Document Type : Original article
Abstract
Background: To tackle the 2019 coronavirus infection (COVID-19) disease pandemic, effective antiviral therapy is critical. We assessed the efficacy of sofosbuvir and daclatasvir for treating patients with COVID-19.
Methods: This was a randomized controlled trial in adults with moderate-to-severe COVID-19 disease admitted to Razi Teaching Hospital in Ahvaz, Khuzestan Province, Iran. Patients were randomly assigned to the sofosbuvir and daclatasvir group (n=35, intervention group) and control group (n=35, standard care). The primary endpoint of this study was the length of hospital stay, clinical improvement, mechanical ventilation, mortality, and side effect.
Results: We found that the combination of Daclatasvir and Sofosbuvir (DCV+SOF) did not make a statistically significant difference in terms of mortality. There was no significant difference in the duration of hospitalization between the two groups. The two groups did not differ significantly in terms of the frequency of side effects. There were 2 cases of intubation and death in both groups.
Conclusion: The medications used in this study, i.e, the combination of daclatasvir and sofosbuvir, failed to show a significant effect in patients, and despite promising laboratory studies, there were no improvements observed in vital signs and the indicators studied, including clinical signs. Hospitalization days, ventilator requirements and mortality did not make a significant difference. To confirm the results of this study, conducting researches with a larger sample size are needed.
Keywords: Acute respiratory distress syndrome, Daclatasvir, Drug interventions, SARS-COV-2, Sofosbuvir
Introduction
The innovative disease of coronavirus (COVID-19), which started early in Wuhan, China, in December, 2019, has spread to most nations and has contributed to a disastrous impact on healthcare services around the country (1,2). On 19 February 2020, Qom city announced the first documented case of the infection in Iran and the disease has now been established in all regions of the country (3,4). Global interest has been generated by the high prevalence of COVID-19, and the World Health Organization (WHO), has described it as a globally concerned human medical crisis (2). COVID-19 progresses rapidly from human to human and as recorded in autopsy trials and laboratory experiments, is mainly acute viral pneumonia that contributes to respiratory failure (5). Fever, dry cough, dyspnea, weakness, sore throat, headache, moderate upper respiratory tract disease, viral pneumonia with respiratory distress, and even death are the typical clinical signs of the infection (6). Latest reports also have shown that it appears to have a broad variety of clinical characteristics in addition to the aforementioned effects, including asymptomatic, diarrhea, myalgia, discomfort, lack of taste and smell, etc. (7,8).
Regrettably, one after the other, treatment combinations believed to be successful have otherwise been proved. Different options are desperately needed, but they take time to grow (9). An urgent care potential is given by reusing existing pharmaceuticals. Present tests include Remdesivir, Hydroxychloroquine, Chloroquine, Favipiravir, Lopinavir/Ritonavir, and Nitazoxanide, although these medications have not proven effective in the treatment of COVID-19 patients, with the potential exception for Remdesivir (4,10). The addition of Azithromycin to the Lopinavir/Ritonavir plus hydroxychloroquine regimen did not show a significant difference in terms of mortality. But patients who received Azithromycin plus Hydroxychloroquine had a better general condition and accordingly this regimen seems to be appropriate for patients without cardiac arrhythmias (11). The results of a review revealed that the most common treatment of COVID-19 is Lopinavir/Ritonavir, Remdesivir, and convalescent plasma, respectively. However, some of these treatments are at the early stages of trial and need more investigation to confirm the efficacy and safety (12).
As a therapy for HCV, a former formulation of Sofosbuvir and Daclatasvir has proven to be effective. The mixture has since been added in 2015 to the Important Drugs List and has been made accessible in generic formulations worldwide (4). For the treatment of HCV in Iran, a generic fixed-dose mixture of sofosbuvir and daclatasvir (400/60 mg, respectively) is used and is thus a pragmatic candidate for the COVID-19 trial (10).
