Document Type : Original article
Abstract
Background: Fatty liver disease is rising as the most common liver disease in recent years. One of the new approaches to manage the disease is the use of intelligent systems. The recommender system is increasingly utilized in managing chronic conditions. This study was performed to identify the common data elements and features of a recommender system for people living with fatty liver.
Methods: This study was a narrative review exploring the minimum data set for a recommender system in fatty liver disease. We aimed to review the current literature evidence to comprehend the specific requirements of the related knowledge. The search was carried out in November 2020 using PubMed, Scopus, Science Direct, and Web of Science databases. We searched the keywords including fatty liver, liver disease, nonalcoholic fatty liver disease, intelligent, smart system, recommender system, minimum data set, data element, and data requirements.
Results: A review of the articles showed that the most common data elements of the administrative category were sex/gender (n=22), age (n=22), and ethnic group/race (n=8). We also identified the clinical data elements and technical features of a recommender system for people living with fatty liver. Based on the findings of this study, “diabetes and glucose status” (n=18), “AST” (n=15), “BMI” (n=13), and “ALT” (n=13) were the most frequent data elements of clinical category. Furthermore, “predicting and identifying” (n=8) was the most common technical feature mentioned in the reviewed articles.
Conclusion: We determined the common elements and features of a recommender system in three different categories: clinical data elements, demographic data elements, and technical capabilities. Using these requirements, it is possible to structure data gathering, medication adherence, and communication with healthcare providers in a standard manner. It is suggested that appropriate policies and national grants be adopted to identify and prioritize a minimum data set to support the healthcare services of people living with chronic conditions.
Keywords: Fatty liver disease, Intelligent system, Minimum data set,
Nonalcoholic fatty liver disease, Recommender system
Introduction
Nonalcoholic Fatty Liver Disease (NAFLD) is an increasing cause of chronic liver disease worldwide. Estimates suggest that about 20–30% of adults in developed countries have excess fat accumulation in the liver (1,2). Individuals with type 2 diabetes and obesity are even at higher risk of getting NAFLD (3). This disease refers to a spectrum of pathological disorders that covers simple hepatic steatosis, steatohepatitis, and cirrhosis that arise despite a lack of alcohol consumption. Moreover, there is significant morbidity and mortality with uncontrolled steatohepatitis, which may progress to advanced hepatic fibrosis, cirrhosis, and hepatocellular carcinoma (4). Therefore, the NAFLD course could follow one or more of its four clinical-pathological entities which are steatosis, nonalcoholic steatohepatitis, advanced fibrosis/cirrhosis, and hepatocellular carcinoma. NAFLD is also associated with atherosclerosis, increased cardiovascular risks as well as mortality (3).
Both genetic factors and lifestyle contribute to the pathogenesis of NAFLD. The ultimate goals of NAFLD management include early diagnosis of the disease, early prevention of further progression of the disease, regression of the disease as much as possible as well as improvement of the underlying metabolic syndrome (5). Despite pharmacological advances, healthy lifestyle changes, including dietary habits and physical activity, remain a fundamental approach for the therapeutic management of NAFLD (6). A 7–10 % weight loss results in improvements in liver enzymes and histology and can be achieved either by dietary changes or by adopting an active lifestyle7. However, implementing lifestyle modification is difficult for patients to achieve success in clinical settings, and maintaining such modifications consistently in daily life can be even more challenging (6,8).
Technological innovations are now commonly incorporated in designing health promotion programs (9). They can address limitations by offering low-cost, highly adaptable, and easily accessible platforms for disseminating lifestyle management interventions (10). They permit real-time data collection, and sharing is increasingly commonplace, enabling researchers to assess multiple health behaviors in various contexts and improvement of health care via non-conventional routes at unprecedented speeds (11). Intelligent systems have recently gained increasing popularity in the promotion of healthy nutrition and physical activity, and prevention of overweight (12). Self-monitoring of dietary intake and physical activity tends to provide the user with the opportunity to set personal goals, to self-monitor their healthy behavior, and to receive tailored feedback (13). By mitigating the barriers associated with committing to repeated in-house nutrition and exercise therapy sessions, mobile apps increase the potential of expanding the reach and efficacy of lifestyle interventions (8). The objective of this study was to identify the minimum dataset for an intelligent recommender system in fatty liver disease.
