Document Type : Original article
Abstract
Background: To find different variables involved in the hospitalization of patients referred to the respiratory Emergency Room (ER) at the time of COVID-19 pandemic.
Methods: A questionnaire was designed to determine different hypothetical factors involved in the hospitalization of 3481 patients during the COVID-19 pandemic.
Results: This study suggests that the following factors/variables are involved in the hospitalization of patients: age, respiratory distress, duration of symptoms, cough, 5-day-prolonged fever, diabetes mellitus, respiratory diseases, renal conditions, history of chemotherapy, saturation of blood oxygen, sore throat, and fever.
Conclusion: We found that through having an insight towards what may and may not be involved in the severity of the novel coronavirus infection, one might be able to decide if a patient could potentially benefit from hospitalization.
Introduction
In December 2019, a new/novel subspecies of the Coronaviridae family was discovered in Wuhan, China. Despite all the efforts, unfortunately, the aforementioned virus was spread throughout the world, and caused a pandemic unlike no other from the past (1). At first, as one would expect, China was struggling with the situation at hand; hospitals were filled, streets were abandoned, businesses collapsed, and, subsequently, the economy crashed (2). People were panicking as to what the fate of the country would be and where they would end up if this disaster continued for longer than expected. The whole world was wondering, first, what this virus is and how it got spread throughout China and, second, how to prevent it from getting into their nations. Leaders decided that the best way to protect themselves and their people is to close down the borders so strictly that their pupils would be as protected as one could be (3). Despite all the efforts and hard work put into this procedure, almost all countries got influenced and/or infected with the virus. Just like China, hospitals were filled, streets were abandoned, businesses collapsed, and, subsequently, economies crashed. Regarding the emergency of the situation, health-care centers and ministries acted rapidly to prevent it from getting worse and to manage the already affected matters and infected individuals. In Iran, specific hotline was devised so people did not have to attend hospitals and medical facilities in person to receive proper care since most cases were either not related to COVID-19 or did not need anything more than proper care and rest at home. Besides, their attendance might have influenced their lives or the lives of others. For the individuals who did attend the hospital inevitably, a series of steps were designed as to what the caregiver should do and how to do it and, as expected, how to gather proper information to help the patient at hand and in the future. One of the biggest and most referred-to hospitals in the country is Imam Khomeini Hospital Complex (IKHC) under the supervision of Tehran University of Medical Sciences. IKHC-TUMS is the largest hospital in Iran with more than 1300 active beds, located in Tehran, Iran. With over 900,000 patients that are receiving outpatient and inpatient services annually, IKHC plays a critical role in the national health care system. During the outbreak of COVID-19 in Iran, a large number of patients suspected of having the infection referred to this center.
During infectious disease outbreaks (e.g., coronavirus disease or COVID-19), it is particularly important to separate the patients likely to be infected with the pathogen from the beginning of entering the triage.
Triage can be effective if:
1) it prevents the transmission of infection to other patients.
2) health-care workers are aware of the use of appropriate personal protection during services to the patients.
3) timely appropriate diagnostic and treatment services are provided to infected patients.