Similarities are observed between HCV replication pathways and the coronavirus, and sofosbuvir could be a possible alternative in the treatment of COVID-19 (13). Based on the minimal experimental data, it is speculated that sofosbuvir could be a potential alternative for improving the treatment of patients with COVID-19, mainly at the onset of the infection and prior to the virus invasion of the parenchymal lung cells (14,15). The safety and effectiveness of numerous antiviral medications, including Sofosbuvir, Sofosbuvir/Ledipasvir, Sofosbuvir plus Velpatasvir, Sofosbuvir plus Daclatasvir, Ribavirin, Lopinavir/Ritonavir, Favipiravir, Umifenovir, and Remdesivir, have been tested or measured for the treatment of COVID-19 in 17 randomized trials (13).
The safety and efficacy of sofosbuvir/daclatasvir/ribavirin arm in COVID-19 patients were tested in a single-center, randomized controlled trial with a target sample size of 72 patients. This randomized trial was too small to make definitive conclusions. There were trends in favor of the Sofosbuvir/Daclatasvir/Ribavirin arm for recovery and lower death rates. However, there was an imbalance in the baseline characteristics between the arms. Larger randomized trials should be conducted to investigate this treatment further (4).
The blockade of SARS-CoV-2 by Sofosbuvir in cell cultures has newly been documented (16). Sacramento et al found that Sofosbuvir blocked transcription of SARS-CoV-2 in cells originating from human hepatoma (Huh-2) and type II pneumocyte (Calu-3) with EC50 values of 6.2 and 9.5 μM, respectively (17). Another study proved that Sofosbuvir was capable of protecting human brain organoids from contamination with SARS-CoV-2 (18). As the disease is new, no clinically accepted medication is available.
Materials and Methods
Study design and participants
The present study is a double-blind randomized controlled clinical trial. In this study, patients with moderate to severe SARS-COVID-19 were admitted to Razi Teaching Hospital affiliated with Ahvaz Jundishapur University of Medical Sciences. Patients with acute fever (oral temperature 37.8 °C at least once before enrollment) and/or cough, shortness of breath, and gastrointestinal symptoms were suspected to have COVID-19. A positive qualitative RT-PCR for SARS-CoV-2 and/or features consistent with COVID-19 on a chest CT scan was conducted to prove COVID-19 infection. In the 18-80 years group, cases of confirmed COVID-19 were included. Just cases with moderate on-admission infection were identified as respiratory rate >30/min, arterial O2 saturation <93%, along with compatible chest CT scan findings.
