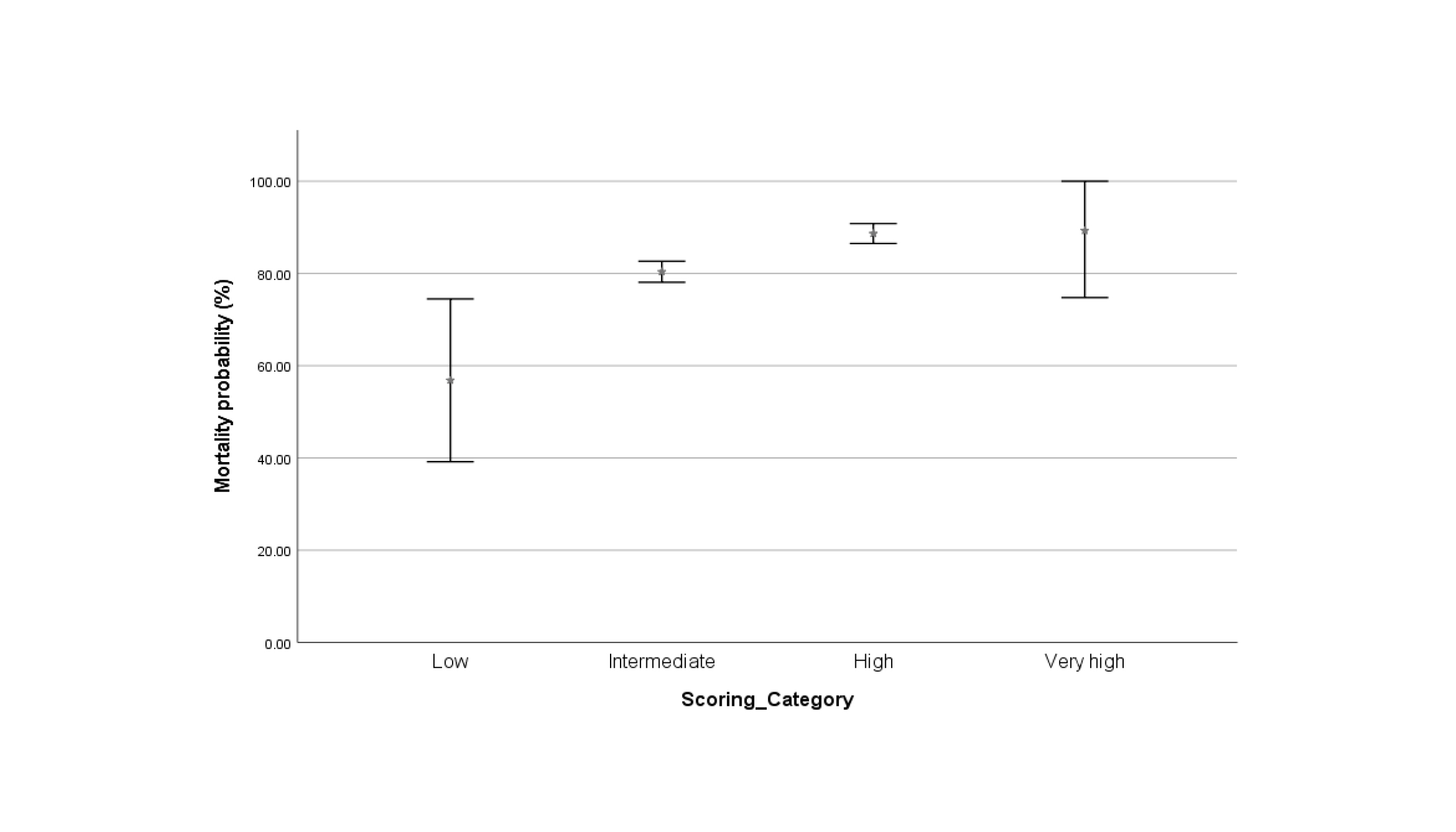
The point scores for the obtained risk parameters in the logistic regression analysis are summarized in Table 4. The minimum total risk score was 0 for a patient without any risk profile. However, the maximum score was 59 for the patients older than 55 years, with a positive history of CerebroVascular Accident (CVA) and a type of malignancy, presented with the symptom of tachypnea, accompanied by elevated CRP and D-dimer on admission, and evidence of bilateral consolidation in chest CT scan. Finally, total risk scores of less than 15, between 15 to 30, between 30 to 45, and higher than 45 were considered low, moderate, high, and very high risks, respectively for in-hospital deaths due to COVID-19 disease. For instance, the patient aged 58 years with previous stroke history and bilateral consolidation in CT view (total risk score of 25) was stratified in moderate risk group for in-hospital deaths. Finally, the scoring system in our updated databases was evaluated. After the Kaplan-Meier analysis, in patients with a higher score, there was a significantly higher probability of in-hospital death (p<0.001) (Figure 2). Also, the mortality probability in each category is presented in (Figure 3).