In order to maximize efficiency, we defined an initial triage in which patients were divided into 3 groups:
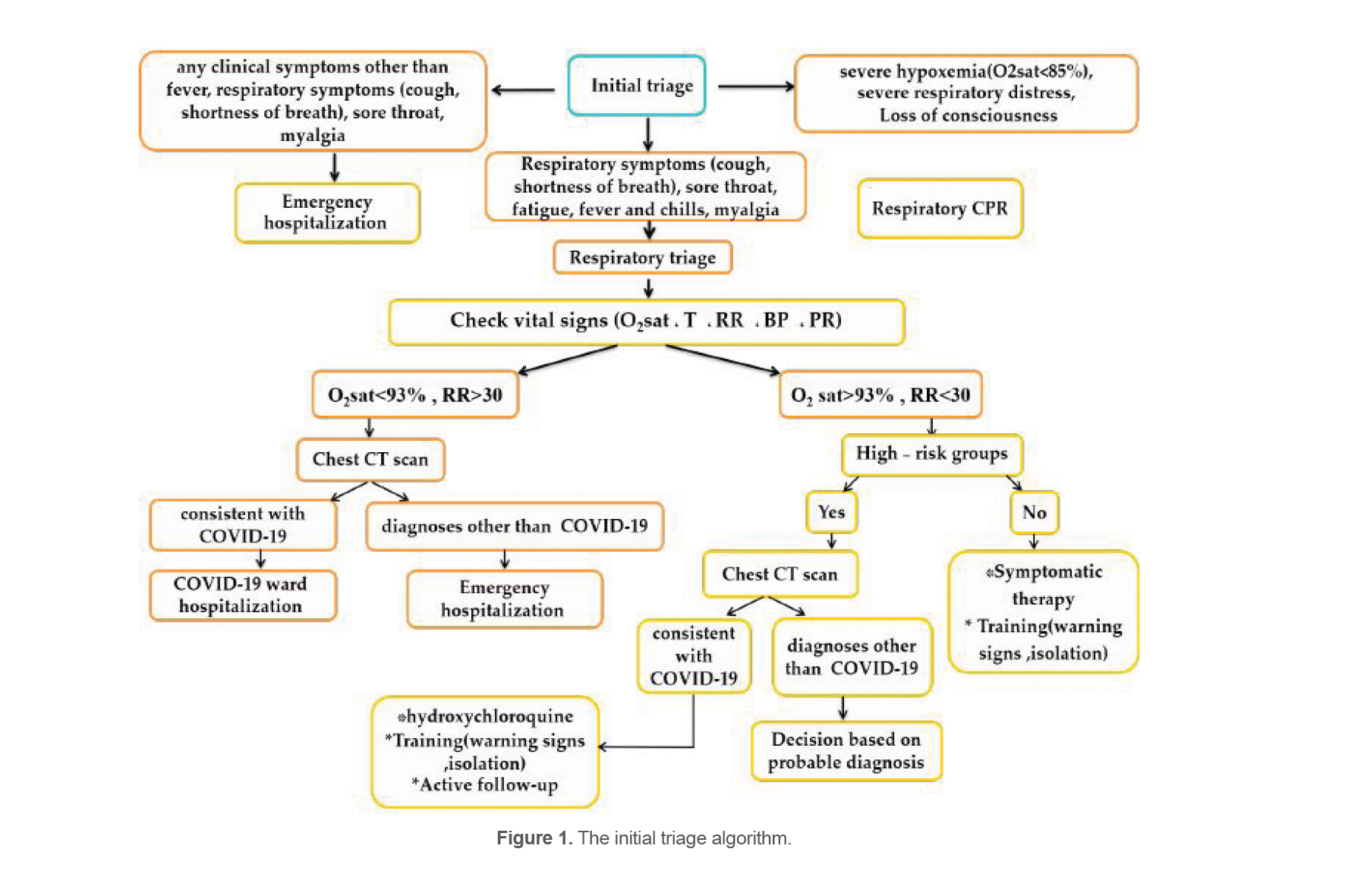
1. Patients needed urgent medical treatment (severe respiratory distress, severe hypoxia (O2sat<85%), and loss of consciousness) were referred to respiratory CPR. (In respiratory CPR, critical patients were visited without delay under the supervision of an emergency medicine faculty)
2. Patients who were suspected to have new coronavirus signs (cough, shortness of breath, sore throat, fatigue, fever, chills, and myalgia) were referred to respiratory triage.
3. Other patients (with other symptoms) were referred to the general emergency.
Respiratory triage has been separated from the general emergency department for the reduction of exposure. Patients were visited by infectious specialists in the respiratory triage. They were first examined for blood pressure, saturation of blood oxygen, temporal temperature, pulse rate, respiratory rate, height, weight, and body mass index. Then, they were asked about their current symptoms and present illness along with the medications they were consuming at the time and past medical history that may or may not have been associated with their current symptoms. Next, they were managed based on the history and the examination and according to the national protocol (Figure 1). Long and time-consuming as this process may have been for both caregiver and the patient, it was necessary to be more aware of the situation and to know what factors were involved in the hospitalization of the patients referred to respiratory triage of the aforementioned hospital at the time of COVID-19 pandemic, or any hospital for that matter.
