Document Type : Original article
Abstract
Background: Cyclic Vomiting Syndrome (CVS) is an idiopathic, complex, multifactorial disorder that is often characterized by recurrent episodes of vomiting and is usually separated by asymptomatic episodes. Prophylaxis should be considered in children with frequent or severe periods. Prevention and treatment of CVS in children is very difficult and no specific and effective treatment has been proven in clinical trials. Propranolol is approved for the prophylaxis of CVS in children of all ages, but its effectiveness has been variable. In this study, we investigated the efficacy and safety of adding L-Carnitine to propranolol therapy in the prevention of pediatric CVS.
Methods: 76 children who were diagnosed with CVS were included in this study. They were divided into two equal groups. The first group received high dose of Propranolol and the case group received L-Carnitine with low dose of propranolol for 6 months.
Results: CVS attacks’ frequency in both groups of treatment with propranolol alone and in combination with L-Carnitine and propranolol, before and after the treatment was significantly reduced. But there is no significant difference between the two groups 70.6%) vs. 90.9%) (p-value=0.062). There was no significant reduction in the duration days between vomiting attack index in both groups (31.6 % vs.43.2%) (p-value= 0.345).
Conclusion: Our research revealed that combination of low dose
propranolol with L-Carnitine has comparable efficacy with high dose
Propranolol in prophylaxis of CVS.
Keywords: Children, Cyclic vomiting syndrome, L-carnitine, Propranolol
Introduction
Cyclic Vomiting Syndrome (CVS) is an idiopathic, complex, multi-factorial disorder of the brain-intestinal axis. Contributing mechanisms include genetic predispositions, physiological abnormalities involving mitochondrial function, autonomic regulation, or neuroendocrine function. It is often characterized by recurrent episodes of vomiting and is usually separated by asymptomatic episodes (1).
The prevalence of CVS in children is approximately 1 to 2%, and it affects all ages from infancy to adulthood, most frequently in school-aged children. 46% of symptoms start at age 3 or earlier but the diagnosis can be delayed by average age of 4 years (2).
Indications for preventive medication in case of recurrent CVS attacks (more than every 1-2 months) and its severity (more than 2 days or need to be hospitalized) consist of impaired quality of life (e.g, frequent absences from school), unsuccessful treatment of acute attack or occurrence of side effects (3).
The cause and pathogenesis of CVS are still unknown. It seems that various factors can influence the development of vomiting in CVS, and several hypotheses including migraine, mitochondrial diseases including mitochondrial fatty acid oxidation disorders; gastrointestinal motility disorder, corticotropin releasing factor in response to stress, brain and intestinal axis disorders, autonomic dysfunction, abdominal epilepsy, ion channel dysfunction, and psychodynamic changes have been suggested as possible causes (1,4).
Tri cyclic antidepressants, beta-blockers such as propranolol, anticonvulsants, Sumatriptan, Erythromycin, L-Carnitine, coenzyme Q10, and Cyproheptadine have been shown to be effective (1-9). Recent consensus recommendations include Cyproheptadine as a first-line agent in children with 5 years of age and younger, and Amitriptyline as a first-line agent in children with 5 years of age and older. Propranolol is a second-line prophylactic medication in all childhood ages (5). The usual dose of Propranolol for the prevention of CVS is 0.25 to 1 mg/kg/day (4). Side effects of Propranolol include hypoglycemia or related seizure, negative effects on heart function such as bradycardia, hypotension, prolonged atrioventricular conduction or intensification of atrioventricular block and bronchospasm/bronchial hyper-reactivity. Other common, non-serious events related to Propranolol are sleep disturbances, diarrhea, constipation, and cold extremities. Consensus recommendations for pre-screening for propranolol treatment consist of cardiovascular screening and identification of patients at risk for heart block, arrhythmia, or pulmonary abnormalities/airway reaction diseases. It is important to note that vomiting and fasting increase the risk of hypoglycemia, especially in children (6).
The functional role of mitochondrial dysfunction has not yet been fully elucidated, but more recently the role of mitochondrial dysfunction in the pathophysiology of CVS has been considered (1-3). L-Carnitine is a dietary supplement that is frequently used in the treatment of mitochondrial dysfunction. The compound L-Carnitine is a long-chain fatty acid across the inner membrane of the mitochondria and is therefore required for lipid oxidation. In addition, L-Carnitine plays a “detoxifying” role in disrupting the accumulated mediators of metabolism from dysfunctional mitochondria (10).