Table 1. Comparing baseline variables between survived and non-survived groups
|
Item |
Survived group (n=507) |
Non-survived group (n=104) |
p-value |
|
Male gender |
310 (61.1) |
67 (64.4) |
0.531 |
|
Mean age, years |
54.39±15.83 |
69.39±13.07 |
<0.001 |
|
Mean BMI, kg/m2 |
27.48±4.70 |
27.38±4.65 |
0.903 |
|
History of hypertension, % |
168 (33.1) |
62 (59.6) |
<0.001 |
|
History of diabetes, % |
135 (26.6) |
54 (51.9) |
<0.001 |
|
Ischemic heart disease, % |
93 (18.3) |
32 (30.8) |
0.004 |
|
History of malignancy, % |
10 (2.0) |
10 (9.6) |
<0.001 |
|
History of lung disease, % |
28 (5.5) |
15 (14.4) |
0.001 |
|
Chronic kidney disease, % |
24 (4.7) |
8 (7.7) |
0.217 |
|
History of CVA, % |
9 (1.8) |
11 (10.6) |
<0.001 |
|
History of statin use, % |
58 (11.4) |
18 (17.3) |
0.099 |
|
History of metformin use, % |
58 (11.4) |
25 (24.0) |
0.001 |
|
History of aspirin use, % |
58 (11.4) |
21 (20.2) |
0.015 |
|
History of plavix use, % |
20 (3.9) |
6 (5.8) |
0.401 |
|
History of insulin use, % |
20 (3.9) |
6 (5.8) |
0.401 |
|
Bilateral ground-glass opacity in CT, % |
267 (69.9) |
50 (71.4) |
0.322 |
|
Bilateral consolidation in CT, % |
29 (7.6) |
17 (24.3) |
<0.001 |
|
Heart rate, /minute |
87.80±15.44 |
91.73±20.27 |
0.035 |
|
Respiratory rate, /minute |
19.51±7.71 |
24.49±10.63 |
<0.001 |
|
Systolic blood pressure, mmHg |
123.96±20.10 |
123.67±23.77 |
0.907 |
|
Diastolic blood pressure, mmHg |
76.41±10.94 |
74.07±13.02 |
0.078 |
|
Body temperature, ºC |
37.16±1.60 |
37.22±0.99 |
0.731 |
|
Oxygen saturation, % |
91.97±5.64 |
84.00±11.73 |
<0.001 |
|
WBC count, /mm3 |
7.36±3.78 |
10.31±6.17 |
<0.001 |
|
Neutrophil count |
5.48±3.58 |
8.13±4.94 |
<0.001 |
|
Lymphocyte count |
1.45±0.87 |
1.58±3.17 |
0.425 |
|
Serum hemoglobin, g/dL |
13.64±2.01 |
13.24±2.55 |
0.092 |
|
Serum BUN, mg/dL |
30.53±43.04 |
69.46±91.99 |
<0.001 |
|
Serum sodium, meq/L |
135.64±6.94 |
135.46±6.94 |
0.761 |
|
Serum potassium, meq/L |
4.25±0.53 |
4.48±0.75 |
<0.001 |
|
Serum calcium, mg/dL |
8.68±0.67 |
8.37±0.82 |
<0.001 |
|
Serum phosphorus, mg/dL |
3.39±0.85 |
4.00±1.42 |
<0.001 |
|
Serum lactate dehydrogenase, mg/dL |
568.54±225.03 |
804.00±528.52 |
<0.001 |
|
ESR, mm/h |
47.12±29.92 |
56.45±33.75 |
0.008 |
|
CRP, mg/L |
59.41±50.06 |
96.32±54.85 |
<0.001 |
|
