Document Type : Original article
Abstract
Background: Kidney transplant recipients are among vulnerable individuals with increased risk of developing COVID-19. Long-term immunosuppression and multiple co-morbidities might affect clinical characteristics of COVID-19 in such patients. In this study, we describe clinical presentations and the incidence of Acute Kidney Injury (AKI) in 9 kidney transplant patients with COVID-19.
Methods: This retrospective case series was conducted on 9 kidney transplant recipients with COVID-19 who were admitted in Imam Khomeini Hospital Complex during the first wave of the disease in Iran from February 20 to 20th April 2020. The diagnosis of COVID-19 infection was confirmed by either positive results of quantitative RT-PCR on nasopharyngeal swabs or typical findings in chest CT scanning.
Results: The median age of patients was 51 years and the graft was functional in all cases before COVID-19 infection. Most patients complained of fever (8 cases), followed by cough (7 cases) and shortness of breath (5 cases). Eight cases had lymphopenia, and leukopenia was reported in 4 cases. AKI occurred in 8 cases. The increase in serum creatinine level resolved partially in most cases, but those who required renal replacement therapy had worse prognosis. Those who survived the acute illness are still alive after more than 16 months with functioning graft.
Conclusion: It was shown in our study that similar to general population, fever and respiratory symptoms are presenting features of COVID-19 in kidney transplant recipients. Lymphopenia is more prominent and the course of COVID-19 infection is more likely to be complicated by AKI in such patients.
Keywords: Acute kidney injury, COVID-19, Iran, Kidney transplantation, Lymphopenia
Introduction
COVID-19, a new viral respiratory illness caused by SARS-CoV-2, emerged in China in late December 2019 and was considered as a global pandemic by World Health Organization (WHO) on March 2020 (1). Significant variability was demonstrated in clinical presentation, course, and prognosis of COVID-19 among infected individuals. Although some patients might be asymptomatic, others would experience variable degree of symptoms including fever, cough, dyspnea, and myalgia (2). Also, the involvement of other organs like gastrointestinal tract, heart, and central nervous system has been reported (3).
Kidney transplant recipients are among individuals with increased risk of developing COVID-19. In a study by Elias M et al in Paris, the incidence of COVID-19 in kidney transplant patients was about 5% which was significantly higher than general population (4). This conferred increased risk might be due to long-term immunosuppressive regimens, which targets both innate and adaptive immunity of these patients. Also, kidney transplant recipients are more likely to be older and have multiple co-morbidities, including diabetes mellitus, hypertension and cardiovascular disorders (5). Clinical characteristics of COVID-19 in kidney transplant recipients, comprising presentation and prognosis, might be different from those reported in other patients.
Soon after the first report of a patient with a definite diagnosis of COVID-19 in Qom, Iran on February 7 2020, the number of patients increased exponentially in all areas of the country (6). Although several studies describe the characteristics of patients in Iran, few reports are available in kidney transplant recipients.
Case series
In this study, we present 9 kidney transplant patients with COVID-19 who were admitted in Imam Khomeini Hospital Complex (IKHC), a tertiary center affiliated to Tehran University of Medical Sciences. The period of study was consistent with the first wave of COVID-19 pandemic in Iran, from 20th February to 20th April 2020. The diagnosis of COVID-19 was confirmed by either positive results of quantitative RT-PCR on nasopharyngeal swabs (5 cases, 56%) or typical findings in chest CT scanning (4 cases, 44%).
After obtaining ethical approval code (IR.TUMS.VCR.REC.1399.363) from our local institute, patients’ data were collected from their files. These data included demographic and clinical characteristics of the patients as well as the results of laboratory and imaging modalities. We defined AKI according to the Kidney Disease Improving Global Outcomes (KDIGO) guideline (7). The last serum creatinine level within 90 days prior to admission was considered as the baseline level.
Median age of the patients was 51 years (ranging from 40 to 72 years) and 66.6% (6 cases) were male. As important co-morbidities, type 2 diabetes mellitus and ischemic heart disease were evident in 4 and 2 patients, respectively. Table 1 describes baseline characteristics of the study population.