Materials and Methods
Design
This study was a narrative review exploring the minimum data set for a recommender system in fatty liver disease. We aimed to review the current literature evidence to comprehend the specific requirements of the related knowledge better. A search was conducted identifying the related articles based on the inclusion and exclusion criteria. The included studies were subsequently categorized, and a summary of key points was provided.
Criteria for the selection of studies
The selection of the studies was performed by two independent researchers. We included English-written original articles published from January 1, 2010, to November 15, 2020.
The exclusion criteria were as follows:
− Different types of studies, such as reviews, abstracts, and reports
− No access to the full-text document.
− Non-English articles
− Animal studies
Search strategy
The search was carried out in November 2020 using the PubMed, Scopus, Science Direct, and Web of Science databases. We searched the keywords of fatty liver, liver disease, nonalcoholic fatty liver disease, intelligent, smart system, recommender system, minimum data set, data element, and data requirements on the following search strategy:
A. ”Fatty liver” OR “Liver disease” OR “Nonalcoholic fatty liver disease” [Title/Abstract]
B. ”Intelligent” OR “Smart system” OR “Recommender system” [Title/Abstract]
C. ”Minimum data set” OR “Data element” OR “Data requirements”[Title/Abstract]
D. [A] AND [B]
E. [A] AND [B] AND [C]
Eligibility criteria