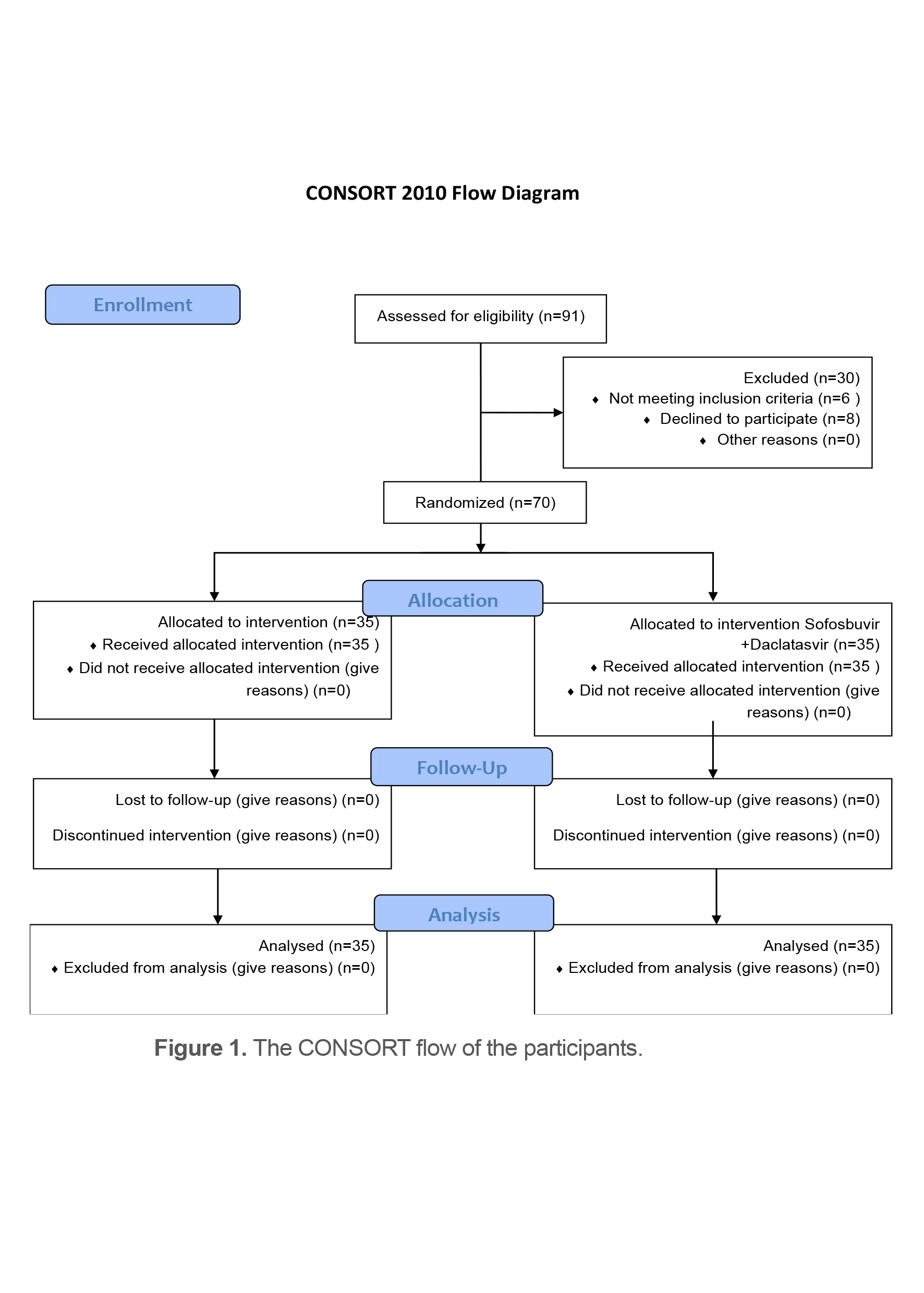
70 cases without multi-organ dysfunction, active cancer, renal failure (less than 50 mL/min/1.73 m2 of creatinine clearance), anemia (less than 9 g/dL of hemoglobin), pregnant, and patients treated with Amiodarone, Phenytoin, Phenobarbital, Rifabutin, or Carbamazepine were removed. Prior to research enrollment, all patients were expected to have written informed consent (Figure 1).
Inclusion criteria
Inclusion criteria including age over 18 years, hospitalization due to at least one of the characteristics of shortness of breath (increased respiratory rate more than 30/minute)/ oxygen saturation less than 93% or arterial oxygen to tail oxygen ratio less than 300 mgHg COVID-19 were confirmed by arterial blood gas analysis.
Exclusion criteria
Exclusion criteria consisted of known allergic reaction to the intervention drug, pregnancy or lactation, any previous interventions for COVID-19, heart rate less than 60 beats per minute, Amiodarone use, evidence of multiple organ failure, need for mechanical ventilation in screening, and Estimated Glomerular Filtration Rate (EGFR) less than 50 ml/minute.
After sampling and obtaining the written informed consent, patients were randomly divided into intervention and control groups using a block table. Randomization was done centrally by a stratified block randomization method. Patients were stratified by admission to sites. After the delegated person obtained the patients’ permission, an independent contact for allocation packets was done. Investigational medications and/or standard of care (national protocol) were dispensed by a pharmacist according to the randomization list. In the intervention group, patients received a Daclatasvir/Sofosbuvir 60.400 mg tablet (Knowledge Pharmaceutical Development Company) daily for 7 days, in addition to the treatment recommendations of the Corona National Committee. In the control group, patients received treatment recommendations from the Corona National Committee (in case of discharge, treatment was continued at home).