There are some gaps in our findings. First, there is not enough data available yet for this disease. Different variants are not fully understood regarding their signs and symptoms (4). Also, it should be noted that due to the lack of control groups, studies cited in this paper might have biases (5).
Materials and Methods
By the consultation of the best practitioners in the country, an algorithm was created for any patients referred to respiratory Emergency Room (ER), and a survey was devised to determine how many variables (if any) are involved in the hospitalization of the 3481 patients referred to IKHC for respiratory conditions.
An initial triage was done to determine the severity of symptoms of each patient: patients with severe hypoxia (O2 sat<85%), severe respiratory distress, and loss of consciousness would be referred to respiratory CPR. Patients with respiratory symptoms (cough, shortness of breath), sore throat, fatigue, fever and chills, myalgia would go through the respiratory triage to decide the outcome of their treatment (Figure 1). Patients with any clinical symptoms other than respiratory symptoms would be admitted to the emergency ward as they were not relevant to respiratory ER.
As for any research, this one had to go under meticulous ethical considerations. From the initial extract of the input system, the name and personal data of the patients were removed prior to any further statistical analyses on the aforementioned data.
The aforementioned variables for the possible outcomes of the treatment are sectioned into three different groups: demographics, current symptoms, and co-existing conditions and complications. For demographics, we had: age, sex, pulse rate, temporal temperature, height, weight, Body Mass Index (BMI), systolic blood pressure, diastolic blood pressure, and saturation of blood oxygen (SpO2). For current symptoms, respiratory distress, duration of the symptoms, fever, chills, cough, sputum, chest pain, myalgia, joint pain, lethargy, perspiration, sore throat, dry throat, headache, runny nose, hoarseness, anosmia, loss of taste, epistaxis, epiphora, loss of appetite, nausea or vomiting, diarrhea, abdominal pain and severe abdominal pain, bloody stool, dysuria, otalgia, skin problems, unconsciousness, drowsiness, 5-day-long fever, and insomnia were considered. Last but not least, for co-existing conditions, diabetes mellitus, hypertension, heart conditions, respiratory diseases, renal conditions, liver conditions, hyperthyroidism, history of chemotherapy, cancer, pregnancy, and being medical staff were bared in mind. Also, certain drugs were considered as possible factors in the research such as methotrexate, steroids, other immunosuppressive drugs, hydroxychloroquine, lopinavir/ritonavir, azithromycin, and oseltamivir. Then, each variable was analyzed through the means of SPSS analysis, and the ones with the p-value equal to or less than 0.05 were included in the final analysis. The variables that entered the final model were considered to be effective in the results. These variables have shown to be effective in the final results of admission: either hospitalized or discharged (Ethics code: IR.TUMS.IKHC.REC.1399.481).
Results
There was a total of 61 variables, potential for being associated with the outcome of this study (Table 1), 25 of which entered the final analysis with the p-value of less than 0.10 (Table 2) in which the ones with the p-value equal to or less than 0.05 were considered to be effective or somehow involved in the hospitalization of the patients described in the introduction.
