Document Type : Review article
Abstract
Background: Several studies have aimed to discuss the Ultrasonographic (US) findings in the assessment of ulnar neuropathy at elbow; however, the current data are widely heterogeneous and it seems necessary to summarize the original studies to reach a consensus. The goal of this study was to conduct a systematic review on the ultrasound measurements of ulnar nerve cross-sectional area at the elbow among patients with definite diagnosis of ulnar neuropathy.
Methods: The global databases including Medline, Web of Science, Cochrane Library, Google Scholar, and Scopus were deeply evaluated for all eligible English studies. Among the 343 initially retrieved articles, 31 studies met the eligibility criteria and were published from 2000 April to 2019 December. After excluding the non-eligible articles, 18 manuscripts were systematically reviewed with the goal of assessing Cross-Sectional Area (CSA) at different levels regarding the elbow using different techniques and by various types of transducer ranged from 4-18 MHZ. Data extraction was independently performed by two reviewers on some structured data-collection forms.
Results: The summary of following details were systematically reviewed for the included studies: technique of US measurement and type of transducer, as well as cut-off value and diagnostic capability of the ultrasonography. The collected data were analyzed in STATA software using random or fixed-effect models, as effect size measures such as raw or standardized mean differences (MD or SMD).
Conclusion: In the current meta-analysis, it was proved that ultrasound could be a suitable device to diagnose ulnar neuropathy at elbow, with acceptable sensitivity (72.0-76.1%) and specificity (76.1-81.8%) values.
Keywords: Cubital tunnel syndrome, Electrodiagnosis, Nerve compression syndromes, Ulnar neuropathies, Ultrasonography
Introduction
Ulnar nerve involvement at the elbow, also known as cubital tunnel syndrome, is the most common focal neuropathy after the median nerve involvement in carpal tunnel syndrome (1). The location of the involvement is sometimes not easy to determine; despite the high prevalence of Ulnar nerve defect in the elbow, there is a possibility of injury in other areas such as the wrist, forearm, and arm. On the other hand, sometimes the disease can be indistinguishable from C8-T1 root lesion or lower-trunk plexopathy. Finally, determining the precise location of lesion is sometimes impossible in axonal lesions (2).
The ulnar nerve innervates the external flexor muscles of the wrist and carpi, i.e. flexor carpi ulnaris and flexor digitorum profundus; it also supplies the sense of the 5th finger and the ulnar side of the fourth finger. About 8 cm proximal to wrist, a sensory dorsal branch is separated from the main ulnar trunk (3). Various techniques for electrodiagnosis have been suggested to determine the location of the lesion by elucidating the conduction block or slowing (4). The diagnosis of ulnar neuropathy is based on a comparison of the Nerve Conduction Velocity (NCV) of the across-elbow segment to the forearm`s NCV. In fact, a decrease of more than 10 m/s is considered abnormal (5). Therefore, the diagnosis of ulnar neuropathy is mainly on the basis of a physical examination and electrodiagnostic data.
Recently, imaging modalities have helped to make a more accurate diagnosis of nerve entrapments. In this regard, Ultrasound (US) has been widely investigated, as a non-invasive, inexpensive, accessible and real-time method. Several studies have discussed the findings of ulnar nerve ultrasound in patients suffering from cubital tunnel syndrome, as well as the consistency of ultrasound and electrodiagnostic findings. In a number of studies, there was a weak correlation between the findings of electrodiagnosis and nerve ultrasonography (6-8). On the other hand, other investigations such as a well-designed study by H.J Chiou et al (4) have stated that US can accurately detect morphologic changes of the ulnar nerve, and it could be considered as a promising alternative to detect and serial evaluations among patients with cubital tunnel syndrome. Therefore, it is necessary to summarize the final results of current literature to reach a consensus. The main aim of this study was to conduct a systematic review on the sonographic measurements of ulnar nerve cross-sectional area at elbow among patients with cubital tunnel syndrome.