Procedure
Corona National Committee treatment recommendations included 200 mg Hydroxychloroquine or 250 mg Chloroquine phosphate tablets (equivalent to 150 mg baseline) 2 tablets every 12 hours on the first day and 1 tablet every 12 hours for at least 7 days depending on the patient’s clinical condition. At the physician’s discretion, one of the following drugs was added to the patient’s diet:
-Kaletra tablets (Lopinavir/Ritonavir) 200/50 every 12 hours 2 tablets for at least 7 days and at a maximum of 14 days.
-Atazanavir/Ritonavir 300/100 tablets one daily tablet with food for at least 7 days and at a maximum of 14 days.
The initial outcome of clinical improvement was defined within 14 days of the starting treatment and for this purpose, fever, respiration rate per minute, and oxygen saturation were measured daily. Criteria for clinical improvement included normalization of the temperature (37.2 °C), respiration rate (≤ 24 per minute), and oxygen saturation (>93% in room temperature) and were stable for up to 24 hours. Secondary consequences include the need for mechanical ventilation, imaging changes (day 14 or earlier as determined by the physician), and mortality.
The present study was a double-blind study evaluating the outcome of treatment and the statistician, and the patients were unaware of assigning individuals to groups, and many patients will be discharged by telephone and 2 weeks by CT scan. They are evaluated later.
Ethics approval
The study protocol was approved by the institutional review board and ethics committee of Jundishapur University of Medical Sciences (approval number: IR.AJUMS.REC.1399.300). This study is registered by IRCT.ir: IRCT20200816048422N1). The grant number is U-99091.
Statistical analysis
Quantitative variables were reported as mean (median) and standard deviation (mid-quarter range) and qualitative variables were reported as number (percentage). The normality of quantitative variables was evaluated using the Kolmogorov-Smirnov test. Chi-square test (or Fisher’s exact test) was used to examine the relationship between qualitative variables and an independent t-test or its non-parametric equivalent (Mann-Whitney test) was used for quantitative comparison between the two groups. The significance level of the above tests was considered less than 0.05. All statistical procedures were performed using SPSS software (version 26.0, SPSS Inc., Chicago, IL, USA). Graphs were drawn in Microsoft office, Excel, 2013 software.
Results