CK-MB, μg/L |
47.55±46.32 |
61.31±46.50 |
0.162 |
|
INR |
1.12±0.24 |
1.17±0.19 |
0.211 |
|
Serum AST, mg/dL |
53.69±30.27 |
96.22±20.00 |
<0.001 |
|
Serum ALT, mg/dL |
41.17±10.59 |
62.54±10.61 |
0.001 |
|
Serum ALP, mg/dL |
189.23±126.66 |
219.56±140.80 |
0.057 |
|
Serum creatinine, mg/dL |
1.18±0.82 |
1.60±1.10 |
<0.001 |
|
PH |
7.42±0.07 |
7.39±0.11 |
0.001 |
|
PCO2, mmHg |
38.56±7.67 |
38.00±12.28 |
0.638 |
|
HCO3, mEq/L |
25.12±4.22 |
22.50±4.91 |
<0.001 |
|
Serum D-dimer, μg/L |
1822.31±217.03 |
4006.88±822.17 |
0.017 |
|
Serum ferritin, ug/L |
590.14±52.11 |
852.29±169.25 |
0.083 |
Table 2. The multivariate logistic regression model for determining the main determinant of in-hospital death in COVID-19 patients
|
|
Coefficient |
p-value (Univariate) |
p-value (Multivariate) |
Odds Ratio (OR) |
95.0% CI for OR |
|
|
Lower |
Upper |
|||||
|
Age |
2.500 |
<0.001 |
0.039 |
1.083 |
1.004 |
1.169 |
|
Hypertension |
1.280 |
<0.001 |
0.425 |
2.183 |
0.320 |
14.925 |
|
Diabetes mellitus |
0.218 |
<0.001 |
0.817 |
1.244 |
0.196 |
7.881 |
|
Ischemic heart disease |
1.574 |
0.004 |
0.089 |
4.831 |
0.785 |
29.412 |
|
History of malignancy |
4.088 |
<0.001 |
0.034 |
59.623 |
1.353 |
2.628 |
|
History of lung disease |
0.154 |
0.001 |
0.904 |
1.167 |
0.095 |
14.357 |
|
History of CVA |
5.065 |
<0.001 |
0.034 |
158.315 |
1.457 |
1.720 |
|
History of metformin use |
0.941 |
0.001 |
0.362 |
2.564 |
0.339 |
19.386 |
|
History of ASA use |
0.278 |
0.015 |
0.798 |
1.319 |
0.157 |
11.111 |
|
Heart rate on admission |
0.041 |
0.035 |
0.080 |
1.042 |
0.995 |
1.091 |
|
Respiratory rate on admission |
8.204 |
<0.001 |
0.018 |
1.103 |
1.017 |
1.196 |
|
Oxygen saturation on admission |
-0.093 |
<0.001 |
0.052 |
0.911 |
0.829 |
1.001 |
|
Bilateral consolidation in CT |
2.568 |
<0.001 |
0.046 |
12.987 |
1.051 |
166.067 |
|
WBC count on admission |
-0.126 |
<0.001 |
0.227 |
0.882 |
0.719 |
1.081 |
|
Lymphocyte count on admission |
0.021 |
<0.001 |
0.513 |
1.022 |
0.958 |
1.089 |
|
RBC count on admission |
0.260 |
0.009 |
0.626 |
1.297 |
0.456 |
3.685 |
|
RDW on admission |
0.291 |
0.001 |
0.116 |
1.339 |
0.930 |
1.923 |
|
BUN on admission |
0.006 |
<0.001 |
0.339 |
1.006 |
0.994 |
1.019 |
|
Potassium on admission |
0.446 |
<0.001 |
0.601 |
1.562 |
0.294 |
8.307 |
|