Materials and Methods
Search strategy
This study was performed according to the established methods and in compliance with the PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analysis) Protocol. Also, our review was approved by the ethics committee of Iran University of Medical Sciences (IUMS) under number: IR.IUMS.REC.1399.256. Two investigators searched the manuscript databases including Medline, Web of Science, Google Scholar, Scopus, and Cochrane Central Register of Controlled Trials (CENTRAL) in the Cochrane Library for all eligible studies. Our main keywords were “Ulnar Nerve”, “Ulnar Neuropathy”, “Ultrasonography”, and “Diagnostic Imaging”, which matched the suggested phrases on MeSH database. The studies were restricted to English language. We included all diagnostic studies which utilized US to assess the ulnar nerve’s cross-sectional area among the cubital tunnel patients. We screened both the studies reported as full-text, and those published as abstracts. The exclusion criteria were thus as follows: 1) a lack of clear and quantitative results; 2) non-English studies; 3) lack of access to full-text of manuscripts after delivering the requesting letter to the corresponding authors to have their full data; and 4) case reports and review papers. In cases that only a subset of patients qualified for the current review, and data from a specific sub-population were missing from the original publication, the corresponding authors of the study were contacted to get the required data. If the relevant data could not be obtained, the study was included when the majority of the participants (> 50%) met the inclusion criteria. However, eventually, a sensitivity analysis was performed excluding the studies where < 100% patients met the inclusion criteria.
Table 1. The baseline details of studies described
|
Author, year |
Country; Setting |
No. of Cases |
M/F Ratio in cases |
Mean age of cases |
Ultrasound type |
Transducer (mHz) |
Study type |
|
Alrajeh,2018 [9] |
USA; Neurology |
12 |
NR |
NR |
T3200 |
15 |
Cross-sectional |
|
Ayromlou, 2012 [10] |
Iran; Radiology |
25 |
16/9 15/8 |
Case: 48.6 Control: 42.1 |
Medison multifrequency 7–14 MHZ |
7–14 |
Case-control |
|
Bartels, 2008 [11] |
Netherlands; Neurosurgery |
9 |
7/2 |
51.7 |
iU 22 scanner |
5–17 |
Cross-sectional |
|
Bayrak, 2009 [12] |
Turkey; Neurology |
36 |
25/11 14/7 |
Case: 44.0 Control: 40.0 |
real-time |
12 |
Case-control |
|
Chen, 2017 [13] |
China; Neurology |
100 |
18/22 59/41 |
Case: 59.6 Control: 58.6 |
iU 22 scanner |
15 |
Case-control |
|
Ellegaard, 2015 [14] |
Denmark; Neurophysiology |
41 |
19/22 19/24 |
Case: 51.2 Control: 44.8 |
Siemens ACUSON S2000 |
18 |
Case-control |
|
Kim, 2015 [15] |
South Korea ; Rehabilitation |
25 |
16/9 15/15 |
Case: 50.8 Control: 45.2 |
VOLUSON |
7–12 |
Case-control |
|
Mondelli, 2008 [16] |
Italy; Public Health |
33 |
20/13 10/4 |
Case:50 Control: 50 |
real-time |
5–10 |
Case-control |
|
Ng, 2011 [17] |
Singapore; General Medicine |
46 |
NR |
49.0 |
E Logic book |
12 |
Cross-sectional |
|
Omejec, 2014 [18] |
Slovenia; Neurology |
81 |
41/37 41/37 |
Case: 47 Control: 47 |
ProSound Alpha 7 |
4–13 |
Case-control |
|
Pelosi, 2018 [19] |
New Zealand; Neurology |
135 |
36/12 |
Case: 57 |
SonoSite Edge |
6–15 |
Cross-sectional |
|
Pompe, 2012 [20] |
Netherlands; Neurology |
137 |
47/64 17/37 |
Case: 51 Control: 47 |
|
5–16 |
Case-control |
|
Radhika, 2015 [21] |
Malaysia; Radiology |
64 |
31/33 |
Case: 50 Control: 50 |
Hockey stick |
15 |
Cross-sectional |
|
Rayegani, 2019 [22] |
Iran; Rehabilitation |
32 |
20/12 18/14 |
Case: 45 Control: 44 |
Philips HD6 |
5–12 |
Case-control |
|
Scheidl, 2013 [23] |
Hungary; Neurology |
50 |
12/9 22/65 |
Case: 40 Control: 40 |
Philips HD11XE |
15 |
Case-control |
|
Wiesler, 2006 [24] |
USA; Orthopedic surgery |
14 |
9/6 9/21 |
Case: 45 Control: 45 |
Philips HDI 5000 |
12 |
Case-control |
|
Yalcin, 2014 [25] |
Turkey; Rehabilitation |
38 |
20/18 |
Case: 44 |
Logiq P5 |
7–12 |
Case-control |
|
Zhong, 2012 [26] |
China; Neurosurgery |
278 |
142/136 |
50 |
ATL HDI 500 |
8–14 |
Case-control |
NR: Not Reported; M/F Ratio: male/female Ratio.