Table 1. Baseline characteristics of kidney transplant recipients with COVID-19 infection
|
Case |
Age (Years) /Sex |
Comorbidities |
Number of Kidney Transplant |
Duration from kidney transplant (Months) |
Serum Cr level before admission |
Immunosuppressive Regimen |
|
1 |
51/F |
Negative |
1 |
300 |
1.4 |
MPA Tacrolimus Prednisolone |
|
2 |
40/M |
Negative |
2 |
84 |
1.5 |
MPA Cyclosporine Prednisolone |
|
3 |
52/F |
HLP/HTN |
1 |
84 |
1.9 |
MPA Sirolimus Prednisolone |
|
4 |
44/F |
HTN |
1 |
240 |
2.8 |
MPA Sirolimus Prednisolone |
|
5 |
42/M |
DM/HTN |
1 |
10 |
1.2 |
MPA Tacrolimus Prednisolone |
|
6 |
72/M |
DM/HTN |
1 |
144 |
1.4 |
MMF Sirolimus Prednisolone |
|
7 |
48/M |
IHD |
1 |
72 |
1.8 |
Tacrolimus Prednisolone |
|
8 |
67/M |
DM |
1 |
180 |
1.2 |
MMF Cyclosporine Prednisolone |
|
9 |
69/M |
DM/IHD |
1 |
60 |
1.7 |
MMF Cyclosporine Prednisolone |
F: Female, M: Male, HLP: Hyperlipidemia, HTN: Hypertension, DM: Diabetes Mellitus, IHD: Ischemic Heart Disease, ACEIs: Angiotensin Converting Enzyme Inhibitors, ARBs: Angiotensin Receptor Blockers, Cr: Creatinine, N/A: Not Available, MPA: Mycophenolic Acid (Myfortic), MMF: Mycophenolate Mofetil (Cellcept)
All except one case were recipients of first deceased donor kidney transplant. Case number 2 was a recipient of the second living unrelated kidney transplant. The graft was functional in all cases before being affected by COVID-19. The median time elapsed from transplantation was about 84 months (ranging from 10 to 300 months).
All patients were on treatment by prednisolone. In 6 patients, calcineurin inhibitor (CNI)-based immunosuppression was prescribed; three patients were on tacrolimus and the other 3 were on cyclosporine. For the remaining 3 patients, sirolimus was administered as the immunosuppressive therapy. All except one subject received either mycophenolate mofetil (MMF) or mycophenolic acid (MPA). MMF was withdrawn in case number 7 due to BK virus nephropathy.
Table 2 represents clinical manifestations and the results of laboratory and imaging findings of the subjects. The median time between the onset of symptoms and hospital admission was 10 days (ranging from 4 to 12 days). Fever was the most common presenting symptom, reported in 8 patients. Other symptoms included cough (7 cases), shortness of breath (5 cases), myalgia (4 cases), diarrhea (3 cases), vomiting (1 case), and sore throat (1 case).