Calcium on admission |
0.745 |
<0.001 |
0.130 |
2.105 |
0.803 |
5.525 |
|
Phosphorus on admission |
0.296 |
<0.001 |
0.548 |
1.345 |
0.511 |
3.540 |
|
ESR1hr |
0.011 |
0.015 |
0.492 |
1.011 |
0.981 |
1.042 |
|
CRP on admission |
2.474 |
<0.001 |
0.023 |
1.019 |
1.003 |
1.035 |
|
AST on admission |
0.014 |
0.001 |
0.088 |
1.014 |
0.998 |
1.030 |
|
Creatinine on admission |
1.064 |
<0.001 |
0.242 |
2.898 |
0.487 |
17.228 |
|
Serum D-dimer |
2.258 |
0.017 |
0.023 |
3.589 |
1.225 |
5.568 |
Hosmer and Lemeshow test result: Chi-square: 3.62, p-value: 0.890.
CVA: cerebrovascular accident, ASA: aspirin, CT: computed tomography, WBC: white blood cell, RBC: red blood cell, RDW: red cell distribution width, BUN: blood urea nitrogen, ESR: erythrocyte sedimentation rate, CRP: C-reactive protein, AST: aspartate transaminase.
Table 3. The multivariate logistic regression model for determining the main determinant of in-hospital death in COVID-19 patients with a positive PCR test
|
|
Coefficient |
p-value (Univariate) |
p-value (Multivariate) |
Odds Ratio (OR) |
95.0% CI for OR |
|
|
Lower |
Upper |
|||||
|
Age |
0.138 |
<0.001 |
0.029 |
1.15 |
1.01 |
1.30 |
|
Hypertension |
1.299 |
0.003 |
0.234 |
3.67 |
0.43 |
31.22 |
|
Diabetes mellitus |
1.205 |
0.057 |
0.270 |
3.34 |
0.39 |
28.39 |
|
History of ASA use |
1.395 |
0.059 |
0.399 |
4.03 |
0.16 |
102.98 |
|
Respiratory rate on admission |
0.283 |
0.009 |
0.040 |
1.33 |
1.01 |
1.74 |
|
Oxygen saturation on admission |
-0.014 |
<0.001 |
0.897 |
0.99 |
0.80 |
1.21 |
|
Bilateral consolidation on CT |
3.784 |
0.032 |
0.061 |
44.01 |
0.84 |
231.8 |
|
WBC count on admission |
-0.525 |
0.002 |
0.058 |
0.59 |
0.34 |
1.02 |
|
RDW on admission |
0.037 |
0.027 |
0.848 |
1.04 |
0.71 |
1.51 |
|
BUN on admission |
0.001 |
0.012 |
0.947 |
1.00 |
0.98 |
1.02 |
|
ESR1hr |
0.004 |
0.065 |
0.835 |
1.00 |
0.97 |
1.04 |
|
CRP on admission |
0.032 |
0.002 |
0.038 |
1.03 |
1.00 |
1.06 |
|
Creatinine on admission |
-0.093 |
0.055 |
0.947 |
0.91 |
0.06 |
13.95 |
Hosmer and Lemeshow test result: Chi-square: 8.06, p-value: 0.427
PCR: polymerase chain reaction, ASA: aspirin, CT: computed tomography, WBC: white blood cell, RDW: red cell distribution width, BUN: blood urea nitrogen, ESR: erythrocyte sedimentation rate, CRP: C-reactive protein.