Data extraction
Data extraction was independently performed by two reviewers (K.M and P.R) on some structured data collection forms without divergences. We resolved the disagreements by consensus or by involving a third person (N.Y). The data entry phase was doubled checked by comparing the data presented in the systematic review with the data extraction form. The second review’s author spotted check the study characteristics for accuracy against the trial report. The summary of the details for the included studies, assessed by systematically reviewing the manuscripts, were as the following (Table 1): A. Study methods: study design, entire study period, details of any ‘run in’ period, number of study centers, study setting, and date of study; B. Participants: total number of participants, gender and age distributions, the number of patients scheduled for ultrasonography assessment; C. Any quantitative scale and parameters related to ulnar neuropathy; D. Inclusion and exclusion criteria; and E. The details of measurements associated with the sonographic evaluation.
Quality assessment
The study quality was evaluated based on the following criteria: 1) the systematic review and meta-analysis were primarily described and formulated based on the questions; 2) inclusion and exclusion criteria were predefined in the studies as the eligibility criteria; 3) searching the literature was performed according to a systematic and comprehensive approach; 4) to minimize the bias, the full texts of the articles were dually reviewed; 5) the quality of the included studies were rated independently by two reviewers (K.M and P.R); 6) studies’ characteristics and findings were comprehensively listed; 7) the publication bias and risk of other biases were listed; and 8) heterogeneity was also assessed.
Risk assessment
The risk of bias for each study was assessed. Any disagreement was resolved by the third author (N.Y). We assessed the risk of bias according to the following domains: random sequence generation; allocation concealment; blinding of participants and personnel; blinding of outcome assessment; incomplete outcome data; and selective outcome reporting. We judged each potential source of bias as high, low or unclear and provided a quote from the study report together with a justification for our judgment in the ‘Risk of bias’ table. Considering each of the domains listed, the risk of bias judgments was summarized across different studies. When considering treatment effects, we took into account the risk of bias for the studies that contributed to that outcome. Investigators or study sponsors were contacted to verify the key study characteristics and obtain the missing numerical outcome data where possible (e.g. when a study is identified as abstract only). In meta-analyses with indication of funnel plot asymmetry (p< 0.1), sensitivity analyses will be conducted. In any case, the risk of reporting bias will be discussed deeply.
Data synthesis
Dichotomous variables were reported as proportions and percentages, and continuous variables as mean values. Binary outcomes from individual studies were combined with both the Mantel-Hansel fixed-effect model and random-effect model. Overall, by using both models, the pooled diagnostic value of ultrasonography for assessing ulnar diameters and 95% Confidence Interval (CI) for this value were used. Cochran’s Q test was utilized to determine the statistical heterogeneity. This test was complemented with the I2 statistic, which quantifies the proportion of total variation across studies that is due to heterogeneity rather than chance. A value of I2 of 0–25% indicates insignificant heterogeneity, 26–50% low heterogeneity, 51–75% moderate heterogeneity and 76–100% high heterogeneity.
Publication bias was assessed by the rank correlation test and also confirmed by the funnel plot analysis. We planned to carry out the following sensitivity analyses, to evaluate whether key methodological factors or decisions affected the main result: 1) Only including studies with a low risk of bias; it should be noted that low risk was considered based on the status of four key domains including random sequence, allocation concealment, incomplete outcome data and selective reporting; 2) A sensitivity analysis will be performed after exclusion of the studies in which at least one member of the review team was affiliated; 3) A sensitivity analysis of using a fixed effects model; 4) A sensitivity analysis regarding the effect of the missing data; and 5) A sensitivity analysis only with studies in which all of the participants meet the inclusion criteria. In case post-hoc analysis was performed after the beginning of the review, the sensitivity analyses were marked with an asterisk and the reason it has been included post-protocol was explained. Reported values were two-tailed, and hypothesis testing results were considered statistically significant at p=0.05. Statistical analysis was performed using the Stata software (version 13.1, Stata Corp, College Station, TX, USA).