Table 2. Clinical manifestations, laboratory data, and imaging results of kidney transplant recipients with COVID-19 infection
|
Case |
Clinical Presentation |
Symptoms Duration before Admission (Days) |
Vital Signs
T (°C) RR BP (mmHg) PR O2sat (at room air) O2sat (supplemental O2) |
WBC (×1000/mm3 ) |
ANC (cells/mm3 ) |
ALC (cells/mm3 ) |
Hb (g/dl ) |
PLT (×1000/mm3 ) |
COVID 19 PCR |
Initial Chest CT-scan /Severity of Lung Involvement |
|
1 |
Fever Cough Dyspnea |
12 |
36.7 22 114/81 114 95% 95% |
11.1 |
9400 |
890 |
9.6 |
399 |
Negative |
Bilateral Patchy Ground Glass Opacity, <10% |
|
2 |
Fever Sore throat Myalgia
|
7 |
38.2 20 120/62 120 82% 96% |
2.8 |
1680 |
870 |
11.5 |
120 |
Positive |
Bilateral Patchy Ground Glass Opacity, <10% |
|
3 |
Fever Cough Diarrhea Vomiting Myalgia |
10 |
36.7 22 110/70 99 88% 97% |
3.5 |
2280 |
950 |
12.1 |
90 |
Positive |
Bilateral Patchy Ground Glass Opacity (predominantly left lung)/ 10-50% |
|
4 |
Fever Cough Dyspnea |
10 |
38.2 19 90/60 86 86% 94% |
10.8 |
9670 |
700 |
9.9 |
88 |
Positive |
Bilateral Patchy Ground Glass Opacity, 10-50% |
|
5 |
Cough Diarrhea
|
4 |
36.8 15 90/65 82 95% 95% |
3.6 |
2520 |
880 |
12.6 |
119 |
Negative |
Bilateral Patchy Ground Glass Opacity, <10% |
|
6 |
Fever
|
10 |
38.4 18 120/80 104 93% N/A |
6.6 |
5520 |
740 |
8.6 |
159 |
Positive |
Bilateral Patchy Ground Glass Opacity, <10% |
|
7 |
Fever Cough Myalgia Diarrhea Dyspnea |
10 |
37.8 18 120/80 70 87% 96% |
7.74 |
5940 |
1100 |
13.2 |
147 |
Negative |
Bilateral Patchy Ground Glass Opacity, <10% |
|
8 |
Fever Cough Dyspnea |
7 |
38.5 26 120/80 95 75% 77% |
6 |
4000 |
1440 |
12.8 |
179 |
Negative |
Bilateral Patchy Ground Glass Opacity, >50% |
|
9 |
Fever Cough Myalgia Dyspnea |
10 |
38.6 18 150/80 82 82% 95% |
3.6 |
2800 |
370 |
15.3 |
111 |
Positive |
Bilateral Patchy Ground Glass Opacity, >50% |
T: Temperature, RR: Respiratory Rate, BP: Blood Pressure, PR: Pulse Rate, O2Sat: Oxygen Saturation, WBC: White Blood Cell, ANC: Absolute Neutrophil Count, ALC: Absolute Lymphocyte Count, PLT: Platelet, PCR: Polymerase Chain Reaction
Table 3. Managements and outcomes of COVID-19 infection in kidney transplant recipients
|
Case |
Immunosuppressive Modification |
Anti-COVID 19 Drugs |
Admission Location |
M.V Required |
RRT Required |
Duration of Admission (Days) |
Outcome |
Cr (Discharge) (mg/dl) |
|
1 |
MPA cessation Hold of Tacrolimus Stress-dose of steroid |
HCQ Atazanavir |
Ward |
No |
No |
7 |
Discharged |
1.8 |
|
2 |
MPA cessation Cyclosporine reduction by 50% Stress-dose of steroid |
HCQ Lopinavir/Ritonavir
|
Ward |
No |
No |
14 |
Discharged |
1.2 |
|
3 |
MPA cessation Sirolimus cessation Stress-dose of steroid |
HCQ Lopinavir/Ritonavir
|
Ward |
No |
No |
13 |
Discharged |
1.4 |
|
4 |
MPA cessation Sirolimus cessation Stress-dose of steroid |
HCQ Atazanavir IVIG |
ICU |
Yes |
Yes |
13 |
Expired |
N/A |
|
5 |
MPA cessation for few days Hold of Tacrolimus Stress-dose of steroid |
HCQ Atazanavir Sofosbuvir |
Ward |
No |
No |
22 |
Discharged |
1 |
|
6 |
MMF cessation for few days Sirolimus cessation Stress-dose of steroid |
HCQ Atazanavir |
Ward |
No |
No |
12 |
Discharged |
1 |
|
7 |
Hold of Tacrolimus Stress-dose of steroid |
HCQ Lopinavir/Ritonavir
|
Ward |
No |
No |
6 |
Discharged |
2.6 |
|
8 |
MMF cessation Cyclosporine cessation Stress-dose of steroid |
HCQ Lopinavir/Ritonavir
|
ICU |
Yes |
No |
6 |
Expired |
N/A |
|
9 |
MMF cessation Cyclosporine cessation Stress-dose of steroid |
HCQ Lopinavir/Ritonavir IVIG |
ICU |
Yes |
Yes |
21 |
Expired |
N/A |
MPA: Mycophenolic Acid (Myfortic), MMF: Mycophenolate Mofetil (Cellcept), HCQ: Hydroxychloroquine, IVIG: Intravenous Immune Globulin, ICU: Intensive Care Unit, MV: Mechanical Ventilation, RRT: Renal Replacement Therapy
Upon admission, 6 patients were febrile. Tachycardia (pulse rate greater than 90 beats per minute) was noted in 5 patients. Oxygen saturation at room air was less than 92% in 6 cases. While 5 patients had unremarkable findings in initial chest CT scanning, imaging modalities revealed bilateral ground glass opacity of more than 50% of both lung fields in two patients (cases number 8 and 9). The extent of lung involvement in case number 4 was estimated to be about 10 to 50%, but the lung opacities rapidly progressed to more than 50% in the following CT scanning.