Table 4. Risk scores for COVID-19 in-hospital mortality
|
Risk score |
Parameters |
|
|
History of CVA |
|
13 |
Positive |
|
0 |
Negative |
|
|
History of malignancy |
|
10 |
Positive |
|
0 |
Negative |
|
|
Bilateral consolidation on CT |
|
6 |
Positive |
|
0 |
Negative |
|
|
Age, year |
|
6 |
>55 |
|
0 |
≤55 |
|
|
Respiratory rate, per minute |
|
20 |
>18 |
|
0 |
≤18 |
|
|
Raised CRP on admission, mg/L |
|
2 |
>54 |
|
0 |
≤54 |
|
|
Raised D-dimer, μg/L |
|
2 |
>1300 |
|
0 |
≤1300 |
|
59 |
Total risk score |
CVA: cerebrovascular accident, CT: computed tomography, CRP: C-reactive protein.
Discussion
There are many estimates of COVID-19 Case Fatality Rate (CFR). The global case-fatality rate in confirmed cases of COVID-19 with 14 days of delay is 2.17% (2,894,010 of 133,538,036 till 9 April) (7,22) while the mortality rate in hospitalized and critically ill patients is expected to be higher. As of today, the in-hospital mortality rate varies from 12.6-22.9% in different countries (11,23-26), with significantly lower mortality in Asia (12.65%) comparing to Europe (22.9%) and America (22.23%) (27). A mortality rate of 17.0% was observed in hospitalized patients. Almost three-fourths of the patients in this study were identified as severe cases, which can justify this relatively high in-hospital mortality. Studies reported that COVID-19 patients in Europe and America were significantly older with a higher incidence of comorbid conditions than patients in Asia, which may explain the difference in CFR and in-hospital mortality between these continents (27).
In line with previous reports (28,29), our results showed the majority of the patients were male (68.7%), which may be related to the more expression of ACE2 receptor in males and the lack of protection of estrogen and X chromosome (28). Nevertheless, gender was not an independent predictor of mortality in our study. The current study also showed advanced age as the main predictor of in-hospital mortality. The defects in T-cell and B-cell function and higher production of type 2 cytokines secondary to aging could lead to uncontrolled virus replication and more extended pro-inflammatory reactions, potentially resulting in more adverse outcomes (29).
This retrospective cohort study identified several risk factors for mortality in Iranian adult patients who were hospitalized with COVID-19 diagnosis. Zhou et al (30) identified several risk factors for death in adults in Wuhan, China. In their study, older age, raised D-dimer, and higher SOFA score on admission were associated with higher odds of in-hospital mortality. Additionally, elevated levels of hs-cTnI and lactate dehydrogenase were more commonly seen in patients with severe COVID-19. In a systematic review, Ma C et al (31) evaluated 30 studies. They reported that old age (≥60years) followed by cardiovascular disease, hypertension, and diabetes were independent factors for the COVID-19 related mortality. In the present study, advanced age, history of malignancy or CVA, tachypnea, raised CRP, raised D-dimer, or the evidence of bilateral consolidation in CT on admission were identified as independent predictors of in-hospital mortality (Table 2). COVID-19 patients with underlying diseases such as hypertension, diabetes mellitus, cardiovascular diseases, malignancies, cerebrovascular accident, immunosuppression, renal failure, and chronic respiratory diseases are especially susceptible to SARS-CoV-2 infection (32,33). In this cohort, comorbidities were present in most patients (67.0%). Besides, a positive history of malignancy or CVA had significantly higher odds of in-hospital mortality. Moreover, the pre-admission history of taking medications in patients with COVID-19 was evaluated and there was no increased risk of mortality with any medication after adjusting other variables (Table 2).