Table 1. Initial variables accounted for in the triage
|
Variable |
OR (95% of CI) |
p-value |
|
Sex |
|
|
|
Female |
0.83 (0.35-1.93) |
0.67 |
|
Male |
1.22 (0.90-1.66) |
0.18 |
|
Age* (Years old) |
|
|
|
0-25 |
Referent |
Referent |
|
26-40 |
1.37 |
0.43 |
|
41-65 |
2.99 |
0.006 |
|
66 and above |
8.56 |
<0.001 |
|
Saturation of blood O2* |
0.03 (0.02-0.50) |
<0.001 |
|
Pulse rate* (BPM) |
|
|
|
0-59 |
Referent |
Referent |
|
60-99 |
0.34 (.07-1.52) |
0.16 |
|
100 and above |
0.72 (0.16-3.17) |
0.67 |
|
BMI (kg/m2) |
|
|
|
0-19.9 |
Referent |
Referent |
|
20-24.9 |
0.82 |
0.58 |
|
25-29.9 |
0.62 |
0.02 |
|
30 and above |
0.60 |
0.008 |
|
Temperature |
1.42 (1.13-1.78) |
0.002 |
|
Height* |
0.97 (0.95-0.98) |
<0.001 |
|
Weight |
0.99 (0.98-1.00) |
0.73 |
|
Systolic BP |
0.99 (0.99-1.00) |
0.60 |
|
Diastolic BP |
0.99 (0.98-1.00) |
0.16 |
|
Respiratory distress* |
5.46 (3.87-7.69) |
<0.001 |
|
Duration* (Days) |
|
|
|
<5 days |
Referent |
Referent |
|
5-10 |
1.70 (1.20-2.43) |
0.003 |
|
11-30 |
0.96 (0.60-1.53) |
0.87 |
|
>30 |
0.83 (0.39-1.76) |
0.63 |
|
Fever* |
2.58 (1.90-3.49) |
<0.001 |
|
Chills* |
2.26 (1.67-3.06) |
<0.001 |
|
Cough* |
1.87 (1.37-2.55) |
<0.001 |
|
Sputum* |
1.74 (1.16-2.61) |
0.006 |
|
Dyspnea* |
2.88 (2.12-3.92) |
<0.001 |
|
Chest pain* |
1.58 (1.13-2.20) |
0.007 |
|
Body pain |
1.28 (0.94-1.75) |
0.11 |
|
Myalgia* |
1.49 (1.06-2.07) |
0.01 |
|
Lethargy* |
1.58 (1.15-2.19) |
0.005 |
|
Sore throat* |
0.62 (0.40-0.98) |
0.04 |
|
Headache |
1.03 (0.71-1.50) |
0.84 |
|
Anosmia |
0.87 (0.52-1.45) |
0.59 |
|
Loss of taste |
1.07 (0.61-1.87) |
0.81 |
|
Loss of appetite* |
2.97 (2.14-4.12) |
<0.001 |
|
Nausea or vomiting* |
2.55 (1.83-3.55) |
<0.001 |
|
Diarrhea |
1.34 (0.90-2.00) |
0.14 |
|
Drowsiness* |
2.66 (1.30-5.43) |
0.007 |
|
5-day-proloned fever* |
3.10 (2.29-4.19) |
<0.001 |
|
Diabetes mellitus* |
3.49 (2.39-5.10) |
<0.001 |
|
Hypertension* |
2.89 (2.02-4.14) |
<0.001 |
|
Heart conditions* |
3.44 (1.87-6.33) |
<0.001 |
|
Respiratory diseases* |
2.55 (1.54-4.22) |
<0.001 |
|
Renal conditions* |
6.25 (2.24-17.41) |
<0.001 |
|
Liver conditions |
3.68 (0.42-31.68) |
0.23 |
|
History of chemotherapy* |
5.65 (2.24-14.26) |
<0.001 |
|
History of cancer* |
3.21 (1.42-7.27) |
0.005 |
|
Methotrexate * |
18.63 (3.73-92.97) |
<0.001 |
|
Steroids |
2.04 (0.25-16.21) |
0.49 |
|
Other immunosuppressants |
1.78 (0.70-4.52) |
0.22 |
|
Hydroxychloroquine |
1.18 (0.79-1.79) |
0.40 |
* p<0.05
Table 2. Final model of variables involved in hospitalization
|
Variables |
OR (95% of CI) |
p-value |
|
Age* (Years old) |
|
|
|
0-25 |
Referent |
referent |
|
26-40 |
1.61 (0.64-4.07) |
0.30 |
|
41-65 |
1.96 (0.78-4.95) |
0.15 |
|
66 and above |
4.27 (1.53-11.96) |
0.006 |
|
Pulse rate (BPM) |
|
|
|
0-59 |
Referent |
Referent |
|
60-99 |
0.39 (0.05-2.60) |
0.33 |
|
100 and above |
0.79 (0.11-5.26) |
0.80 |
|
BMI (kg/m2) |
|
|
|
0-19.9 |
Referent |
Referent |
|
20-24.9 |
0.58 (0.24-1.37) |
0.21 |
|
25-29.9 |
0.55 (0.23-1.31) |
0.18 |
|
30 and above |
0.60 0.25-1.45) |
0.26 |
|
Respiratory distress* |
3.17 (2.02-4.98) |
<0.001 |
|
Duration* (Days) |
|
|
|
<5 |
Referent |
Referent |
|
6-10 |
0.99 (0.61-1.62) |
0.99 |
|
11-30 |
0.36 (0.18-0.72) |
0.004 |
|
31 and more |
0.70 (0.27-1.84) |
0.48 |
|
Chills |
1.36 (0.84-2.21) |
0.21 |
|
Cough* |
1.72 (1.11-2.69) |
0.01 |
|
Sputum |
0.86 (0.48-1.55) |
0.63 |
|
Chest pain |
1.42 (0.89-2.27) |
0.13 |
|
Lethargy |
0.88 (0.54-1.42) |
0.60 |
|
Sore throat* |