Search results
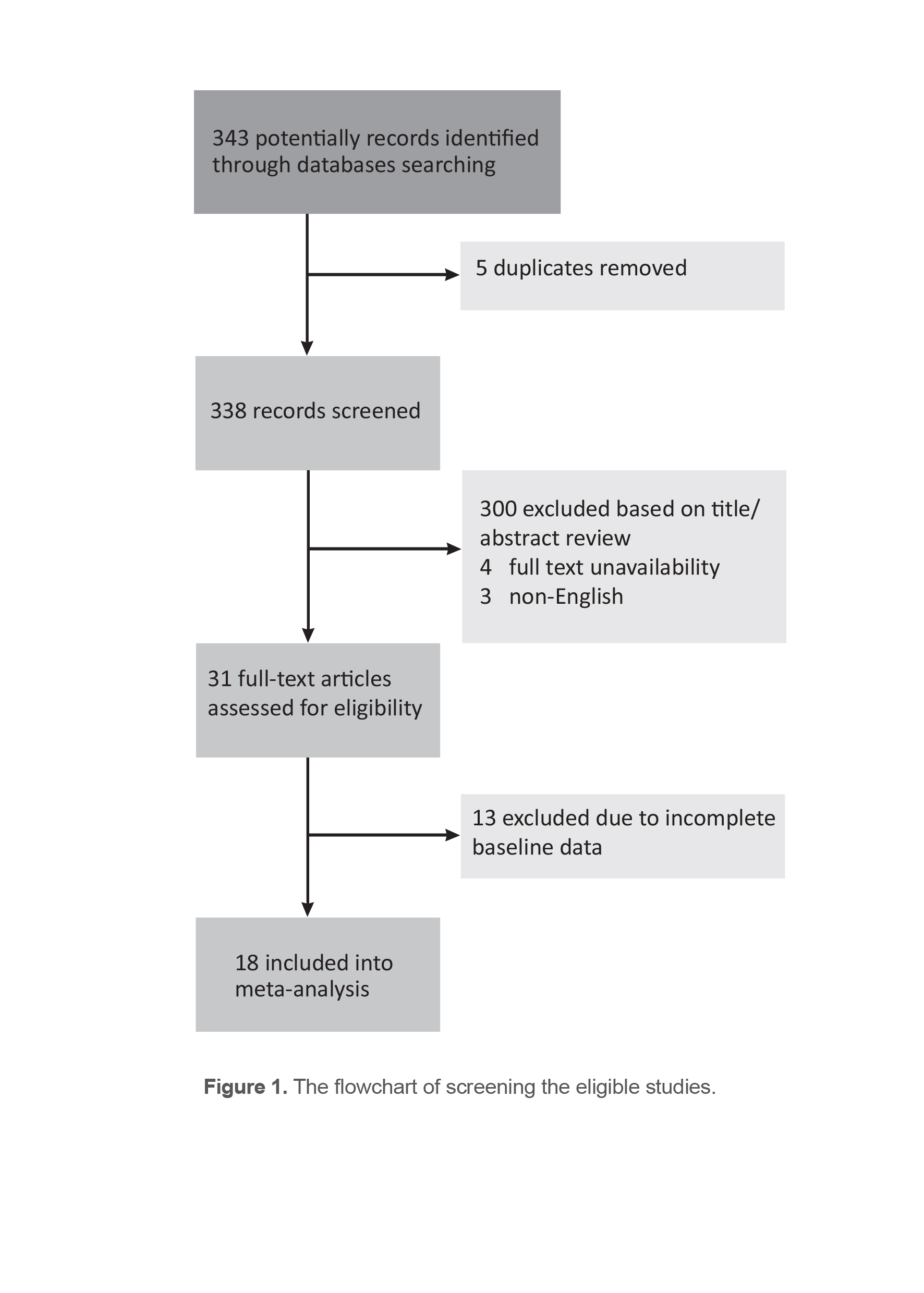
Of total 258 studies that were initially assessed based on the keywords, 31 articles, published from 2000 April to 2019 December, met the endpoints and only 18 ones were finally analyzed. The flowchart of screening the eligible studies has been depicted in Figure 1.