The age, sex, and baseline characteristics were generally similar between the two groups (Tables 1 and 2), since clinical improvement consists of general symptoms, Pulse Rate (PR), Respiratory Rate (RR), oxygen saturation (O2 sat), and body temperature (T). Initially, using the chi-square test, two daily differences of each clinical symptom were calculated and reported in the following tables. Finally, the total clinical symptoms of the participants per day were calculated. Then, the difference between the mean frequencies was calculated using the independent t-test. Based on the t-statistic (0.769) and significance level (0.448), no significant difference was observed in the clinical improvement in a total of 16 days of intervention (day 14+0+last day) in the clinical improvement. Therefore, the hypothesis is not accepted and no significant difference was observed between the groups in the clinical improvement.
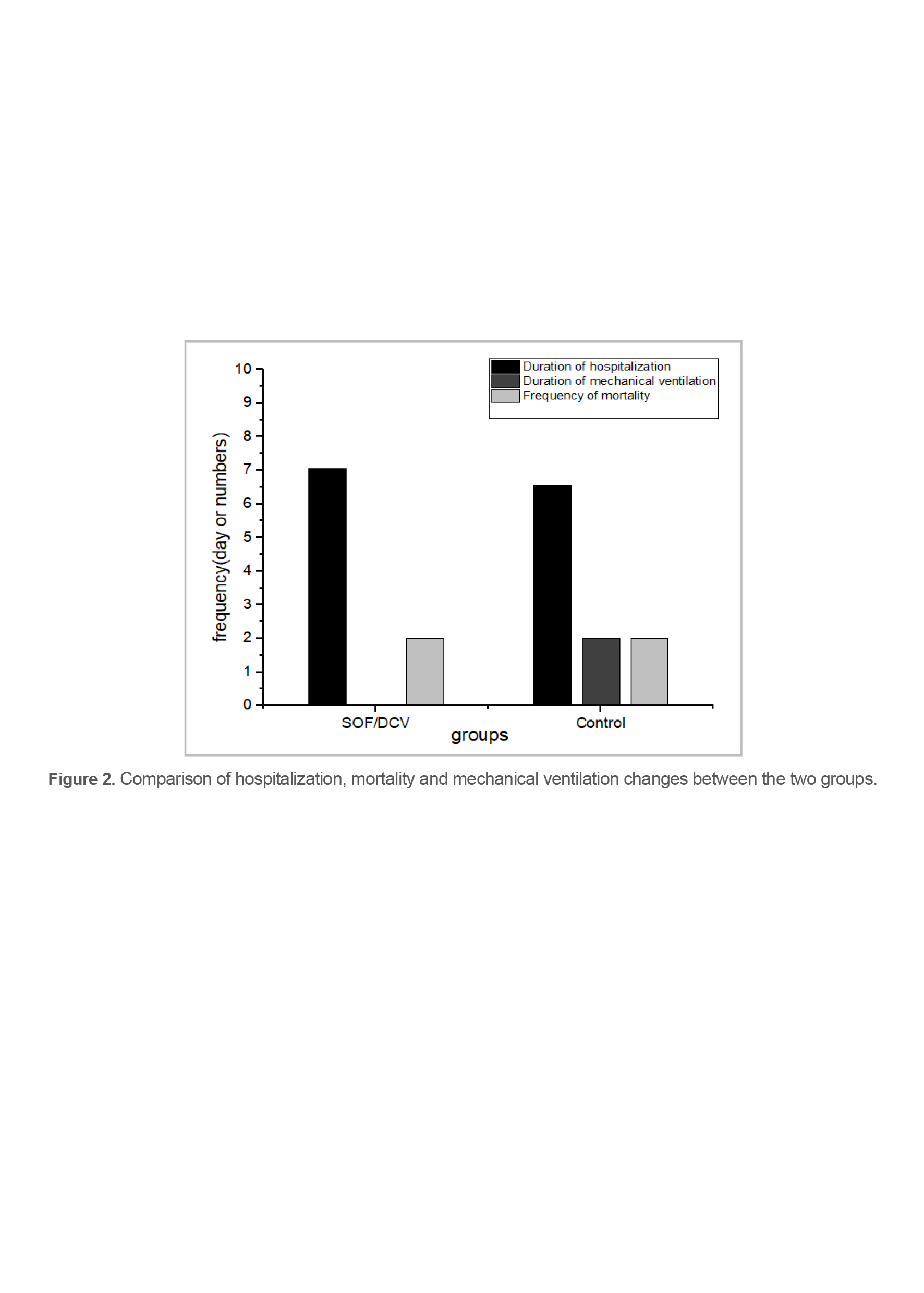
Based on the performed analyzes and the independent t-test (t=0.515) obtained from comparing the mean in the two groups during the hospitalization period, the level of significance is equal to 0.609, which is not statistically significant. Therefore, the two groups did not differ significantly in terms of length of the hospital stay. Hence, this hypothesis is not accepted (Figure 2). According to the analysis, the amount of Chi-square obtained from comparing the frequencies of the two groups during the days of mechanical ventilation is equal to 2.180, which is not statistically significant (p=0.336). Therefore, there is no significant difference in the two groups in terms of the duration of mechanical ventilation days. Thus, this hypothesis is not accepted (Figure 2).
The results regarding the use of mechanical ventilation also show that the amount of Chi-square obtained by comparing the frequencies of the two groups in the frequency of the use of mechanical ventilation is equal to 2.180, which is not statistically significant (p=0.336). Therefore, the two groups do not differ significantly considering the frequency of mechanical ventilation. Hence, this hypothesis is not accepted (Figure 2).
According to the analysis, the amount of Chi-square obtained by comparing the frequencies of the two groups frequency of mortality is equal to 0.003, which is not statistically significant (p=0.953). Therefore, there is no significant difference in the two groups in terms of mortality. Hence, this hypothesis is not accepted (Figure 2).
Based on the analyzes performed, the amount of Chi-square obtained from comparing the frequencies of the two groups in the indicators related to side effects is presented in the following tables. In general, considering the mean frequency of the drug group (98.5±52.41) and the mean frequency of the control group (96.5±56.37) which is equal to p=0.960, this rate is not statistically significant. Therefore, the two groups did not differ significantly in terms of the frequency of the side effects. Thus, this hypothesis is not accepted.