0.42 (0.23-0.79) |
0.007 |
|
Loss of appetite |
1.24 (0.74-2.07) |
0.39 |
|
Nausea or vomiting |
1.38 (0.84-2.27) |
0.20 |
|
Drowsiness |
0.97 (0.29-3.15) |
0.96 |
|
Fever for 5 days or more* |
2.13 (1.33-3.41) |
0.002 |
|
Diabetes Mellitus* |
1.90 (1.08-3.35) |
0.02 |
|
Hypertension |
1.70 (0.98-2.96) |
0.05 |
|
Heart conditions |
1.46 (0.56-3.82) |
0.43 |
|
Respiratory diseases* |
2.09 (1.08-4.07) |
0.02 |
|
Renal conditions* |
5.37 (1.40-20.58) |
0.01 |
|
History of chemotherapy* |
13.47 (3.02-59.98) |
0.001 |
|
History of cancer |
0.70 (0.14-3.60) |
0.67 |
|
Saturation of blood O2* |
0.04 (0.02-0.07) |
<0.001 |
|
Fever* |
1.67 (1.04-2.69) |
0.03 |
* p<0.05
Discussion
COVID-19 has different modes of transmission although what seems to be the case in the respiratory pathway is the most effective way to infect the host (6). Despite it cannot be determined who has COVID-19 and who does not just by looking at them, certain predictors might be beneficial in foreseeing the severity of the ones who actually get infected (7-10).
Diabetes, advanced age, and many other comorbidities are known to be associated with COVID-19 (7). Blood oxygen levels, heart rate variability, and age have shown to be relatively solid indicators of COVID-19 severity (8-10). Although CT scan does not fully predict the infection of COVID-19 (11), we used CT scan in some of the patients and PCR in others to ensure the presence of the infection and allocate beds to them.
As demonstrated in table 2, a saturation of blood oxygen levels with a grouping based on 93 played a role in the objective. Also, we entered age to the final model as follows: less than 25 years old, 26-40, 41-65, and older. Contrary to our belief, the duration of symptoms had a role in the hospitalization with a p-value of less than 0.01. The grouping for duration is less than 5, 6-10, 11-30, and 31 days or more. Symptoms like cough, sore throat, 5-day-prolonged fever, and fever, in general, were involved in the objective although no relationship was found between the objective and chills, sputum production, and chest pain. In addition, comorbidities like diabetes mellitus, respiratory diseases, renal conditions, and history of chemotherapy had a role in the hospitalization.
As expected, blood oxygen levels were related to pulmonary involvement. Patients presented with hypoxia had significant chest CT involvement (8). The current study shows a similar correlation between the saturation of blood oxygen and the severity of the disease. If the saturation of blood oxygen falls below 93%, there is a high probability that the patient would need hospitalization (p<0.001).
As proven before, heart rate and heart rate variability are associated with a COVID-19 positive infection (9,12), however, due to our findings, pulse rate is not related to hospitalization although in cardiovascular problems, heart rate variability is a predictor of hospitalization (13).
Age strongly suggests different presentations and prognoses (10,14). As an example, sore throat is more than 3 times different in people below 60 and 60 years old or older (11.8 vs. 3.5%). As for the prognosis, need to a longer respiratory treatment and a poorer response to the mentioned treatment were observed in patients with 60 years or older age (14). In our study as well, we found that there is a high probability (p=0.006) that patients older than 65 years that referred with COVID-19 symptoms would be hospitalized.
