Document Type : Original article
Abstract
Background: Although the effect of Erythropoietin (EPO) in neonatal and animal model of hypoxic ischemic encephalopathy has been previously reported, its effect on comatose patients in adult human has yet to be investigated.
Methods: This study was designed to find the effect of intravenous administration of EPO on the recovery from coma in the adult patients with Cardiac Arrest (CA)-induced hypoxic ischemic encephalopathy. This randomized controlled trial study was performed on 60 CA patients who survived Cardiopulmonary Resuscitation (CPR) from April 2011 to Nov 2020. The patients were randomly divided into two equal groups including the control, received normal saline, and the EPO groups, and demographic data were recorded. The EEG and Glasgow Coma Scale (GCS) were recorded on hours 6, 12, 24, and 48 post-success CPR and interpreted by an expert neurologist. Magnetic Resonance Imaging (MRI) was done at 24 and 72 hr of post-CPR and interpreted by an expert radiologist. All patients were checked twice daily by an expert cardiologist.
Results: 60 patients were included in this study. There was no significant difference between two groups in terms of demographic data. There was also no significant difference between two groups in terms of GCS and EEG at all post-CPR interval times. No significant difference was observed between both groups with respect to the frequency of pre-existing and metabolic acid-base disorders.
Conclusion: The intravenous administration of EPO has no effect on the recovery from coma in the adult patients with CA-induced hypoxic ischemic encephalopathy.
Keywords: Consciousness, Encephalopathy, Erythropoietin, Hypoxia, Ischemia
Introduction
Cardiac Arrest (CA) is one of the major causes of mortality and long-term neurologic disorders. Despite recent heath care and resuscitation advances, its outcomes remain poor, with 10% of patients surviving until hospital discharge of which 5% experiencing complete neurologic recovery (1). Hypoxic ischemic brain injury or encephalopathy occurs as a consequence of CA that leads to mortality and long-term neurologic disability ranging from mild cognitive deficits to minimal conscious and Persistent Vegetative States (PVS) in survivors (2,3). Several neuroactive agents such as erythropoietin alone in combination with hypothermia have been introduced to protect or restore brain damage resulted from hypoxic-ischemic encephalopathy in neonatal infant. This is due to biological properties and their safety in sick infants (4). Neonatal animal studies have shown that immediate and delayed treatment of hypoxic ischemic brain with erythropoietin can be neuroprotective and/or neurorestorative (5,6). The prevalence of PVS or coma among survivors after CA represents a heavy burden on patients, their families, and health care personnel (7). Although the effect of erythropoietin in neonatal and animal model of hypoxic ischemic encephalopathy has been previously reported, its effect on PVS in adult human has yet to be investigated. Therefore, this study was designed to find the effect of intravenous administration of Erythropoietin (EPO) on the recovery from coma in the adult patients with CA-induced hypoxic ischemic encephalopathy. Moreover, mean erythropoietin dose was selected based on a review by Oorschot et al (4).
Materials and Methods
This randomized double blind controlled trial study was performed on 60 CA patients who had successful Cardiopulmonary Resuscitation (CPR) from April 2011 to Nov 2020. The Ethics Committee and the authors’ institutional review board of Shahrekord University of Medical Sciences approved the study (IR.SKUMS.REC.1387.685). The author group collected written informed consent from all the patients’ families. The patients with 30-70 years of age and Glasgow Coma Scale (GCS) <7 were included in this study and randomly divided into two equal groups including the control (received normal saline), and the erythropoietin groups. The exclusion criteria were time since CPR> 24 hr, cardiac arrest out of hospital, the history of advanced cancer, chronic disease, as well as the history of advanced cardiac, pulmonary and renal diseases. All patients were cared and treated under the same protocol, and CPR and their neurologic states were conspired for one month.
Erythropoietin injection
During the one-hour post-success CPR, the initial dose of erythropoietin infusion was started as 200 IU/kg/5 min with accurate control of vital signs (cardiac and pulmonary monitoring) and then continued with 20 IU/kg/hr of erythropoietin infusion for 24 hr. The standard glucose, potassium solution containing insulin was used for better penetration of erythropoietin into brain. All patients received mechanical ventilation as following: Synchronized Intermittent Mandatory Ventilation (SIMV), Positive End Expiratory Pressure (PEEP): 3 cmH2O, Respiratory Rate (RR): 8/min, Tidal Volume (TV):6 cc/kg, and fraction of inspired oxygen (FiO2:100%, was reduced to 40% for 48 hr).
The vial signs of patients were checked continuously through EKG monitoring, pulse oximetry, capnography, and I/O control. The patients were maintained at normothermia, normotensive, and normocapnia to mild hypocapnia. The GCS of each patient was checked by an anesthesiologist.