We included the most relevant original English studies applying the following exclusion criteria:
1) Non-original studies, including reviews and non-original editorials;
2) Pure laboratory or animal studies not conducted on humans;
3) Case reports and case series;
4) Studies not conducted on the system for people living with nonalcoholic fatty liver disease;
5) Studies not related to the alcoholic fatty liver disease;
6) Abstracts or conference abstracts, or no available full-text.
Literature selection
We screened the titles and abstracts of the retrieved papers to identify studies meeting the inclusion criteria. To analyze the identified articles included in the review, the following variables were utilized: First author, publication date, country, minimum dataset, and other findings.
The appropriate full-text articles were included, and their results were discussed to make the final selection. After reading the full text of all the eligible papers, the researchers made the final decision for each study.
Ethics approval and consent to participate: The present study was extracted from the master thesis with code 9711450002 and code of ethics IR.TUMS.SPH.REC.1400.224 entitled “Design, and development a recommender system for people living with fatty liver disease” conducted at Tehran University of Medical Sciences in 2021. We thank the statistical population and all the participants for taking time to contribute to the study.
Consent to publication
Not applicable
Availability of data and material
The authors stated that all information provided in this article could be shared.
Using the applied systematic search strategies, 698 articles were identified and retrieved.
Results
General specifications
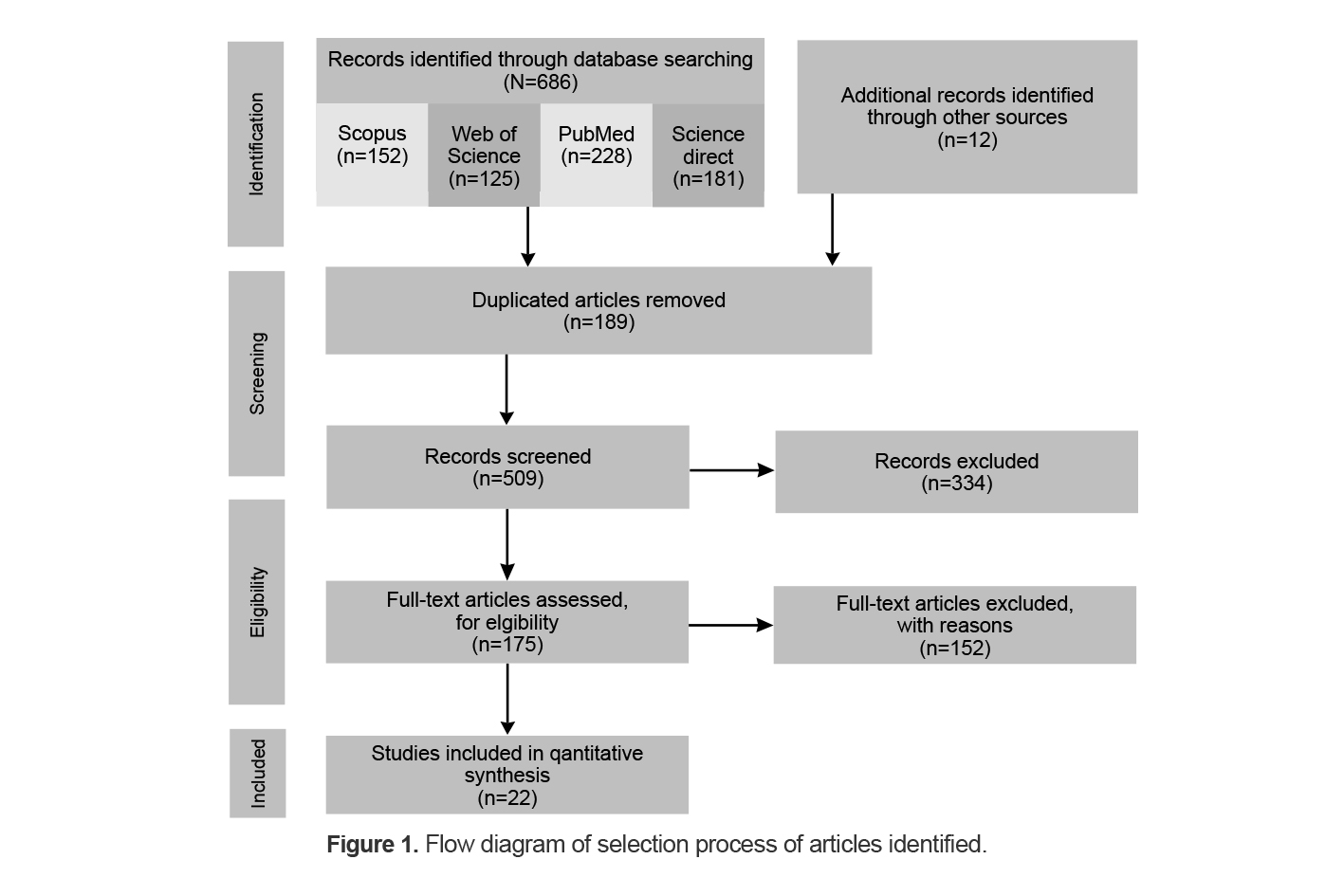
After an initial review of the retrieved articles, 189 duplicates were removed, and the title and abstract of the remaining 509 articles were reviewed. Applying the selection criteria, 486 articles were excluded, and only 22 articles met the inclusion criteria and were included in the final review (Figure 1).
Identifying minimum dataset
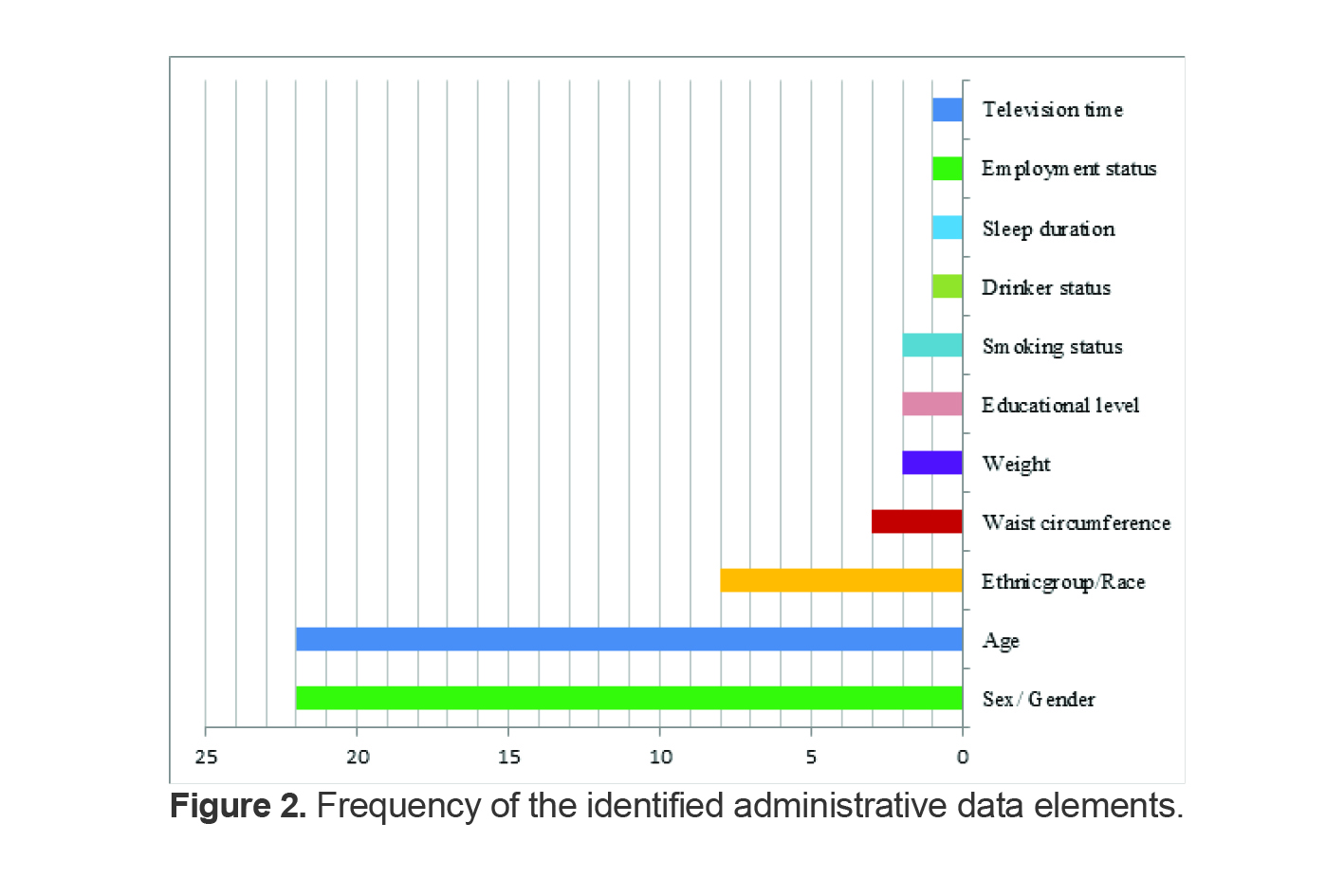
We obtained a set of data elements and features of the intelligent recommender system for people living with fatty liver comprised of three categories: administrative data elements, clinical data elements, and technical capabilities (Table 1). A review of the articles showed that the most common data elements of the administrative category were sex/gender (n =22), age (n=22), and ethnic group/race (n=8). The frequency of the identified administrative data elements is shown in figure 2.
We also identified the clinical data elements and technical features of a recommender system for people living with fatty liver. Based on the findings of this study, “diabetes and glucose status” (n=18), “AST” (n=15), “BMI” (n=13), and “ALT” (n=13) were the most frequent data elements of the clinical category. Furthermore, “predicting and identifying” (n=8) was the most common technical feature mentioned in the reviewed articles (Table 2).
ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body-mass index; HbA1c, glycated hemoglobin; HDL, high-density lipoprotein; LDL, low-density lipoprotein; PLT, platelet; type 2 DM, type 2 diabetes mellitus; A1AT, alpha 1 antitrypsin; AIH, autoimmune hepatitis; AlkPhos, alkaline phosphatse; ARLD, alcohol-related liver disease; DILI, drug-induced liver injury; HBV, hepatitis B virus infection; HCV, hepatitis C virus infection; PBC, primary biliary cholangitis; INR: international normalized ratio; eGFR: estimated glomerular filtration rate;GOT: glutamic-oxaloacetic transaminase; GPT: glutamic-pyruvic transaminase
Table 1. Identified minimum dataset of intelligent recommender systems in fatty liver
|
ID |
The first author (reference) |
Publication date |
Country |
Minimum dataset |
||
|
Administrative |
Clinical |
Technical features |
||||
|
1 |
Forlano, R 1 |
2020 |
London |
Age, Sex, Ethnic group |
BMI, Type 2 DM, Arterial hypertension, Dyslipidemia, PLT, ALT, AST, Total cholesterol, Triglycerides, HDL, LDL, HbA1c, Ferritin |
Machine Learning–Based Quantification |
|
2 |
Lin, YJ 14 |
2020 |
Taiwan |
Age, Sex |
Albumin ,Ammonia ,Blood urea nitrogen, Total bilirubin , Direct bilirubin , Creatinine , C-reactive protein, eGFR ,Glucose ante cibum Serum GOT, Serum GPT, Hemoglobin, Potassium Sodium Platelets , PT Control , PT fibrinogen , PT international normalized ratio, Leukocyte count |
Monitoring System for Predicting Mortality |
|
3 |
Lim, SL 8 |
2020 |
Singapore |
Age , Gender, Ethnicity, Waist circumference, Weight
|
Diabetes, Hyperlipidemia, Hypertension, BMI, ALT, AST, Systolic blood pressure, Diastolic blood pressure |
Intervention by mobile technology on weight loss |
|
4 |
Atabaki-Pasdar, N 15 |
2020
|
Sweden |
Age , Sex, Weight, Waist circumference |
BMI, SBP, DBP, HbA1c, Fasting glucose, Fasting insulin, 2-hour glucose, 2-hour insulin Triglycerides, ALT, AST, Alcohol intake, Liver fat |
Predicting and elucidating by ML |
|
5 |
Ioannou, GN 16 |
2019 |
USA |
Age, Sex, Race/ethnicity
|
BMI, AUDIT-C score: No alcohol, Low-level alcohol use, Unhealthy alcohol use, Diabetes, Substance use disorder, HIV coinfection, Complications of cirrhosis, MELD score, AFP, Hemoglobin, Platelet count, Creatinine, Bilirubin, INR, Albumin, Alkaline phosphatase, FIB-4 score, AST/ALT ratio |
Models estimating risk |
|
6 |
Van Vleck, TT 17 |
2019
|
USA |
Age, Sex, Race
|
Liver serology at base line: aspartate aminotransferase; alanine aminotransferase, Base line comorbidities: diabetes mellitus; hypertension; BMI |
Augmented Intelligence with NLP for Identifying Patients
|
|
7 |
Yang, M 18 |
2019
|
China |
Sex, Age
|
BMI , ALT, AST, AST/ALT ratio, ALP, GGT, TC, TG, HDL, LDL, apoA1, Alb, Tbil, Cholinesterase, Urea, Ferritin, Fasting glucose, PLT, Insulin, HA, PTA, PIIINP, Diabetes, Hypertension |
--- |
|
8 |
Muthuselvan, S 19 |
2018 |
India |
Age, Gender |
tot bilirubin, direct bilirubin, tot proteins, albumin |
-- |
|
9 |
Perveen, S 20 |
2018
|
Pakistan |
Age, Gender |
Abdominal obesity, waist circumference, Lipoprotein level, HDL level, Blood pressure, Fasting Glucose (FG), Diastolic BP, Systolic BP, Unknown disease frequency, COPD frequency Dementia frequency, Depression frequency, Diabetes Mellitus frequency, Epilepsy frequency, Hypertension frequency, Osteoarthritis frequency, Parkinson’s Disease frequency, Triglycerides, BMI |
Diagnosis risk and progression by Machine learning |
|
10 |
Wu, CC 21 |
2018 |
Taiwan |
Age, Gender |
Systolic blood pressure, Diastolic blood pressure, Abdominal Girdle, Triglyceride, HDL-C, Glucose AC, GOT-AST, GPT-ALT |
Prediction using ML
|
|
11 |
Su, GL 22 |
2018 |
USA |
