Document Type : Case report
Abstract
Topiramate is being widely used to prevent migraine headaches and treat epilepsy and mental disorders; however, Oral Lichenoid Lesion (OLL) is one of its rare side effects. The present report has been provided based on a patient case study who had developed OLLs following treatment with topiramate. The patient was a 50-year-old woman referred to a psychiatric clinic with complaints of severe headaches, anxiety, insomnia, and symptoms of Obsessive-Compulsive Disorder (OCD). For this purpose, fluoxetine, topiramate, and nortriptyline were prescribed. Two months after increasing the topiramate dosage to 400 mg per day, she developed OLLs. The Topiramate dose was reduced within two weeks and finally discontinued. The lesions were removed four weeks after the cessation. The patient had no lesions for 6 months. With restarting the drug, the lesion reappeared and finally, ceasing topiramate usage. To conclude, the mentioned lesions are one of the rare complications of this anticonvulsant drug.
Keywords: Case report, Diagnosis, Lichenoid lesion, Oral, Side effects, Topiramate
Introduction
Topiramate which is known as an anticonvulsant and a mood stabilizer (1-3), is being widely utilized for treating neuropsychiatric disorders, alcohol abuse, eating disorders, epilepsy, migraine headaches (2,4,5), and weight loss (6). Despite its pharmaceutical advantages, topiramate administration may result in some side effects such as concentration difficulties, tongue dysfunction (1,7,8), dizziness (9), paresthesia (10), skin lesions (11), taste disturbance (12), dry mouth, and gingival hyperplasia (13,14). Pruritus is further reported as a complication associated with taking anticonvulsants (15), including topiramate (11). The term Oral Lichenoid Lesions or Reactions (OLLs/OLRs) refers to chronic inflammatory lesions of the oral mucosa that are expressed during histological examinations by dispersed lymphocytes with eosinophils and plasma cells. Such lesions are recognizable through specific symptoms and are histologically similar to Oral Lichen Planus (OLP) (16, 17). In this case report, the researchers encountered OLLs following topiramate administration in a 50-year-old woman presenting with the symptoms of Obsessive-Compulsive Disorder (OCD).
Case Report