All patients received a baseline Arterial Blood Gas (ABG), and their acid-base disorders were improved. Baseline EKG, CBC, FBS, BUN, Cr, hepatic and cardiac enzymes, albumin, and chest X-ray (CXR) were recorded for each patient as the same manner. The patients were maintained under normoglycemia and prevented from hemodilution, hemoconcentration, dehydration and fluid overload. The EEG were recorded on hours 6, 12, 24, and 48 post-success CPR and interpreted by an expert neurologist. At first 72h post-CPR, the patients were closely monitored. Magnetic Resonance Imaging (MRI) was done at 24 and 72 hr of post-CPR and interpreted by an expert radiologist. All patients were checked twice daily by an expert cardiologist. Cardiologist, radiologist and neurologist were the same for all patients. Patients were also monitored closely for erythropoietin side effects such as hypertension, seizures, stroke and thromboembolic complications.
Statistical analysis
All data were analyzed using SPSS software version 22. All data were expressed as mean±standard deviation. The mean of scale variables was compared between groups using independent t tests. Some of the variables were presented in a descriptive manner. A value of p <0.05 was considered statistically significant.
Results
Demographic data were presented in table 1. There were no significant differences between the two groups with respect to demographic data (p>0.05) (Table 1). All cardiac arrests took place in Coronary Care Unit (CCU), Emergency Room (ER) and Intensive Care Unit (ICU). Leading cause of cardiac arrest was acute myocardial infarction followed by trauma and intracranial hemorrhage. Out of the treatment and control groups, 8 (26.6%) and 6 (20%) cases were female and 22 (73.4%) and 24 (80.0%) were male, respectively. There was no significant difference between two groups in terms of sex. The mean GCS of the patients at six interval times of post-CPR in both groups were presented in table 2.
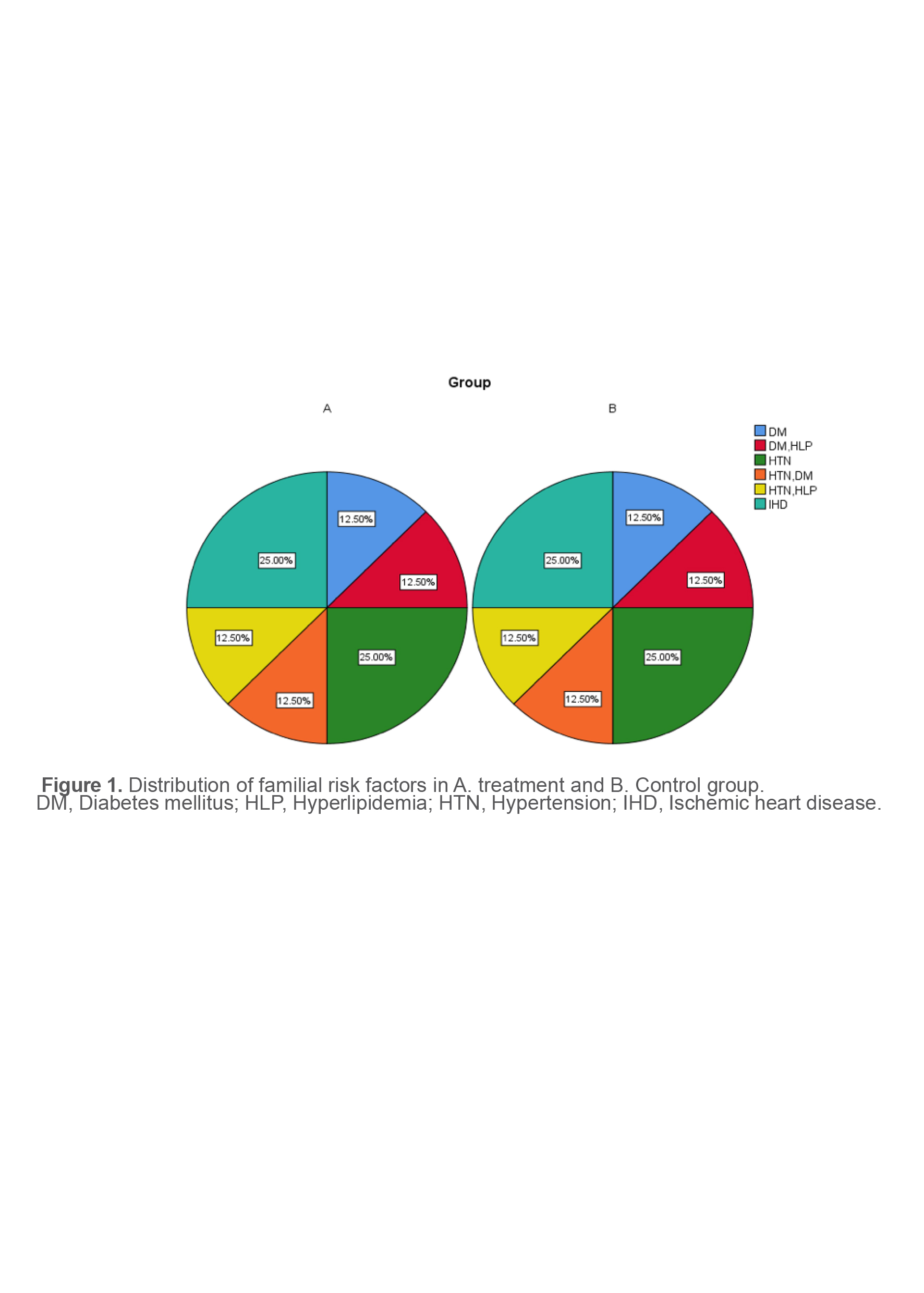
There was no significant difference between the two groups in terms of GCS at all post-CPR interval times (Table 2). There was no significant difference between the treatment and the control groups in terms of risk factors including Diabetes Mellitus (DM), Hypertension (HTN), DM+HTN, Hyperlipoproteinemia (HLP), DM+HLP, HTN+HLP, and Ischemic Heart Disease (IHD) (Figure 1).