Due to the lack of studies on L-Carnitine in this field and the lack of definitive treatment in CVS patients, we decided to compare the effect of combination therapy with low dose Propranolol and L-Carnitine with conventional dose of Propranolol in the prophylactic treatment of CVS in children and adolescents.
Materials and Methods
This study was a single-blind randomized controlled trial carried out on children with CVS. Prior to the study, informed consent was obtained from the children’s parents. They were referred to a gastroenterology clinic of the Imam Hussein Children’s Hospital (Isfahan, Iran) in 2020. The diagnosis of CVS was done by academic pediatric gastroenterologist. The sample size was obtained 38 for each group. In 76 children and adolescents (3–18 years old) the diagnosis of CVS was confirmed according to Rome IV Criteria (12-11) (Table 1). Exclusion criteria were comprised of the presence of asthma, diabetes mellitus, cardiovascular diseases, and drug hypersensitivity, gastrointestinal, neurological or inherited metabolic diseases.
Table 1. Rome IV diagnostic criteria for CVS
|
Must include all of the following: |
|
Two or more periods of intense, unremitting nausea and paroxysmal vomiting, lasting hours to days within a 6-month period |
|
Episodes are stereotypical in each patient |
|
Episodes are separated by weeks to months |
|
After appropriate medical evaluation, the symptoms cannot be attributed to another condition |
The baseline testes performed on all patients included: complete blood count, liver function tests, creatinine, blood urea nitrogen, electrolytes, lipid profile, glucose, amylase, lipase, and ammoniac and urine analysis. Neurologic examination and upper gastrointestinal series were done for rule out of neurologic or anatomic abnormalities.
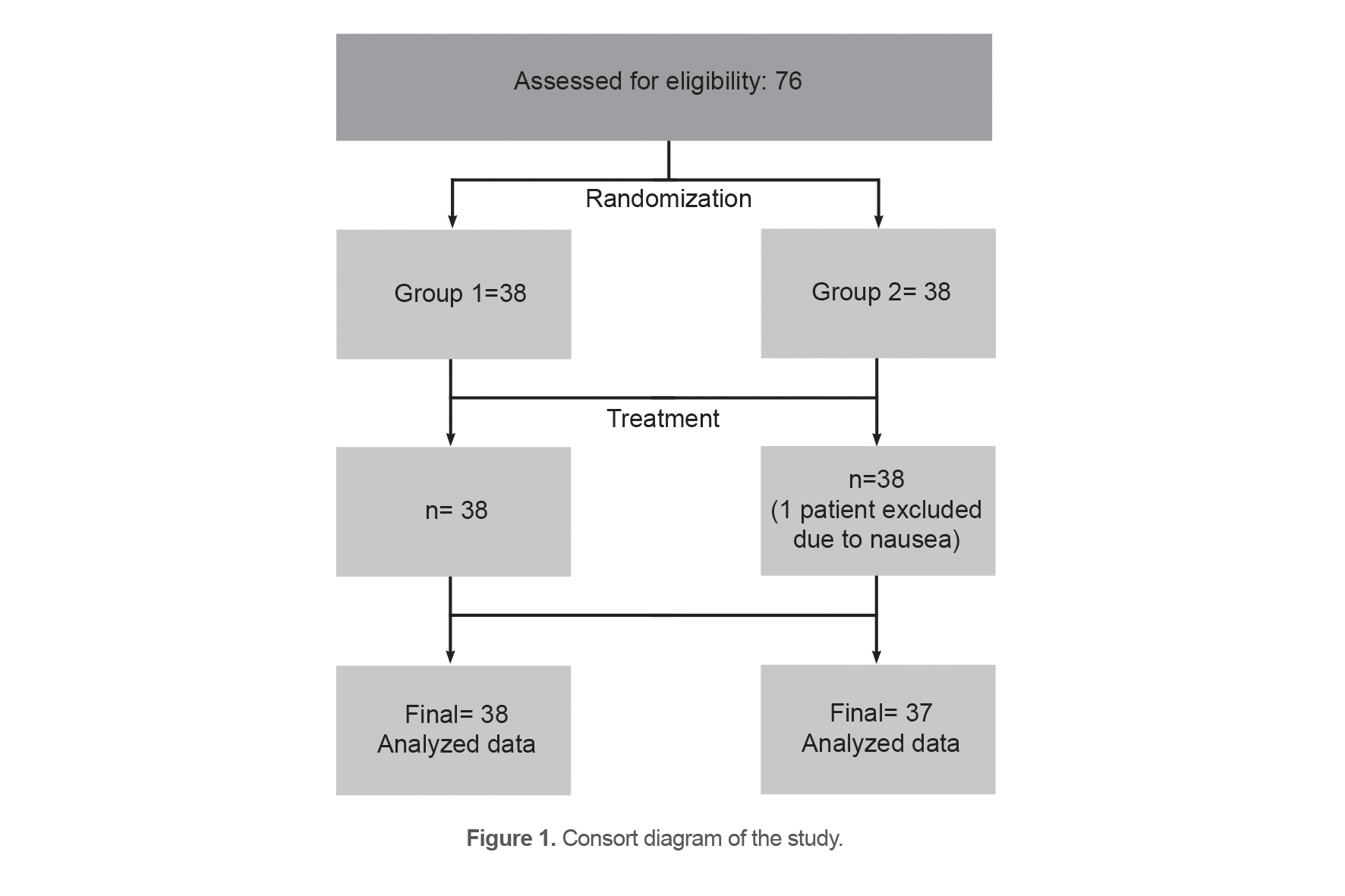
Children illegible for studies were randomly divided into two equal groups (38 patients in the first and 38 in the second group). Convenience sampling method and random allocation were used for selecting the patients in two treatment groups (Figure 1). The first group received Propranolol tablet (Rouz Darou company in Iran) at the initial dose of 1 mg/kg (body weight) per day, if there is no proper response, the dose will be increased gradually to 2 mg/kg per day for six months.