Results
Among the 343 initially retrieved articles, 307 were excluded after “Title” and “Abstract” reviewing in the first stage. In the second stage, 5 duplicate reports were excluded, and the remaining 31 full‐text articles were further reviewed. Agreement for selection of the studies was very good (k=0.9). Furthermore, 13 studies were excluded since their data were either incomplete or not associated with the main question of the review. Finally, 18 manuscripts were systematically reviewed with the goal of assessing Cross-Sectional Area (CSA) in different areas by various techniques of ultrasonography utilizing different types of transducer with the frequencies ranged 4 to 18 MHZ (9-26). Descriptive characteristics of the included studies are presented in table 1. Regarding the study types, five articles were done as cross-sectional study and 13 as case-control studies. In all studies, ultrasonography was applied to determine CSA, at least in one of the three areas of A) 2-4 cm proximal to the medial epicondyle (CSA-prox); B) 2-4 cm distal to the epicondyle (CSA-dist); and C) the maximum cross-sectional area (CSA-max) of the ulnar nerve. Considering the two aims of the study including the ranges of CSA determined at the three different levels and assessing the diagnostic value of ultrasonography to determine CSA, meta‐analysis was performed separately for each goal.
Systematically reviewing the CSA in different studies reached to the following ranges for this index: 1) CSA-prox ranged 5.5–18 mm2 for the ulnar neuropathy group versus 4-9.6 mm2 for the healthy control group; 2) CSA-dist ranged 5.0-9.8 mm2 for the ulnar neuropathy group versus 4-8.1 mm2 for the healthy group; and 3) CSA-max ranged 6.7-12.6 mm2 for the ulnar neuropathy group vs. 5.0-10.0 mm2 for the healthy group. With respect to the diagnostic value of US to determine ulnar neuropathy, the area under the ROC totally ranged between 0.73-0.79 for assessing CSA-prox, 0.62-0.76 for assessing CSA-dist and 0.75-0.90 for assessing CSA-max.