The median amount of absolute lymphocyte count was 880 per µl (ranging from 370 to 1440 per µl). About 90% of cases (8 out of 9 patients) had lymphopenia with absolute lymphocyte count of less than 1200 per µl. The amount of hemoglobin was less than 10 g/dl in 3 cases, and 5 patients had thrombocytopenia.
As inflammatory markers, CRP (C reactive protein) was checked for cases number 4, 8 and 9 which was 86 mg/dl, 45 mg/dl and 104 mg/dl, respectively. Also, the D-dimer level of case number 4 was 2055 ng/ml and for case number 9 was measured about and 4812 ng/ml. Unfortunately, the inflammatory markers were not assessed for patients admitted in general ward.
Table 3 shows the managements and outcomes of the study population. The median time of hospital admission was about 13 days (ranging from 6 to 22 days). The primary modification in immunosuppressive regimen of the patients was cessation of antimetabolite agents (including MMF, MPA, and sirolimus) and administrating stress doses of corticosteroid. According to the first National Flowchart for Diagnosis and Treatment of COVID-19 released in February 27 2020, all patients received either atazanavir or Kaletra (Lopinavir/Ritonavir) as the initial antiviral agents. Since these protease inhibitor agents impede the metabolism of CNIs, tacrolimus was withheld, cyclosporine dose was reduced throughout the administration of either atazanavir or Kaletra and their serum levels were monitored precisely. Cases number 8 and 9 were critically ill with severe pulmonary involvement; therefore, cyclosporine was withheld for them.
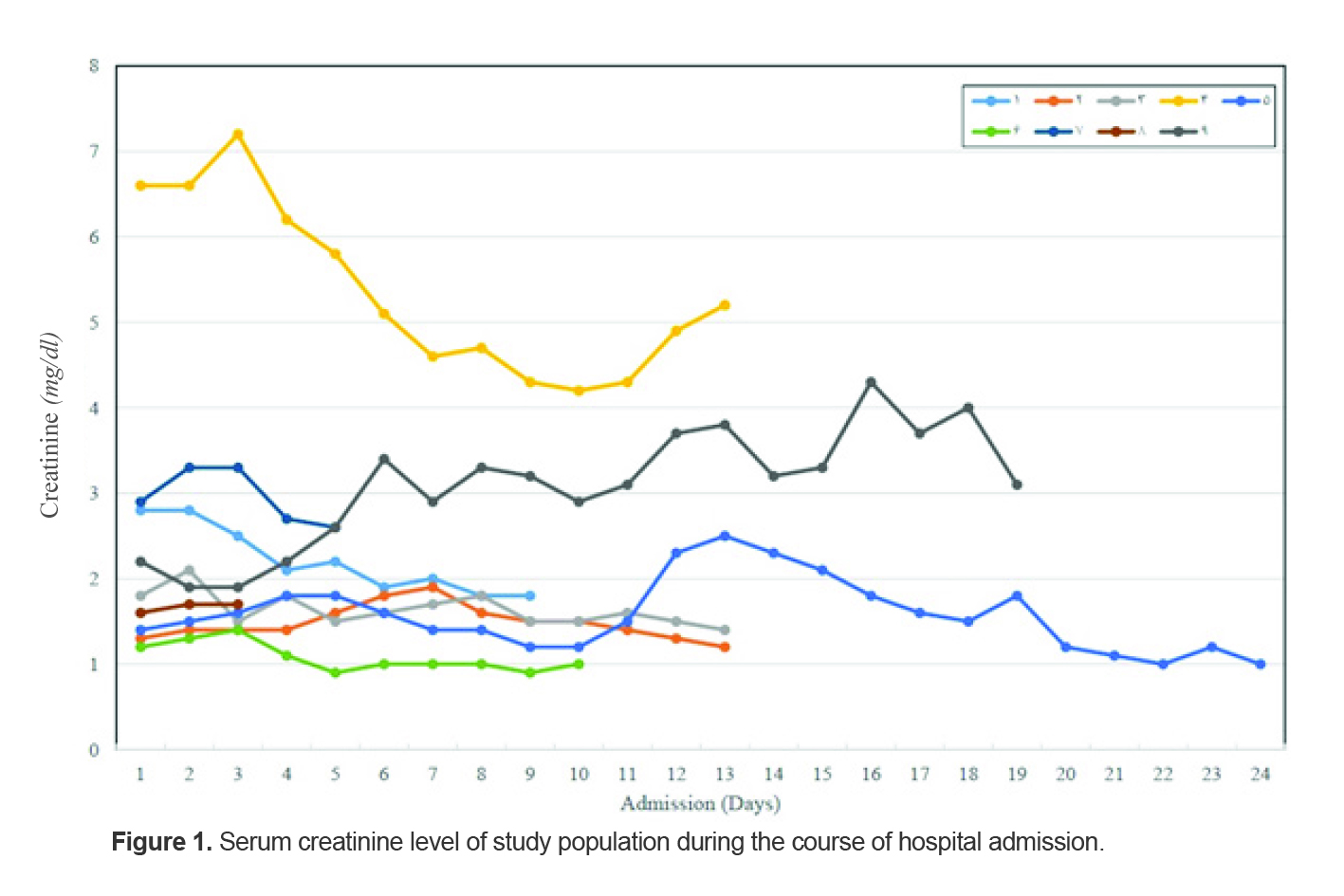
As shown in figure 1,8 patients experienced Acute Kidney Injury (AKI) during the course of COVID-19 infection. Kidney biopsy was not performed for any of these cases to determine the cause of AKI. Cases number 4 and 9 required hemodialysis. AKI was resolved at least partially in other cases.