The second group received 100 mg/kg of L-carnitine (Karen company in Iran) with a maximum dose of 2 g daily and low dose Propranolol (0.5 mg/kg/day) for the same time as the first group.
Patients were visited during the treatment period each month in terms of frequency and severity of attacks and a checklist was completed (Table 2). Patients in whom the frequency of vomiting attacks was reduced by greater or equal to 50% were defined as responders, and the remaining patients were classified as no responders.
Table 2. The checklist at each doctor visit
Name and surname: ……………………Date: / /
Home Phone: ……………………… Mobile: ……………….…….
|
|
Age |
|
Girl □ Boy □ |
Gender |
|
Elementary □ High School □ Middle School □ |
Education |
|
Village □ Town □ |
Location |
|
L-carnitine + propranolol □ Propranolol □ |
Medication |
|
Before taking the drug □ After taking the drug □ |
Vomiting frequency by number per month |
|
Before taking the drug 1 2 3 4 5 6 7 8 9 10 After taking the drug 1 2 3 4 5 6 7 8 9 10 |
Attack intervals by day |
|
Foods listed in the training recommendations Insomnia and poor sleep Stress TV, computer and mobile Crowded environment and cigarette smoke infectious diseases If there is a factor other than the above mentioned |
Possible factors initiating the attack |
Statistical analysis
Continuous quantitative variables were expressed as means ±SD (standard deviations) or median (IQR), if they had non-parametric distribution. Categorical variables were described as frequency (percentages). Kolmogorov–Smirnov test was utilized to assess the normality of numerical data. Levene’s test was also used to check equality of variances.
To compare the means of the numerical data between two groups, independent t-test was used. To compare of the median for variables with non-parametric distribution between the groups, Mann-Whitney test was utilized. The paired t-test was used to test mean difference between pairs of measurements for variables with normal distribution and Wilcoxon test was used for non-parametric distribution.
The Chi-Square test was applied to compare frequencies of the categorical variables among two treatment groups. All statistical analyses were performed using SPSS 20.0 for Windows. P value less than 0.05 was considered as statistically significant.