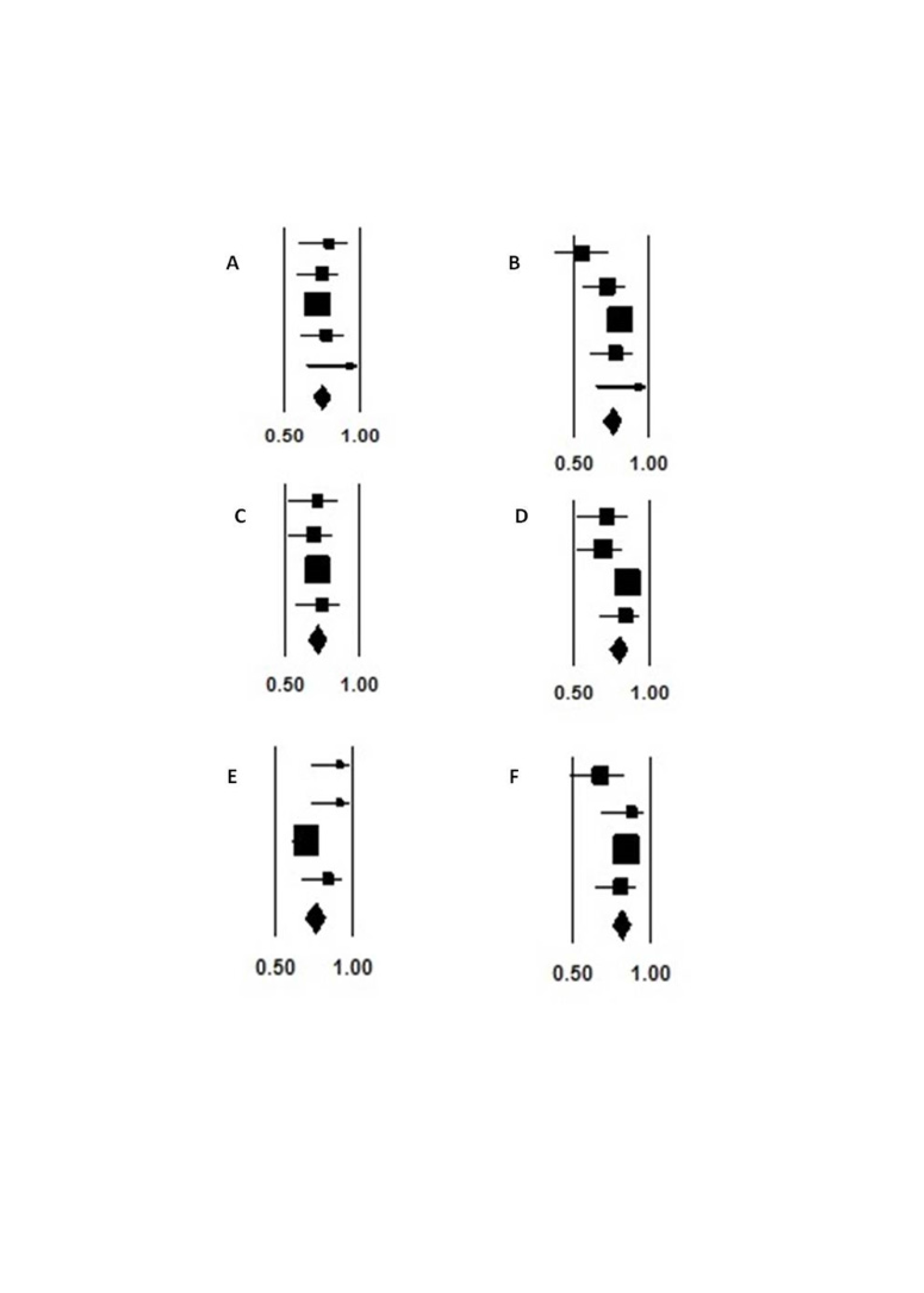
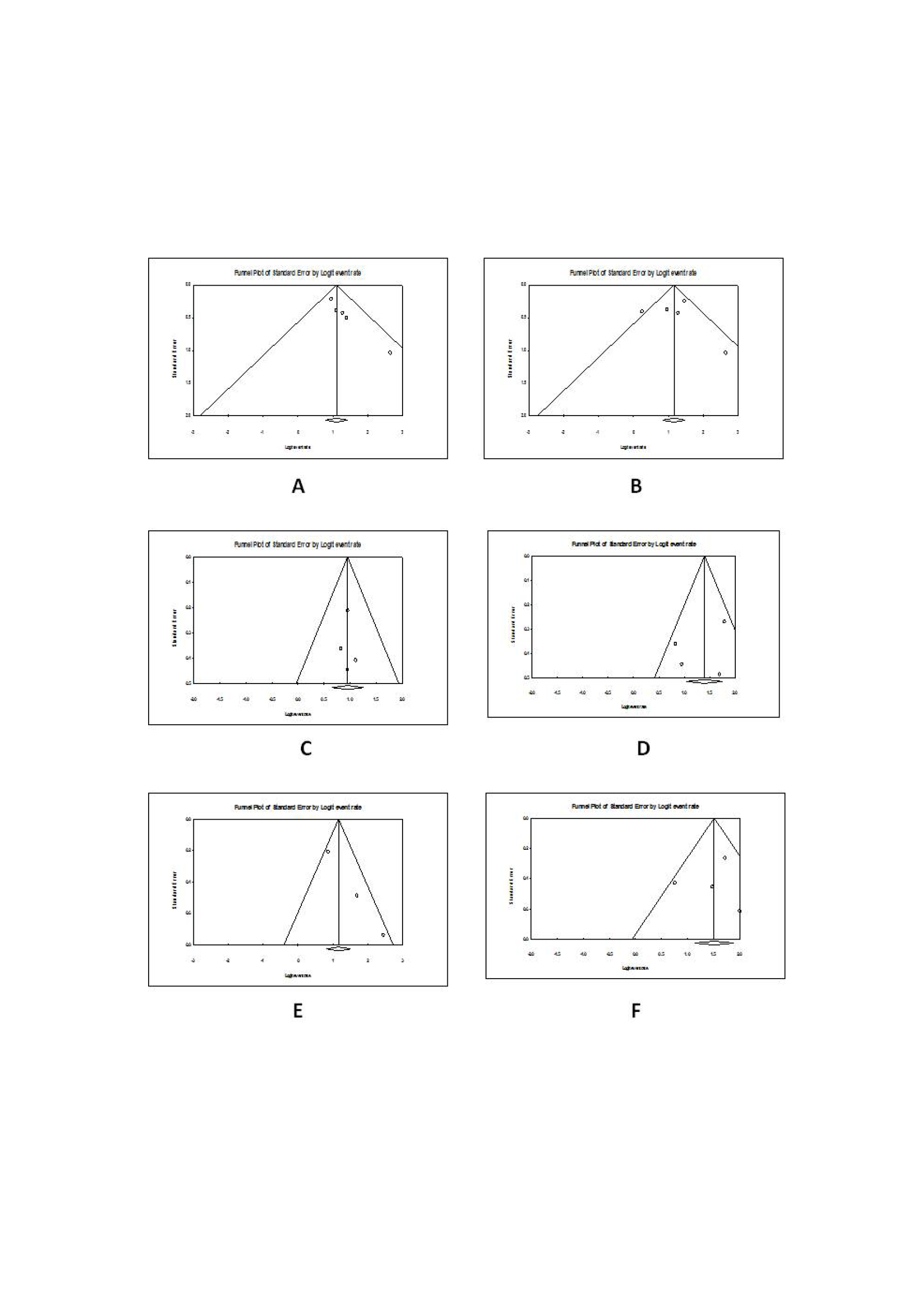
The pooled data on the diagnostic value of US: this device had a pooled sensitivity of 75.1 (95%CI: 68.8-80.5) and specificity of 76.1 (95%CI: 69.7-81.5) at the proximal level, sensitivity of 72.0 (95%CI: 65.5-77.8) and specificity of 80.1 (95%CI: 73.8-85.1) on distal level, and sensitivity of 76.1 (95%CI: 69.2-81.9) and specificity of 81.8 (95%CI: 75.6-86.7) on maximal CSA amount (Figure 2). No statistical heterogeneity was revealed among the studies to analyze sensitivity and specificity of the tool with I2 ranged 0.001-0.37.5. Publication bias was not found in any of the value assessments (Egger test, p values ranged 0.2-0.6) (Figure 3).
Discussion
In the current meta-analysis, the US usefulness was usefulness in the evaluation of suspected ulnar neuropathy by the accurate assessment of CSA at different levels of the elbow including proximal and distal to medial epicondyle, as well as the point with maximum CSA of the nerve. Although different brands of the device utilizing different frequencies had been employed, almost all studies agreed with acceptable sensitivity and specificity of this tool for assessing the likelihood of ulnar neuropathy via measurement of CSA. In this regard, the diagnostic value of US for predicting neuropathy was also comparable at different levels of the elbow (proximal or distal points). Such results led to the homogeneity of the results in the manuscripts.
Overall, the pooled sensitivity of 72.0-76.1% and the specificity of 76.1%-81.8% were achieved considering all types of CSA measurements. Also, according to the ROC curve analysis, US had a proper application for CSA assessment of the nerve with the aim of confirming or ruling out ulnar neuropathy. All to all, since EDX is a less available, expensive and somewhat painful procedure, ultrasonography (US) as an alternative or adjunct to EDX might be helpful in confirming entrapment, as well as the diagnosis of anomalous innervations. Moreover, through real-time high-resolution imaging, US can evaluate cubital zone anatomy and ulnar nerve condition in different positions (22).