In our analysis, more than two-thirds of patients with COVID-19 experienced respiratory symptoms, and about one-third experienced gastrointestinal symptoms. A substantial proportion of patients presented with cardiac injury, liver, kidney dysfunction, and hyperglycemia. Angiotensin-converting enzyme 2(ACE2) was reported to be expressed in small intestinal epithelial cells, cholangiocytes, and the pancreas (9,34,35), indicating that direct cytopathic effects through an ACE2-dependent pathway may induce the multiorgan injury in patients with COVID-19. Deposition of immune complexes of virus antigen or virus-induced specific immunological mechanisms, besides indirect effects on renal tissue, such as hypoxia, shock, and rhabdomyolysis, may play a role in Acute Kidney Injury (AKI) (36). Meanwhile, regarding cardiac injury, systemic pro-inflammatory cytokine responses, production of procoagulant agents, and hemodynamic disturbances may lead to ischemia and thrombosis (37). In addition, liver impairment, systemic inflammation, elevated levels of pro-inflammatory cytokines, oxidative stress in hepatocytes, liver CD8+ T cells, and hypoxemia play a role in liver enzyme disturbance (38).
One of the limitations of this study was that there was incomplete documentation of several cases. Moreover, PCR testing was performed only in some patients, and all tests were not positive which could be related to test sensitivity and sampling. Also, due to the lack of sufficient diagnostic kits in the early surge of the disease and diagnostic uncertainty, this test was not performed in all patients. Symptoms and imaging findings in cases without available PCR tests were reviewed precisely, and those with symptoms incompatible with COVID-19 were excluded. The findings were measured on admission time and may represent the severity of COVID-19, while the causal relationship between abnormal findings and severity could not be ascertained. Despite significant missing data in some of our database variables, all variables were required to be included in our final assessment. Due to complexity of the COVID-19 management in its early surge as well as the high load of admitted patients, an appropriate database could not be organized for all consecutive patients. Therefore, a high volume of missing data in some variables was inevitable. Furthermore, this study was an observational study with limitations in evaluating the efficacy of corticosteroids and antiviral drugs, and further research, including multi-center studies, is still needed.
Conclusion
In this report, the clinical, laboratory, and radiological characteristics as well as the complications and outcomes of hospitalized COVID-19 patients who deceased were compared with characteristics of those who survived in a tertiary hospital in Iran. It was found that advanced age, history of malignancy, history of cerebrovascular accident, tachypnea, raised CRP, raised D-dimer, and bilateral pulmonary consolidation on CT were the main determinants of in-hospital mortality and finally a new scoring system was introduced for stratifying the risk of death.
Acknowledgements
We acknowledge the assistance of all healthcare workers involved in the diagnosis and treatment process of patients in Sina hospital. We are indebted to the Research Development Center of Sina hospital for its support. The authors are grateful to Dr. Ehsan Saraee for designing, consultation, and technical support of the electronic database registry, Mrs. Masoumeh Taleh, Mr. Saeed Hejrani, and members of the COVID-19 Crisis Management Committee of the Sina hospital for their help and advice. The protocol of this study corresponds to the 2013 Helsinki Declaration and was approved by the Ethics Committee of Tehran University of Medical Sciences (IR.TUMS.VCR.REC.1399.005).
Conflict of Interest
The authors declare that they have no conflict of interest.
Funding
This work was supported by Tehran University of Medical Sciences [Grant number: 99-1-101-47193]. The funding source of the study had no role in the study design, data collection, data analysis, data interpretation, or writing of the manuscript.
Availability of data and material
Data will be available on request
Ethics approval
The protocol of this study corresponds to the 2013 Helsinki Declaration and was approved by the Ethics Committee of Tehran University of Medical Sciences (IR.TUMS.VCR.REC.1399.005). All participants gave written informed consent before inclusion in the study.