Results
One of the patients in the L-Carnitine + Propranolol group was excluded from the study due to non-acceptance of the drug. The data of 75 patients aged 3-17 years old was analyzed. 37 patients were treated with L-Carnitine + Propranolol and 38 patients with Propranolol. The mean age of the patients was 9.55 ±2.74 years. There were no differences in age, gender, and level of education between the two groups (p>0.05) (Table 3). Possible factors of initiating the attack in patients for two treatment groups were reviewed and compared (Figure 2).
Table 3. Characteristics of patients by drug treatment
|
|
L-Carnitine+ Propranolol (N=37) |
Propranolol (N=38) |
p-value |
||
|
Continuous variables |
Mean |
SD |
Mean |
SD |
|
|
Age |
9.68 |
3.13 |
9.42 |
2.34 |
0.692 |
|
Categorical variables |
N |
% |
N |
% |
|
|
Gender: Boys |
21 |
56.8% |
16 |
43.2% |
0.204 |
|
Gender: Girls Pre school |
16 4 |
43.2% 50% |
22 4 |
56.8 50% |
0.545 |
|
Elementary |
23 |
46.9% |
26 |
53.1% |
|
|
Guidance |
6 |
50% |
6 |
50% |
|
|
High school |
4 |
66.7% |
2 |
33.3% |
|
Statistical analysis of the results shows that vomiting frequency in both groups of treatment with Propranolol alone and in combination with L-Carnitine and propranolol before and after treatment was significantly reduced, but there is no significant difference between the two groups (70.6 vs. 90.9%) (p-value=0.062).
There was no significant reduction in the duration days between vomiting attack index in both groups (31.6vs.43.2%) (p-value= 0.345). Regarding the score attack in vomit episode in both groups, there was a significant decrease after starting the treatment and compared to the two groups, patients treated with propranolol had a better response (78.9 vs. 78.4%) (p -value=0.99) (Tables 4 and 5).
Table 4. Comparison of the patients’ clinical data in two treatment groups
|
|
|
L - Carnitine + Propranolol (N=37) |
Propranolol (N=38) |
Pm |
||||||
|
|
|
Median |
(Min-Max) |
Mean |
SD |
Median |
(Min-Max) |
Mean |
SD |
|
|
Vomiting frequency (monthly) |
Before |
3 |
(0-10) |
2.81 |
2.12 |
3 |
(0-7) |
2.68 |
1.65 |
0.966 |
|
After |
0 |
(0-3) |
0.49 |
0.93 |
0 |
(0-4) |
0.89 |
1.47 |
0.406 |
|
|
Pw |
|
<0.001 |
|
|
|
<0.001 |
|
|
|
|
|
duration days between vomiting attack |
Before |
10 |
(3-120) |
25.46 |
32.45 |
10 |
(4-90) |
19.37 |
21.32 |
0.743 |
|
After |
15 |
(0-365) |
52.84 |
87.90 |
7 |
(0-240) |
37.16 |
67.15 |
0.518 |
|
|
Pw |
|
0.207 |
|
|
|
0.58 |
|
|
|
|
|
Score attack in vomit episode |
Before |
7 |
(3-10) |
6.76 |
2.23 |
6 |
(3-10) |
6.47 |
1.87 |
0.443 |
|
After |
1 |
(0-7) |
1.57 |
1.98 |
1 |
(0-6) |
2.32 |
1.92 |
0.014 |
|
|
Pw |
|
|
<0.001 |
|
|
<0.001 |
|
|
|
|
Pm: p-values obtained from Mann-Whitney test; Pw: p-values obtained from Wilcoxon test.