As another main result, although good agreement was found across the different studies on the diagnostic value of US, the CSA measured by this device revealed a wide range. In other words, it seems that if the studies assessed the best cut-off values of CSA for discriminating ulnar neuropathy from healthy condition, a wide range of this cut-off point would be found; thus it seems that to determine an appropriate and valuable outpoint for CSA to predict ulnar neuropathy, we face a heterogeneous condition.
Study limitations
Overall, US seems to be a helpful device for diagnosing ulnar neuropathy. However, some questions have remained to be necessary for answering. First, ‘which sectional area of the nerve should be considered for evaluation with the most diagnostic accuracy?’ since different levels have been considered for this purpose in various studies. Second, ‘which cut-off point for the CSA at each level could be considered?’ Finally, ‘which type of transducer gives us the most accuracy in CSA evaluation?’ Additionally, ‘given the limited comparative studies on the diagnostic accuracy of different imaging tools, does US outperform other instruments and what are the potential limitations of this tool over other instruments?’ Therefore, despite confirming the diagnostic capability of US in this regard, further studies are still required to obtain the best diagnostic method. But overall, due to its availability, affordability, and non-invasiveness, US is the best known method to date.
Conclusion
In the current meta-analysis, it was proved that ultrasound could be a suitable device to diagnose ulnar neuropathy at elbow, with acceptable sensitivity and specificity values, especially via CSA measurement at the proximal level or the maximum amount.
Conflict of Interest
Authors have no financial or non-financial competing interests to disclose.
Funding
This study had no financial sponsor and authors did not receive any funds.