Age, Gender, Race Geographic |
Hepatitis B, Cirrhosis, Cirrhosis Complication, Ascites, Hepatorenal syndrome, Spontaneous Bacterial Peritonitis, Variceal Bleed, Hepatic Encephalopathy, Hepatocellular Carcinoma, Thrombocytopenia, ALT, Bilirubin, Modified Elixhauser Comorbidity, Abdominal CT, Abdominal MRI, Abdominal Ultrasound , Esophagoduodenoscopy, Liver Biopsy Paracentesis |
Virtual Consultations for Veterans with Liver Disease |
|
12 |
Miller, MH 23 |
2018
|
UK
|
Age, Sex
|
BMI, AIH, HCV, HBV, PBC, A1AT, NAFLDnofibrosis, NAFLD with fibrosis, ARLD no fibrosis, ARLD with fibrosis, Gilbert’s syndrome, DILI, Isolated elevated AlkPhos, Haemochromatosis, Wilson’s disease |
Automated assessment |
|
13 |
Trépo E 24 |
2018 |
Belgium |
Age, Sex
|
INR, bilirubin, ceratinne, Albumin |
Predicts Survival of Patients |
|
14 |
Zhou, XD 25 |
2017 |
China |
Age, Sex, Ethnicity |
Cirrhosis: Alcoholic cirrhosis, number Biliary cirrhosis, number Nonalcoholic cirrhosis, number, MELD: Reweight-MELD, Del-Cr-MELD, AKI-MELD, MELD, components: Bilirubin, Creatinine, 48-hour creatinine, Cr48hours/Cr, INR, Loge MELD components: Bilirubin, Creatinine, 48-hour creatinine, Cr48hours/Cr, INR |
Remodeling for Predicting Mortality Risk |
|
15 |
Corey, KE 26 |
2016 |
USA |
Age, Gender, Ethnicity
|
BMI, Diabetes mellitus, Hypertension, Family history of CVD, Renal failure, LDL, HDL, Albumin, Sodium |
Using an Electronic Medical Records Database to Identify NAFLD |
|
16 |
Meng, G 27 |
2016 |
China |
Age, Sex, Physical activity, Sitting time, Smoking status, Drinker status, Sleep duration, Educational level, Employment status, Television time |
BMI, ALT, Total energy intake, WC, TC, TG, LDL-C, HDL-C ,SBP, DBP, FBG |
--- |
|
17 |
Goh, GBB 28 |
2015 |
USA |
Age, sex |
Diabetes, Caucasian, HTN, BMI, AST, ALT, Albumin, Platelet ,Serum iron, Ferritin |
Model to predict |
|
18 |
Lesmana, CRA 29 |
2015 |
Indonesia |
Age, Sex, Smoking history |
Body mass index, Systolic blood pressure, Diastolic blood pressure, Fasting blood glucose, Triglyceride levels, Total cholesterol levels, LDL-cholesterol, HDL-cholesterol, Chronic parenchymal liver disease, Serum AST levels, Serum ALT levels |
--- |
|
19 |
Jan-PS 30 |
2014 |
German |
Age, Gender |
AST, ALT, ALT/AST ratio, BMI, Incidence of diabetes |
Non-Invasive Separation with Predictive Modeling |
|
20 |
Montesi, L 31 |
2014 |
Italy |
Age, Gender, Education, Profession, Waist circumference |
Body mass index, Blood glucose Insulin, HOMA-IR, Total cholesterol, HDL-cholesterol, Triglycerides, Systolic pressure Diastolic pressure, Alanine aminotransferase, Gamma-glutamyltransferases, Diabetes, Hypertension, Treated with statins/fibrates, Kotronen index, Fatty liver index, Visceral adiposity index |
--- |
|
21 |
Jan-Peter, S 32 |
2013 |
Germany |
Age, Gender |
BMI , AST, ALT, gamma-GT, LDH, bilirubin |
--- |
|
22 |
Sumida, Y 33 |
2011
|
Japan |
Age, Gender
|
BMI, Obesity, Dyslipidemia, Hypertension, Type 2 diabetes, Hemoglobin, Platelet count, AST, ALT, AST/ALT ratio, GGT, Cholinesterase, Total cholesterol, Triglyceride, Ferritin, FPG, IRI, Hyaluronic acid, Type IV collagen, Histological fibrosis |
Clinical scoring system for predicting steatohepatitis in NAFLD |
Table 2. Frequency of common identified clinical data elements and technical features
|
Clinical |
1. Diabetes and glucose status |
18 |
14,30,20,18,16,22,28,19, 31,23,15,17,20,33,20 |
|
2. AST |
15 |
14,16,17,18,19,20,23,24,30,31,32,33,34,35,36 |
|
|
3. BMI |
13 |
14,16,17,18,19,20,22,25,28,29,31,33,34 |
|
|
4. ALT |
13 |
14,16,17,18,19,20,23,30,31,32,34,35,36 |
|
|
5. Triglycerides |
8 |
14,17,20,23,29,31,33,35 |
|
|
6. HDL |
8 |
14,20,22,23,28,29,31,33 |