Those with extensive lung involvement (cases number 4, 8, and 9) were admitted in the Intensive Care Unit and required invasive mechanical ventilation. Unfortunately, these patients died. The remaining cases were discharged with acceptable condition and with no significant impairment in graft function. For further follow up and after about 16 months of their admission, we called the patients at mid-August 2021. Fortunately, all the patients who survived the acute illness are still alive with functioning graft.
Discussion
In this case series, we discussed clinical presentations, management, complications and outcome of COVID-19 infection in 9 kidney transplant recipients who were admitted in our hospital during the first 2 months of COVID-19 pandemic in Iran. The most common presenting symptoms of our patients were fever followed by cough and dyspnea. These findings are in favor of other studies which showed fever and respiratory symptoms as the prominent clinical manifestations of COVID-19 in kidney transplant recipients (8). In congruence with other studies in transplant patients, gastrointestinal symptoms were not a frequent presentation (4,9-12). Although kidney transplant recipients might have atypical clinical manifestations, comparing our results with other studies in general population represents similar clinical presentation of COVID-19 in transplant patients and general population (2,13).
In our study, lymphopenia was the most common laboratory abnormality. These findings mirror other studies in terms of leukopenia and lymphopenia in kidney transplant recipients with COVID-19 (8-12). Several mechanisms were proposed for lymphopenia in COVID-19 patients including T cell infection by SARS-CoV-2 and its interference with T cell expansion (14). Comparing the incidence and severity of lymphopenia in kidney transplant and other patients represents a more pronounced lymphopenia in kidney transplant recipients. It seems that treatment with immunosuppressive agents might predispose such patients to more severe lymphopenia throughout the course of COVID-19.