There was no significant difference between the treatment and the control groups in terms of corneal reflex [(3(10%) vs. 0(0%)] and pupillary light reflex (8/30:26.6% vs. 9/30:30%), respectively. No significant difference was observed between the treatment (27 asystol and 3 VF cases) and the control (24 asystol and 6 VF cases) groups in terms of primary EKG. The obtained data from EEG in both groups at 6-, 24-, 48-, and 72-hour post-CPR were presented in table 3.
The frequencies of mixed metabolic acidosis+ respiratory acidosis, pure metabolic acidosis, and metabolic acidosis+respiratory alkalosis in the treatment and control groups were 50% (15 cases) vs 40% (12 cases) and 50% (15 cases) vs 60% (18 cases), respectively. There was no significant difference between the treatment and control groups with respect to the frequencies of mixed metabolic acidosis, respiratory alkalosis and pure metabolic acidosis. EEG abnormalities were almost the same between the two groups during the 72-hour follow-up.The mean age of treatment and control groups were 52.56±8.14 and 53.4±7.08 years, respectively. There was no significant difference between treatment and control groups with respect to mean age (p>0.05). The patients were classified in 3 age groups; 30 to 40, 41 to 50, and 51 to 60 years old (Table 4). There was no significant difference between both groups in terms of age classification (p>0.05). Intra-group analysis showed a significant difference amongst the patients considering age classification (p<0.001). Thus, the most frequent age class belonged to age group 3 or 51-60 years old in both groups.
Table 1. Demographic data of both groups
|
Variable/group |
Treatment |
Control |
p-value |
|
Weight (kg) |
75.76±13.80 |
76.73±11.97 |
0.773 |
|
Height (cm) |
167.43±8.22 |
167.63±7.14 |
0.920 |
|
CPR time (min) |
13.23±2.95 |
12.96±2.53 |
0.709 |
|
PR (/min) |
108.66±16.07 |
110.73±15.68 |
0.616 |
|
BP (mmHg) |
141±28.96 |
146.67±38.93 |
0.358 |
|
RR (/min) |
27.9±3.91 |
29.10±2.68 |
0.587 |
|
T (°C) |
36.7±0.87 |
36.40±1.08 |
0.171 |
CPR, Cardiopulmonary resuscitation; BP, Blood pressure; RR, Respiratory rate; T, Temperature
Table 2. The Glasgow Coma Scale at six interval times of post-CPR
|
Time/group |
Treatment |
Control |
p-value |
|
1 hr post-CPR (mean+SD) |
4.3±1.36 |
4.60±1.37 |
0.401 |
|
6 hr post-CPR |
4.2±1.34 |
4.5±1.38 |
0.399 |
|
12 hr post-CPR |
4.5±1.04 |
4.3±1.36 |
0.527 |
|
24 hr post-CPR |
4.2±1.86 |
4.1±2.04 |
0.896 |
|
48 hr post-CPR |
3.5±2.37 |
4.1±2.6 |
0.358 |
|
72 hr post-CPR |
4.57±1.8 |
5.04±1.92 |
0.404 |
CPR, Cardiopulmonary resuscitation
Table 3. Results of EEG in both groups at 6-, 24-, 48-, and 72-hour post-CPR
|
Time/groups |
Treatment |
Control |
p-value |
|
6 hr post-CPR |
Major abnormality (27 cases) Moderate abnormality (3) |
Major abnormality (26 cases) Moderate abnormality (4) |
0.601 |
|
12 hr post-CPR |
Major abnormality (27 cases) Moderate abnormality (3) |
Major abnormality (26 cases) Moderate abnormality (4) |
0.601 |
|
24 hr post-CPR |
Major abnormality (27 cases) Moderate abnormality (3) |
Major abnormality (26 cases) Moderate abnormality (4) |
0.601 |
|
48 hr post-CPR |
Major abnormality (27 cases) Moderate abnormality (3) |
Major abnormality (26 cases) Moderate abnormality (4) |
0.601 |
|
72 hr post-CPR |
Major abnormality (27 cases) Moderate abnormality (3) |
Major abnormality (26 cases) Moderate abnormality (4) |
0.601 |
Table 4. Age classification and frequency of each age class in both groups
|
Age classification/ group |
Treatment |
Control |
p-value |
|
30-40 years |
5 cases (8.3%) |
3 cases (5%) |
0.6 |
|
41-50 years |
3 cases (5.0%) |
4cases (6.7%) |
0.34 |
|
51-60 years |
22 cases (36.7%) |
23 cases (38.3%) |
0.74 |
|
Total |
50 cases (50%) |
50 cases (50%) |
0.965 |
Discussion