The patient was a 50-year-old illiterate housewife, referred to a psychiatric clinic with complaints of severe headaches in 2011. The patient also had reported such headaches in the occipital lobe with 15 times a month frequency, lasting for 24-48 hours each time. In addition, she had reported periodic one-sided throbbing headaches accompanied by photophobia, nausea, and vomiting. The headaches were intensified upon performing more activities. During a psychiatric interview, the patient had complained about depression, impatience, irritability, sense of guilt, self-blame, lack of energy and fatigue, together with obsessive thoughts for two years. Therefore, based on the Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition (DSM-V) criteria, the comorbidity of Persistent Depressive Disorder (PDD) and OCD was diagnosed, and migraine headaches without an episodic tension-type diagnosis were declared with reference to the International Classification of Headache Disorders (ICHD) criteria.
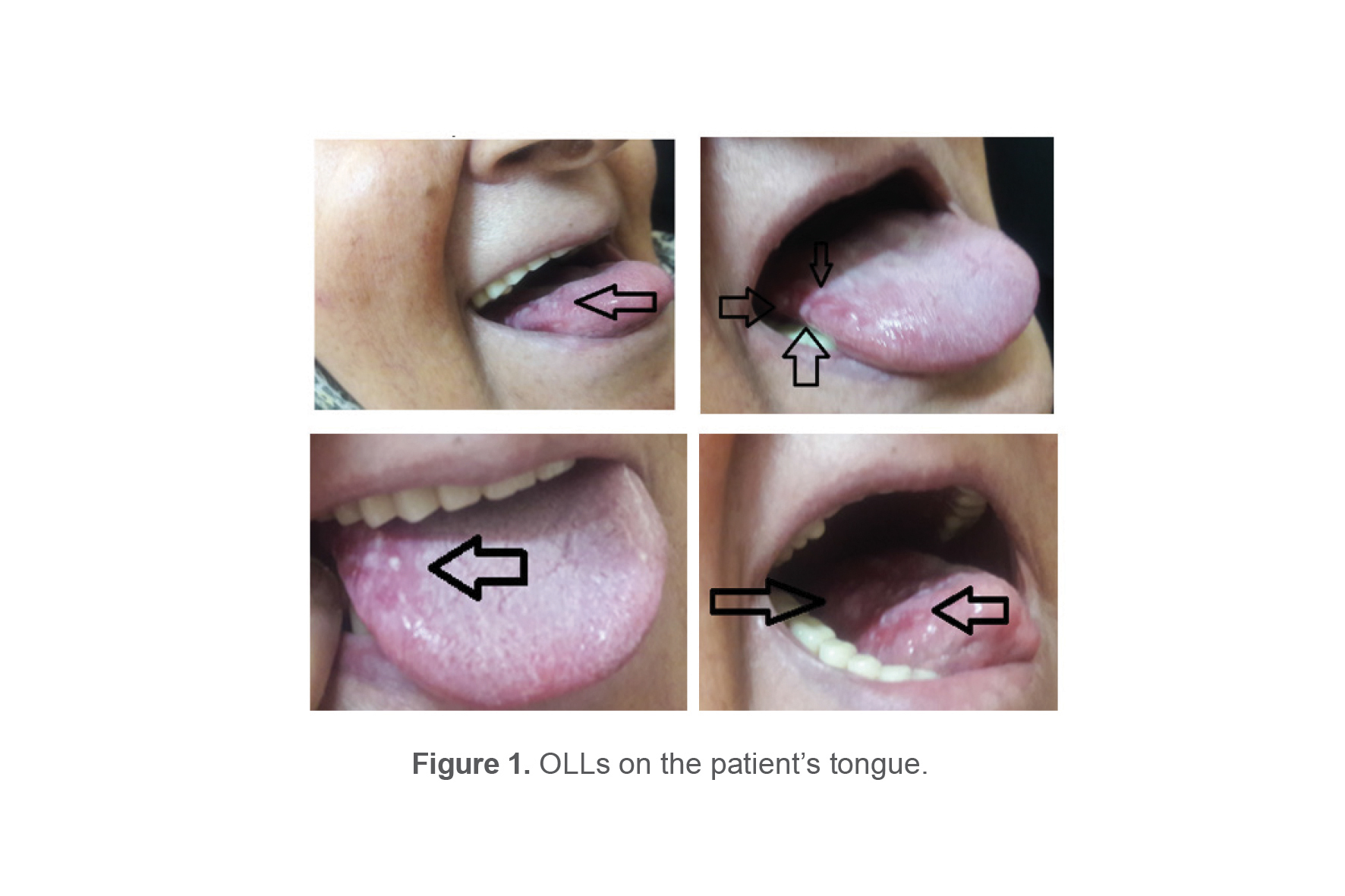
Accordingly, the treatment regimen was started with 10 mg fluoxetine daily and 0.5 mg alprazolam nightly over nine months, and then the fluoxetine dosage was gradually increased to 80 mg per day and the use of alprazolam was discontinued. Mood symptoms were improved during this period and the OCD symptoms were significantly relieved. Headache episodes were also mitigated; however, headache remained as the patient’s complaints alongside weight gain. Thus, 25 mg topiramate and 10 mg nortriptyline (once per night) dosages were added to fluoxetine. Afterward, the nortriptyline and topiramate dosages were gradually elevated to 100 and 300 mg per day, respectively. The mentioned treatment regimen significantly minimized the symptoms, but the patient’s symptoms became severe after decreasing the dosage of each drug. In a visit in the fourth year of the treatment, the patient also complained about a painful oral lesion on her tongue that could be exacerbated by drinking hot beverages. The lesion looked like a lichenoid one (Figure 1). In the same referrals, the patient declared that she had increased the topiramate dosage to 400 mg per day for the past three months due to her satisfaction with a decreased appetite. She had been referred to a dermatologist and the oral biopsy had revealed erosive OLP with mild dysplasia. There were no records of the occurrence of OLLs following the use of topiramate and nortriptyline, but the occurrence of such lesions was reported after taking anticonvulsants such as carbamazepine. Since the last change in the drugs administered prior to the occurrence of OLLs was the topiramate dosage increase, the use of this anticonvulsant was reduced for two weeks and finally discontinued, and the lesions were improved over four weeks. However, after six months, the patient who was undergoing treatment by fluoxetine and nortriptyline without any OLLs, started taking topiramate with the previous dosage (namely, 400 mg per) because of her own positive viewpoint to its effectiveness, and the OLLs appeared once again.