According to the earlier versions of National Flowchart for Diagnosis and Treatment of COVID-19, all patients of our study received hydroxychloroquine plus either atazanavir or Lopinavir/Ritonavir as antiviral agents (15,16). Soon after, several studies showed inefficiency of Lopinavir/Ritonavir in the treatment of COVID-19 infection. For example, in a trial by Cao B et al on COVID-19 patients, no benefit was reported for Lopinavir/Ritonavir beyond the standard care (17). Due to negative data in clinical trials and unfavorable drug interactions, the 8th National Flowchart for Diagnosis and Treatment of COVID-19 fails to recommend routine use of Lopinavir/Ritonavir for this disease.
Remdesivir, with inhibitory effects on RNA polymerase, should be considered as one the first drugs that was approved by FDA (Food and Drug Administration) for emergency use in the treatment of adult hospitalized patients with COVID-19 in certain situations. Although data are inconsistent, several studies showed the superiority of remdesivir in shortening the time to recovery of hospitalized adult patients (18). Due to lack of such experiences during the study period, none of our patients received remdesivir as the antiviral agent.
Based on expert opinion, published data yet denote to reducing maintenance immunosuppression as a key management in kidney transplant patients with COVID-19. However, the degree of reduction in immunosuppression still remains unclear and concerns regarding alloimmune rejection should be balanced by high mortality of COVID-19 pneumonia in kidney transplant recipients (19). In this study, we stopped antimetabolite agents (including MMF, MPA and sirolimus) upon hospital admission while increasing the amount of corticosteroid to the stress doses. We also reduced the dose of CNIs (including tacrolimus and cyclosporine) and in case of severe COVID-19 pneumonia, we stopped CNI administration.
COVID-19 infection might cause AKI by either direct pathogenic mechanism of SARS-CoV-2 or indirectly as a result of its systemic effects (20). We reported AKI in more than 80% of our patients. In case-series by Monfared A et al and Rahimzadeh H et al, the incidence of AKI in kidney transplant patients with COVID-19 was 57% and 100%, respectively (12,21). In a review of initial published experiences by Moris D et al, AKI was reported in 58.5% of the kidney recipients with COVID-19 (8). On the other hand, AKI occurred in 46% of 3993 hospitalized general patients with COVID-19 (22). Also, a consensus report of the 25th Acute Disease Quality Initiative (ADQI) Workgroup suggested that AKI incidence would be over 20% in hospitalized patients with COVID-19 infection (20).
Compared with general population, it seems that transplant patients are more susceptible to develop AKI during COVID-19 infection. Thus, transplantation might be considered as a major risk factor of AKI in COVID-19 patients. Whether the severity of infection or baseline characteristics of patients might contribute to AKI in kidney transplant recipients is still uncertain. In our study, increase in serum creatinine level was resolved at least partially in most cases, but those who required renal replacement therapy had worse prognosis.
In our case series, all the patients who died had elevated levels of inflammatory markers and two of them experienced severe AKI with the need to Renal Replacement Therapy (RRT). Since none of the survivors required RRT during the course of AKI, it seems that severe AKI with the need to RRT might be considered as a poor prognostic marker in kidney transplant patients with COVID-19.
In this case series, our sample size was small and several other factors (like CRP, D-dimer, and IL6) were not considered for all the patients. Therefore, we could not draw any conclusion about the prognostic factors of our patients. Thus, as a preliminary research, our study served only as an introduction to kidney transplant recipients with COVID-19 in our hospital.
Conclusion
Our case series showed that similar to general population, fever and respiratory symptoms are presenting features of COVID-19 in kidney transplant recipients. Lymphopenia is more prominent and the course of COVID-19 infection is more likely to be complicated by acute kidney injury in such patients.
Acknowledgements
This research was approved by our local ethical committee (IR.TUMS.VCR.REC.1399.363) and has been supported by Tehran University of Medical Sciences (grant no 99.1.190.47650). Authors would like to appreciate the support and constructive comments of the methodologists of research development office, Imam Khomeini Hospital Complex, Tehran, Iran.
Conflict of Interest
The authors have no conflict of interest to disclose.