The primary aim of this study was to find the effect of intravenous administration of EPO on the recovery from coma in the adult patients with CA-induced hypoxic ischemic encephalopathy and correlate relationship between gender and age, risk factors, and demographical data as well as EEG and GCS at five post-CPR interval times (hours 6, 12, 24, 48, and 72). The usefulness of the GCS for outcome prediction in survivors of treated CA were proven.
The GCS monitoring has been shown to be a simple and reliable approach for clinical outcome assessment in the treated CA patients at hospital arrivals after return of spontaneous circulation as well as before induction of therapeutic hypothermia (8,9). We found that the administration of EPO results in no improvement in GCS at hours 6, 12, 24, 48, and 72 hr post-CPR compared to the un-treated group. The frequency of dead patients was 30% (9/30) and 23.3% (7/30) in the treatment and control group.
There was no significant difference between the treatment and control group regarding survival rate as one of the clinical outcomes. This finding is in accordance with previous study that has reported the relationship between GCS score and clinical outcomes (8,9). The administration of EPO to protect or restore brain damage resulted from hypoxic-ischemic encephalopathy in neonatal infant has been illustrated in numerous studies (4). CA induces the cessation of brain blood flow, which can lead to ischemia and brain injury. How to prevent hypoxic-ischemic encephalopathy-induced brain injury following CA remains a question that needs to be answered (9). Multiple protective effects of EPO, such as neuroprotective effects and antiapoptotic, antioxidant, angiogenic against ischemia have been shown in cell culture and animal models (10). Erythropoietin administration has been shown to protect retinal neurons from acute ischemia-reperfusion injury (11).
The obtained data from demographical data showed that there was no significant difference between both groups in terms of age, sex, BP, RR, PR, and CPR time. The patients were classified in 3 age groups and the average age-specific incidence rate for CA was 51-60 years old. There was no significant difference between patients with or without treatment in terms of age. Age has been previously reported to early prediction and risk stratification of a poor outcome in comatose survivors following out-of-hospital CA (12). We have also found that there is no significant difference between both groups considering the corneal and pupillary reflexes that are other early predictors of the poor outcome in comatose survivors following out-of-hospital CA (12).
The obtained data from the frequencies of mixed metabolic acidosis + respiratory acidosis, pure metabolic acidosis, and metabolic acidosis + respiratory alkalosis showed no significant difference between the treatment and control groups with respect to frequencies of metabolic acid-base disorders that are common clinical problems in ICU patients (13).
In the present study, there was no significant difference between both groups in terms of pre-existing medical conditions such as DM, HLP, HTN, and IHD alone or in combination with each other. Although diabetes/high blood sugar, HTN, IHD, and HLP risk factor have been remained significant predictors of functional outcomes and neurocognitive functioning following traumatic brain injury (14,15,16), no relationship was found between the diabetic and non-diabetic patients with and without EPO with respect to clinical outcome.
Conclusion
In conclusion, the intravenous administration of EPO has no effect on the recovery from coma in the adult patients with CA-induced hypoxic ischemic encephalopathy. In addition, there was no significant difference in terms of the pre-existing medical conditions such as DM, HLP, HTN, and IHD as well as the frequency of metabolic acid-base disorders between both groups.
Conflict of Interest
The authors declare no conflict of interest in this study.
Acknowledgements
The authors wish to thank the Research Center of Sharekourd University of Medical Sciences, Iran.