Document Type : Case report
Abstract
Novel COVID-19 has caused a deathful pandemic since 2019 with more than 2.5 million deaths reported around the world by February 2021. Although best known for its effects on respiratory system, it can be responsible for multiple organ damage. Cardiovascular complications are not uncommon meanwhile. However, some cardiac manifestations are also reported, namely: palpitations and chest pain. Acute myocarditis, acute heart failure, acute coronary syndrome, cardiac arrhythmias and thromboembolic events have been the most common cardiovascular complications reported. Meanwhile, more deaths occurred as a result of aortic dissection. Herein, we want to report a silent death in a patient with COVID-19.
Keywords: Acute aortic dissection, COVID-19 complication, Tamponade, Upper respiratory infection
Introduction
The novel coronavirus 2019 beginning from china has caused a pandemic since late 2019, predominantly affecting respiratory system. The most common presentations involve respiratory system and include sore throat, sputum production, dry coughs, sneezing, dyspnea, rhinorrhea and pneumonia (1,2). Other manifestations include weakness and myalgia, gastrointestinal, hepatic and hematologic presentations, anosmia, CNS and neurologic symptoms, fluid and electrolyte derangements and failure of multiple organs (3).
Some cardiac manifestations are also reported, namely: palpitations and chest pain. Acute myocarditis, acute heart failure, acute coronary syndrome, cardiac arrhythmias and thromboembolic events have been the most common cardiovascular complications reported. Meanwhile, more deaths occurred as a result of aortic dissection (4,5). Hereunder we report a silent death according to cardiovascular complication in a patient with COVID-19.
Case report
A 62-year-old female was brought to Shohadaye Tajrish hospital, Tehran, Iran by EMS. Unfortunately, evidence showed patient was dead several hours prior to admission, and resuscitation was of no help.
She had history of chronic hypertension, under control by atenolol and losartan and was also smoker, approximately 20 packs a year. Three days before admission, she left work due to fatigue, low grade fever and coughing; she was found dead thereafter.
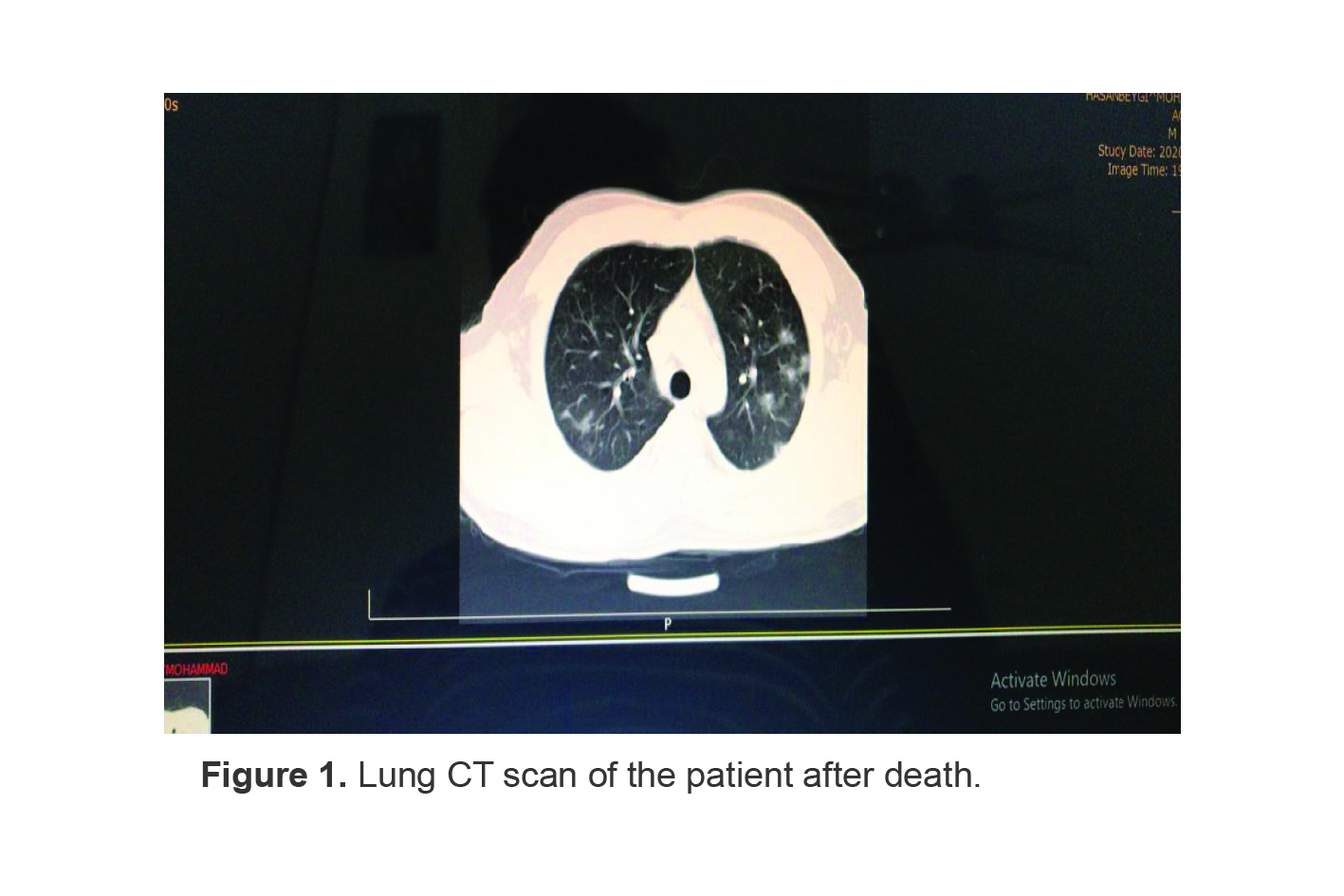
Autopsy and sampling showed positive PCR for COVID-19 and cause of death named to be aortic dissection rupture and tamponade. Lung CT scan was also compatible with coronavirus (Figure 1).