|
|
7. Total bilirubin / Direct bilirubin |
8 |
15,18,20,21,24,26,27,34,36 |
|
|
8. Hypertension /Blood pressure/HTN |
8 |
16,19,20,22,28,30,33,35 |
|
|
9. Systolic blood pressure |
7 |
16,17,22,23,29,31,33 |
|
|
10. Albumin |
7 |
15,18,20,21,36,30,28,26 |
|
|
11. Diastolic blood pressure |
7 |
16,17,22,23,29,31,33 |
|
|
12. Total cholesterol |
6 |
14,20,29,31,33,35 |
|
|
13. LDL |
5 |
14,20,28,29,31 |
|
|
14. GGT |
5 |
20,33,34,35,36 |
|
|
15. HbA1c / Hemoglobin |
5 |
14,15,17,18,22 |
|
|
16. Ferritin |
4 |
14,20,30,35 |
|
|
17. Creatinine |
4 |
15,18,26,27 |
|
|
18. Platelet count |
4 |
18,20,30,35 |
|
|
19. Alkaline phosphatase |
3 |
18,25,36 |
|
|
20. Alcohol intake |
2 |
17,18 |
|
|
21. Liver fat |
2 |
17,33 |
|
|
22. Dyslipidemia |
2 |
14,35 |
|
|
23. PLT |
2 |
14,20 |
|
|
24. Hyaluronic acid |
2 |
20,35 |
|
|
25. Serum GOT |
2 |
15,23 |
|
|
26. Serum GPT |
2 |
15,23 |
|
|
27. Sodium Platelets |
2 |
15,28 |
|
|
28. INR |
2 |
18,26 |
|
|
29. Cholinesterase |
2 |
20,35 |
|
|
30. PTA |
2 |
20,15 |
|
|
31. Cirrhosis/Cirrhosis Complication |
2 |
24,27 |
|
|
32. Fatty liver index |
2 |
17,33 |
|
|
Technical |
1. Predicting and identifying |
8 |
15,23,26,27,28,30,32,35 |
|
2. Risk estimating |
2 |
18,22 |
|
|
3. Quantification |
1 |
14 |
|
|
4. Monitoring |
1 |
15 |
|
|
5. Virtual Consultations |
1 |
24 |
|
|
6. Decision support |
1 |
36 |
Discussion
The general recommendations for addressing non-communicable diseases, which are responsible for two-thirds of deaths globally, are mainly related to lifestyle changes, such as diet and physical activity. Challenges with encouraging healthy diets include gathering accurate information about dietary intake and delivering interventions that can influence behavior. Internet technologies offer excellent potential for addressing these challenges (34). Increasing health information needs changes in information-seeking behavior to be observed around the globe.
According to the recent studies, 81% of U.S. adults use the Internet and 59% assert that they have looked online for health information regarding diseases, diagnoses, and different treatments. Thus, patients tend to become active participants in the decision-making process. This change in the thinking process is often referred to as patient empowerment. However, information overload and irrelevant information are major obstacles for drawing conclusions on the personal health status and taking adequate actions. Encountered a large amount of medical information on different channels (e.g., news sites, web forums, etc.), users often get lost or feel uncertain when investigating on their own. In addition, manifold and heterogeneous medical terms pose another barrier for laymen. Medical information available for patient-oriented decision making has increased drastically but is often scattered across different sites. Recommender systems (RS) suggest items of interest to users of information systems or e-business systems and have evolved in recent decades (35). Having patient demographic and health information in a medium that affords sophisticated and rapid analysis to identify tailored treatment solutions, and being able to deliver this information to the provider at the point of care, can transform treatment (36). The aim of this study was to identify the data requirements and technical capabilities of the recommender system for people with fatty liver disease. We identified a demographic category with 11 common data elements including sex/gender, age, ethnic group/race, waist circumference, weight, educational level, smoking status, drinker status, sleep duration, employment status, and television time.