Table 1. Baseline characteristics of the patients
|
p-value |
Control (n=35) |
SOF/DCV (n=35) |
Variables |
|
0.966 |
52.38±15.09 |
52.54±14.07 |
Age(year) |
|
0.849 |
166.8±11.24 |
165.6±11.70 |
Height(cm) |
|
0.854 |
91.67±130.6 |
91.06±14.53 |
Weight(kg) |
|
0.964 |
33.52±5.74 |
33.46±5.90 |
BMI(Kg/m2) |
|
0.875 |
1.61±0.49 |
1.63±0.48 |
Type 2 diabetes |
|
0.954 |
1.94±0.23 |
1.94±0.23 |
Respiratory diseases |
|
0.168 |
2.00±0.01 |
1.94±0.23 |
Renal diseases |
|
0.070 |
1.91±0.28 |
2.00±0.01 |
Hepatic diseases |
|
0.070 |
1.91±0.28 |
2.00±0.01 |
Thyroid disease |
|
- |
- |
- |
Cancer disease |
|
0.337 |
2.00±0.01 |
2.00±0.01 |
Rheumatoid disease |
Daclatasvir (DCV); Sofosbuvir (SOF)
Table 2. Duration of the symptoms before hospitalization of the participants in the two groups of drug therapy and control group
|
Days |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
10 |
12 |
14 |
20 |
Sum |
|
|
Groups |
SOF/DCV |
1 |
2 |
5 |
9 |
1 |
10 |
0 |
5 |
0 |
2 |
0 |
35 |
|
Control |
1 |
2 |
5 |
1 |
3 |
10 |
1 |
6 |
2 |
2 |
2 |
35 |
|
|
Sum |
|
2 |
4 |
10 |
10 |
4 |
20 |
1 |
11 |
1 |
5 |
2 |
70 |
*First week of the symptoms = 40, Second week of the symptoms = 18 Third week of the symptoms = 2; Daclatasvir (DCV); Sofosbuvir (SOF)
Discussion
We found that the combination of DCV+SOF made no statistically significant difference in terms of mortality. There was no significant difference in the duration of hospitalization between the two groups. This finding was aligned with the previous studies (19-21). Although the combination of DCV+SOF may improve oxygen saturation and decreases the symptoms such as fever or generalized aches, it did not show significant survival benefits (22).
Infection with SARS-CoV-2 is a potential disease with such a high rate of spread that only the most well-structured health systems in high-income, advanced nations will overcome it successfully. Since medicines are the perfect solution to prevent infectious diseases such as COVID-19 from spreading, their production cycle has fundamental problems and protection control measures that take several months or years to accomplish their implementation (23).
Approximately two-thirds of the patients admitted to the study were men (65.71%), which is consistent with the previous studies showing that COVID-19 affects men more than women (4). A significant proportion of patients (57.14%) were symptomatic seven days or more prior to hospitalization.
In this case, Abbaspour et al “pointed out that trends are in favor of sofosbuvir, daclatasvir, and ribavirin for regeneration and lower mortality rates have occurred.” However, they showed that there was a “difference between the weapons in the study design.”To further evaluate this treatment, larger, randomized trials should be performed (4).
Eslami et al “reported that via successful healthcare signs, lower mortality rates, a shorter period of both ICU and hospital stays and fewer side effects, treatment of patients with extreme COVID-19 with sofosbuvir/daclatasvir was substantially more successful than ribavirin”. These early findings must be replicated in larger double-blind, randomized sofosbuvir/randomized trials. There is a global consensus on the treatment of COVID-19 infection by daclatasvir (9).
27.12% of the patients had hypertension, 37.14% had diabetes, 14.2% had cardiovascular disease and 18.5% had other chronic diseases. The client’s body mass index was 33.5 kg/m2 on average, which is in the obesity category. There was no statistically significant difference between the control and Daclatasvir+Sofosbuvir groups in terms of duration of pre-hospital symptoms, ethnicity, level of education, chronic diseases, and body mass.