Table 5. Response to treatment in 75 cases with CVS
|
Variables |
Percent of cure |
Propranolol + L-Carnitine (N=37) |
Propranolol (N =38) |
p-value |
|
Vomiting frequency (Monthly) |
< 50% |
3 (9.1%) |
10 (29.4%) |
0.062 |
|
>= 50% |
30 (90.9%) |
24 (70.6%) |
||
|
Duration days between vomiting attack |
< 50% |
21 (56.8%) |
26 (68.4%) |
0.345 |
|
>= 50% |
16 (43.2%) |
12 (31.6%) |
||
|
Score attack in vomit episode |
< 50% |
8 (21.6%) |
8 (21.1%) |
0.99 |
|
>= 50% |
29 (78.4%) |
30 (78.9%) |
Discussion
Given that CVS interferes with patients’ quality of life during attacks, it is important to find an effective treatment for the disease although there are several treatments shown to prevent CVS attacks. The aim of this study was to compare the effect of standard dose of propranolol with combination of L-carnitine and low dose propranolol in prophylaxis of CVS, which showed that two groups had approximately the same response (Table 4). Although several different medications have been shown to be helpful in preventing CVS attacks, no specific treatment for CVS has been established in controlled trials in children and as a result treating CVS in children is problematic and time consuming. Propranolol is a B–blocker and one of the recommended medications as prophylaxis for CVS. Several studies revealed its efficacy with variable results (50-92%) (2,11-15).
According to a systematic review study, a total of 244 children were treated prophylactically with antidepressants, antiepileptic, anti-migraine or other drugs. Tricyclic antidepressants reduced episodes in 67.6% of patients. Combination of L-Carnitine and Amitriptyline in 76.7% of patients and Propranolol in 86.8% of patients had improvement in symptoms and it should be noted that Propranolol is the most common anti-migraine drug used to prevent CVS in pediatric studies (11).
In a randomized trial study, they found that Propranolol displayed the efficacy of (92%) patients and showed to be more effective compared to amitriptyline (12). In another study, a total of 38 children who were treated prophylactically with two drugs, Topiramate or Propranolol, reported a response rate of 81% in the Propranolol group and 94% in the Topiramate group (13). One study compared the effects of Amitriptyline, Propranolol, and Pizotifen in children with CVS and reported 61, 50 and 50% responses, respectively (14). To increase the response to treatment, some researchers designed the studies to use combination therapies for disease prophylaxis (9, 10,11,15,16). In one randomized control trial, it was revealed that combination therapy of erythromycin with Propranolol significantly had a more promising effect than Propranolol alone (15).
The promising effect of L-carnitine on CVS has been observed in recent years (10,16). The results of a study represented that a protocol consisting of mitochondrial cofactors (coenzyme Q10 and L-Carnitine) plus Amitriptyline (or possibly Cyproheptadine in children under 5 years) reduced the incidence of vomiting by 75% (10) and a case series on 6 patients with CVS the administration of L-Carnitine, increased the duration between vomiting episodes from 1.7 months before administration to 1.1 years (16). Other studies have also shown a positive effect of L-Carnitine on these patients. The combination of co-enzyme Q and L-Carnitine are safe dietary supplements had been effective for prophylaxis of the CVS in cohort studies on children, probably through improving the mitochondrial function (10). Also, the combination of these two drugs with Amitriptyline (or possibly Cyproheptadine) was observed to be effective in preschool children (2,17).
The current research revealed that the combination of low dose Propranolol and L-Carnitine has comparable efficacy with high dose Propranolol (78.38% vs. 86.84 %) (p-value = 0.834).
In another study, propranolol was started at 1 mg/ kg per day for all the patients, and if the response was not acceptable, the dose was increased to 2 and finally 3 mg/kg per day, and eventually 80% of the patients improved, but in one third of the children, the treatment was not continued due to the complications (18).
Although there were no significant side effects reported in the Propranolol group in this study, it seems to be better tolerated due to the lower Propranolol dose and the potential for fewer complications. Additionally, in patients whose disease is based on mitochondrial disorder, this combination appears to be more appropriate than Propranolol alone.
Conclusion
The present study revealed that the combination of low dose Propranolol with L-Carnitine have comparable efficacy with high dose Propranolol in prophylaxis of the CVS.
Limitations
An important limitation of the study was the patients’ refusal to go to medical centers due to the occurrence of Coronavirus pandemic which reduced the sample size. Finally, it seems that similar studies with a larger sample size and a longer follow-up time can be more helpful and useful in the treatment of children with CVS.
Acknowledgements
This study has been approved by the ethics Iranian Registry of Clinical Trials (IRCT20120716010297N9). The authors of this study would like to thank the Research Institute for the Prevention of Non-Communicable Disease, Isfahan University of Medical Sciences for their support.
Conflict of Interest
The authors declare no conflict of interest.
Financial support and sponsorship
None.