Ethics committee of Shahid Beheshti University of Medical Sciences approved presenting this case (IR.SBMU.RETECH.REC.1399.354).
Discussion
Inflammation plays an important role in the development of aortic dissection, as found in many patients. Although dissection may occur due to collagen tissue diseases, it is often caused by the rupture of an atherosclerotic plaque as the blood passes through the intima-media layers and progresses distally. Also, inflammation plays an important role in this plaque rupture (6).
Type 1 Acute Aortic Dissection (AAD) is a serious clinical condition that requires urgent surgical intervention as it is associated with high mortality and morbidity. Causes such as atherosclerotic foci, degeneration, and tissue diseases may play a role in the emergence of this condition (6).
There is a concern about the relationship between a viral infection and aortic dissection. Recently, an increased admission for aortic dissection and higher hospital mortality of urgent aortic dissection surgery during the influenza season compared with noninfluenza season were noticed. An association between viral syndromes and aortic dissection, especially in winter months has been recently noticed regardless of climate. Inflammatory, immune-mediated injury, increased sympathetic activity or medication uses are some of the reasons that may contribute to aortic dissection in a patient with influenza infection but after influenza vaccination, the rate of dissection was lowered (7).
It is not obvious whether COVID-19 directly results in vascular complications or the preexisting vascular pathologies are being complicated by coronavirus. There are some reports about the coronavirus invading directly to endothelial cells of vessels by dysregulation of angiotensin-converting enzyme 2 receptors or it might be secondary to inflammation and cytokine storm (8,9).
The case we reported was a middle-aged woman with well-controlled hypertension who sacrificed silent death. One hypothesis would be that she had previous unrecognized aortic aneurysm or dissection which ruptured due to frequent cough and hypertension exacerbation secondary to her recent COVID-19 however, the patient’s medical revealed no aortic pathology. Therefore, we would like to suggest the important role of histopathologic changes or inflammatory responses to COVID-19 in cardiovascular complications such as aortic dissection.
Shiva Tabaghi and Mohammadali Akbarzadeh reported a case of Covid-19 who developed with chest pain, loss of consciousness and cardiogenic shock on the 8th day of admission and was diagnosed with type A aortic dissection who expired before being transferred to operating room (7). Patel et al also reported a case of cervical artery dissection associated with coronavirus initially manifested with worsened typical migraine headache (10). In addition, Fukuhara et al described a case of Debakey type 1 aortic dissection presented with severe chest and abdominal pain, who was not tested for coronavirus because of low probability due to clinical criteria; and was diagnosed only after operation and presence of respiratory complications who fortunately survived (11).
In NYC, there was a decline in prevalence of acute type A aortic dissection and concurrent increase in silent deaths in 2020 in comparison to previous years which may be the consequence of lower rates of elective cardiac surgeries during COVID-19 outbreak (12). Similarly, during influenza outbreak an increase in prevalence of aortic dissection was mentioned, which subsequently decreased by initiating the vaccination (13,14).
The main concern is whether coronavirus associated inflammation and immune response may be the casualty for aortic dissection. Yet, there are few studies about such relationship and might need further investigations.
Acknowledgements
We thank Anesthesiology research center of Shahid Beheshti University of Medical Sciences for their collaboration.
Conflict of Interest
The authors declare that there is no conflict of interest
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.