Symptoms at the time of admission include 70% shortness of breath, 64.2% dry cough, 50% weakness and fatigue, 38% muscle pain, 48.57% fever and chills, 27.14% anorexia, 17.1% nausea, and 15.71% dizziness. Decreased sense of smell was reported in two patients, but disorders of the sense of taste were not observed in any patient. There was no statistical difference between the study groups in terms of clinical symptoms at admission. These findings are similar to those reported by the United States Centers for Disease Control (24).
Among the variables compared between the two groups, the vital signs in the drug treatment group did not show a significant difference compared to the control group. Both groups had tachypnea, tachycardia, and fever at the time of admission, and had decreased oxygen saturation levels without supplemental oxygen use. As the patients’ fever continued, the symptoms were monitored. By controlling the fever, the heart rate dropped to a more normal value, then the number of breaths dropped from normal, and finally, patients were able to maintain normal oxygen levels without relying on oxygen. The duration of hospitalization in the Daclatasvir+Sofosbuvir group was 7.05 days, and in the control group was 6.55, which did not show a statistically significant difference (p=0.609). One patient in the control group and one patient in the drug group needed mechanical ventilation.
Sadeghi et al reported that addition of sofosbuvir and daclatasvir to standard care substantially shortened the hospitalization length in comparison to standard treatment. While fewer deaths in the treatment arm were observed, this was not statistically substantial. It seems wise to perform larger-scale trials (25). The results of Sadeghi et al are consistent with the results of the present study.
The results of this study showed 2 deaths (5.7%) in each study group that indicated no difference between the two groups. Sovodak in this population did not require specific profitability and did not cause a difference between the two statistical groups in terms of mortality, length of hospital stays, improvement of vital signs, and the need for mechanical ventilation.Although the actual case fatality risk of SARS-CoV-2 is still unknown with modeling-based predictions that differ widely among experiments, it has been reported to be less extreme than other coronaviruses, such as SARS-CoV (9.6%) and MERS-CoV (34.5%) (7,24). However, the results of the present study may not be consistent with some studies. Given that the mortality ratio to the number of participants was very high, it may be due to the selection of samples at the time of the first wave of the corona in Iran being at its peak. Besides, it is reported that SARS-CoV-2 variants can challenge clinical treatments since they may have different mortality rates, transmissibility, and morbidity (26).
The most common symptoms in this population were shortness of breath, dry cough, weakness, fatigue, fever, and chills. Other significant symptoms such as anosmia or decreased sense of taste, were not significantly more common in this population.
Limitations
The present study has some limitations. First of all, the sample size was on a medium scale. Second, the costs of Sofosbuvir/Daclatasvir are expensive and it may be unaffordable to utilize all parts of the world. Thirdly, Sofosbuvir/Daclatasvir is a rare medication and is not available easily. Finally, we failed to determine the variants of coronavirus that were included in our study.
Conclusion
The drug used in this study such as the combination of daclatasvir and sofosbuvir, did not show a significant effect in patients, and despite promising laboratory studies, it could not be considered in the treatment regimen of patients with COVID-19. The drug did not make a significant difference in the improvement of vital signs, nor in the improvement of any of the studied indicators, including clinical symptoms, hospitalization days, the need for a ventilator, and the mortality rate. The findings of the current study are in contrast to the findings of Sadeghi et al which stated that “the use of daclatasvir and sofosbuvir reduced the length of hospital stay in COVID-19 patients (6 days in the pharmacotherapy group vs. 8 days in the control group, p=0.029).
Acknowledgements
This study was partly supported by Razi Teaching Hospital in Ahvaz. The present study was taken from Dr. Zahra Fakhraei’s dissertation and all its rights belong to Jundishapur University. (Approval ethics number: IR.AJUMS.REC.1399.300, Grant number: U-99091). Iranian Registry of Clinical Trials No: IRCT20200816048422N1.
Conflict of Interest
There is no conflict of interest to declare.
Funding
This research was funded by Jundishapur University of Medical Sciences.