Discussion
This case represents one of the side effects of topiramate-induced OLLs. It should be noted that mouth and tongue are affected by the drug reactions and chemical complications (18). Topiramate can cause an increase in extracellular matrix production and in the number of cellular components and collagen that may lead to gingival hyperplasia. This drug is associated with chronic inflammation caused by dental plaque. On the other hand, Antonio et al showed growth of the fibrous tissue which may be possible in OLLs (18,19). Such oral changes are also seen after taking some drugs such as lithium, carbamazepine, and phenytoin (14,17), but symptoms such as headaches, insomnia, weight gain, and depression improve (5). Biopsy confirmed the lichenoid nature of the oral lesions. Also, The Naranjo Drug Reaction Probability Scale (NDRPS) was also used to address the causative role of topiramate. According to this criterion, the probability of an unpleasant therapeutic, preventive, diagnostic approach and the side effects in patients’ prior exposures could be assessed based on a list of questions investigating the side effects of either using or stopping the drugs (20-22). In this report, the NDRPS score was equal to 9. Considering this criterion, the scores could range from 4 to 13, wherein the scores >9 verified drug-induced reactions, the scores 5-8 suggested the probing ability, while the scores 1-4 indicated the possibility of drug-induced reactions. Finally, the scores of zero and below could raise the suspicion of drug reactions. According to the interpretation of this criterion, a reaction to topiramate was diagnosed (Table 1).
Table 1. NDRPS score
|
Questions |
Yes |
No |
Unknown |
Score |
|
1. Are there previous conclusive reports on this reaction? |
0 |
0 |
0 |
0 |
|
2. Did the adverse event appear after the administration of the suspected drug? |
+1 |
0 |
0 |
+1 |
|
3. Did the adverse event improve once the drug was discontinued or a specific antagonist was administered? |
+1 |
0 |
0 |
+1 |
|
4. Did the adverse event reappear upon the topiramate reintroduction? |
-1 |
+2 |
0 |
+1 |
|
5. Are there alternative causes that could have induced the reaction on their own? |
+2 |
+2 |
0 |
+4 |
|
6. Did the reaction reappear once a placebo was given? |
0 |
0 |
0 |
0 |
|
7. Was the drug detected in the blood or other body fluids in concentrations known to be toxic? |
0 |
0 |
0 |
0 |
|
8. Was the reaction more severe when the dosage was increased or less severe once the dosage was decreased? |
+1 |
0 |
0 |
+1 |
|
9. Did the patient experience a similar reaction to the same drugs in any previous exposures? |
0 |
0 |
0 |
0 |
|
10. Was the adverse event confirmed by any objective evidence? |
+1 |
0 |
0 |
+1 |
|
|
5 |
4 |
0 |
9 |
This type of drug reaction has been also reported with glibenclamide and atenolol. OLLs have further developed following long-term oral administration of both drugs (23). In this regard, medications such as capecitabine and lapatinib, as well as zolendronic acid and lansoprazole were prescribed for a patient with breast cancer. Consequently, minute pustules developed within 24 hours and then disappeared followed by painful lichenoid lesions on the front of the tongue. This phenomenon preceded the appearance of painful OLLs on the anterior part of the tongue. According to the score 6 obtained using the NDRPS, an adverse reaction to capecitabine was probable, which was then verified by the fading of the symptoms following the adjustment of the drug dosage (19). The results of the above-mentioned studies were in line with the observations in this case report, in which boosting the topiramate dosage from 300 to 400 mg per day triggered lesions, diagnosed as OLLs, based on the clinical-pathological examinations and the NDRPS, but it disappeared after the drug withdrawal. Then, the patient’s oral symptoms resolved (14,17,18). In this study, the patient’s oral symptoms resolved following the topiramate dosage reduction and withdrawal.
Another category of anticonvulsants that can develop such side effects was further observed in a 51-year-old man visiting a clinic to treat bipolar disorder. He had taken 300 mg lithium twice a day for two years. Since oral atrophic lesions had not been observed before, histopathological examinations had reported OLLs as reactions against lithium consumption. Later, the psychiatric team had used prednisolone for 15 days for therapeutic purposes, which had been effective in minimizing the side effects (24). The results of the present and previous reports accordingly stipulated that various drugs, especially in high dosages, might induce OLRs on their long-term consumption (14). Further, the score of 9, according to the NDRPS in the present study, indicated the drug-induced nature of the reaction. Given the prevalence rate of this side effect (25), further studies on the benefits and harms of this medication are required. In conclusion, physicians and psychiatrists must be familiar with OLLs as a rare side effect of topiramate.
Acknowledgements
The authors are grateful to the Mazandaran University of Medical Sciences for its support. We appreciate the patient for her nice cooperation. Informed consent was obtained from the patient (Ethic code: IR.MAZIMS.TEC.1401.14925).
Conflict of Interest
None declared.
Declaration of Patient Consent
The authors certify that they have obtained appropriate patient consent.