According to the reviewed articles, 104 data elements were identified for the clinical category of the intelligent recommender system for people living with fatty liver. Mehraeen et al, in a related study, by full-text reviewing of 9 related articles, identified and justified the elements in three main categories and 37 subcategories including clinical data elements, technical capabilities, and demographic data elements. According to the findings of this similar study, among the clinical category, 11 data elements and six data elements were selected as the demographic category by the statistical population (37). A structured and accessible clinical data set is a prerequisite for optimum information management and efficient clinical procedures in every healthcare organization(38).
Nhavato et al, in a developmental study, identified requirements of an intelligent system for tracking the care of patients in six categories: data acquisition requirements, telecommunications cost, privacy and data security, text message content, communication, and system scalability. The findings of this similar study showed that using this system could improve the quality of healthcare and facilitate the communication of healthcare organizations (39). According to the findings of this paper, the technical capabilities of an intelligent recommender system for people living with fatty liver need features such as predicting and identifying, quantification, monitoring, risk estimating, virtual consultations, and decision support.
The modern era of computing has stretched its reach to the intensive and efficient usage of Intelligent Techniques (ITs) in bioinformatics. Owing to the uncertainty in medical data sets, deriving comprehensible information becomes a major challenge for physicians. This challenge can lead to an erroneous diagnosis of a disease, which would further lead to improper treatment. Specifically, we can maintain that it would be favorable for patients in case medical experts cross-check their assessment with the help of some decision-making systems. These systems are developed by using intelligent techniques, which resourcefully scrutinize complex and ambiguous data sets. Implementing these ITs for liver disorders is acting as a catalyst in overcoming the overheads and problems faced by doctors. ITs effectively prevail over the inadequacies, help in obtaining better accuracies, and make the systems adaptable. ITs decrease the probability of occurrence of medical errors and reduce the cost, time, and effort needed40. The liver resists early detection, as it functions normally even when partially damaged, making the disease even more alarming because by then it might have suffered eternal damage. This indicates that an early diagnosis of liver disorders becomes a necessity so that in time treatment can be possible. During diagnosis, analyzing complex data set of patients stretches the decision time of doctors. To reduce this time period and effort, decision-making systems are developed using numerous intelligent techniques.
Self-management is known as a crucial key to improving the health outcomes of patients with chronic diseases including NAFLD. However, there is no instrument to measure the level of self-management for patients with NAFLD. Items of the questionnaire were generated based on the guidelines for patients with NAFLD and the Individual and Family Self-Management Theory. A six-factor was extracted from construct validation using exploratory factor analysis: lifestyle management, drinking management, sleep management, health-supplements management, medical treatment compliance, and family support. Healthcare providers should assess and evaluate the level of self-management to provide tailored interventions based on their care needs. This instrument would provide useful information for healthcare providers who assess self-management levels for individuals with NAFLD. In addition, it may be utilized as the indicator of health outcomes in this population41. Moreover, we developed a demographic category with 8 data elements including weight, marital status, gender, age, occupation, and level of education. It is necessary that organized personal information of patients be accessible in every healthcare organization and therefore, the need to develop demographic data elements for managing the individual data is evident.
Conclusion
In this paper, we determined the common elements and features of a recommender system in three different categories: clinical data elements, demographic data elements, and technical capabilities. Using these requirements, it is possible to structure data gathering, medication adherence, and communication with healthcare providers in a standard manner. It is suggested that appropriate policies and national grants be adopted to identify and prioritize a minimum data set to support the healthcare services of people living with chronic conditions. A complementary study to identify the additional requirements such as technology infrastructures and security requirements of a recommender system for fatty liver through a semi-experimental methodology can be an appropriate route to future research on this topic.
Limitations
Given that many studies in the field of recommender system for people living with fatty liver disease were not performed, a great deal of time was spent searching for the related articles.
Conflict of Interest
The authors declare that there is no conflict of interest regarding the publication of this manuscript.