Increased BMI has been shown to be highly suggestive of poor health and also a poor outcome of probable diseases (15). High BMI is strongly suggestive of poor outcomes in Diabetes Mellitus (DM) type 2. Insulin dependence, cardiovascular, cerebrovascular, renal, lower extremities, and ocular complications in patients with DM-2 are more observed in the groups with higher BMIs (16). Even for metabolically healthy individuals, high BMI is a risk factor for cardiovascular diseases (17). Also, BMI is strongly related to COVID-19 test positivity. Currently, the UK government suggests people with BMI>40 adhere to non-pharmaceutical and lifestyle adjustments to prevent the spread of COVID-19, social distancing to name one (18). However, our study found no connection between BMI and the hospitalization of these patients. The relationship between severity of COVID-19 and BMI was not clear in our study since their relationship is relatively likely to be random compared to other variables (p=0.261).
A reliable approach to the diagnosis of COVID-19 is a chest CT scan. A study showed that the longer we wait after the patients show symptoms, the more involvement (e.g., ground-glass view) we might see in the imaging. In the mentioned study, the group with the longest duration (6-12 days) of symptoms was associated with more significant CT involvement (19). In our study, the group whose symptoms had started 11-30 days before their visit had the most chance of hospitalization (p=0.004).
Cough is associated with a high chance of COVID-19 positive PCR (20). It is one of the most common symptoms of COVID-19. However, actions needed to deal with acute and chronic cough due to COVID-19 are not yet clear, as a result, current guidelines for acute and chronic cough due to other reasons are used (21). A meta-analysis found that out of 24,410 confirmed COVID-19 patients, 57% of them had cough as a symptom (22). The present study also suggests a similar finding: cough is correlated with hospitalization of patients (p=0.015). Patients referred to the special clinic with a cough had a higher chance of being hospitalized than the patients who did not.
Sore throat, however self-reported, is not rare amongst patients with a positive PCR. 17.4% of patients had a sore throat. It is also found that sore throat is even more common with the new UK variant of the virus (23). Our study found that it could be related to hospitalization (p=0.007), however, since this symptom is self-reported, it is not a reliable and adequate indicator of COVID-19 for hospitalization and should be considered among other factors and variables presented in this article.
One of the most common symptoms of COVID-19 is fever. Although it is self-limited if properly treated with fluids. For patients with a temperature of fewer than 38.5 degrees, allowing the body to use the high temperature to fight the infection would be the best decision (24). However, a study shows that prolonged fever (9-11 days) is associated with hypoxia compared to the control group (25). In the setting of our study, we found that prolonged fever (p=0.002) as well as having fever in general (p=0.033) is associated with a higher chance of hospitalization. The more days a patient has a fever, the higher the chance of that patient being hospitalized.
In April 2020, due to the lack of information regarding Diabetes Mellitus (DM) and its relationship with COVID-19, the general suggestion was to be cautious of hypoglycemic conditions (7). In August 2020, more thorough research emerged which showed that not only the incidence is higher among patients with DM, but also the severity of the disease is more catastrophic (26). The current study, as well, showed that there is a high chance (p=0.026) that if the patient is diabetic, of any sort, they will be hospitalized because of COVID-19. In addition, patients with any kind of renal dysfunction/disease are more prone to hospitalization (p=0.014) than those with no background of renal diseases.
Another study conducted in 2020 represented that chemotherapy is not associated with the severity of COVID-19 while malignancies are (27), to our surprise, in our patients with specific demographics of the region, history of chemotherapy is related to hospitalization (p=0.001), but cancers are not definite predictors of our favorable outcome (p=0.679).
Conclusion
Although more thorough research with more precise measures of determining the possible outcome might help future researchers, perhaps it is safe to assume that this research of over 3400 referrals and the analytical data extracted would make a killer argument for anyone deciding on whether or not to hospitalize a patient infected with COVID-19.
Limitations
A big hurdle in conducting this research was the fact that the country was in the surge of COVID-19 and a large number of referrals attended the hospital despite a shortage of staff. Therefore, the focus was naturally and ethically to care for the patients in need of it and the time to collect and record the data was limited.
Acknowledgements
The authors thank the staff of the hospital for their help.
Conflict of Interest
There is no conflict of interest.