Document Type : Review article
Abstract
Background: Poisoning is a substantial type of unintentional injury in children that is associated with significant mortality and morbidity.
Methods: This study reviewed the patterns of poisoning in children in Iran.
Results: Based on the results of the studies, the prevalence of poisoning is higher in boys and the most poisoned children were in the age group of 1 to 3 years. Drugs were the main toxic factors, followed by narcotics and opium. The rate of poisoning was higher in urban areas. Neurological symptoms were the main signs and symptoms in poisoned children. Most patients were completely cured and the mortality rate was about 2%. Family addition, unsafe storage of drugs, and lack of parental supervision over children were the main risk factors for poisoning among children.
Conclusion: Unintentional poisonings are still common among children in developing countries. Drug poisoning is the main cause of poisoning in children. Therefore, increasing knowledge and awareness about the types of poisoning and how to prevent it is very important in preventing childhood poisoning.
Keywords: Children, Iran, Pattern, Poisoning
Introduction
Poisoning is a significant unintentional injury in children and is associated with significant mortality and morbidity. The World Health Organization (WHO) reported that the estimated death rate for children and youth under the age of 20 is 45,000 deaths per year (1).
According to the report of the American Association of Poison Control Centers’ National Poison Data System in 2017, 50% out of the 2 million calls for human poisonings resulting from toxic substances involved children under 13 years of age (2). Seven percent of all accidents in children under 5 years of age are associated with poisoning, and it accounts for 2% of child deaths in developed countries and more than 5% of child deaths in developing countries (3,4). Children between the ages of 1 and 5 years are at the highest risk of poisoning and account for 80% of all child poisoning cases (5). Poisoning was defined as the fourth leading cause of accidental death in children (6). The death rate due to poisoning in children is about four times higher in low- and middle-income countries (1).
Child poisoning may be unintentional or intentional, but most of these cases in children are involuntary and out of curiosity (7). Poisoning patterns vary in different geographical areas with different social, cultural, occupational, economic and environmental risk factors and the availability of substances or poisons. Thus, to manage and prevent this problem, there is a need for epidemiological studies related to each country and region (8). The present study was conducted with the aim of investigating the patterns of childhood poisoning in Iran.
Materials and Methods
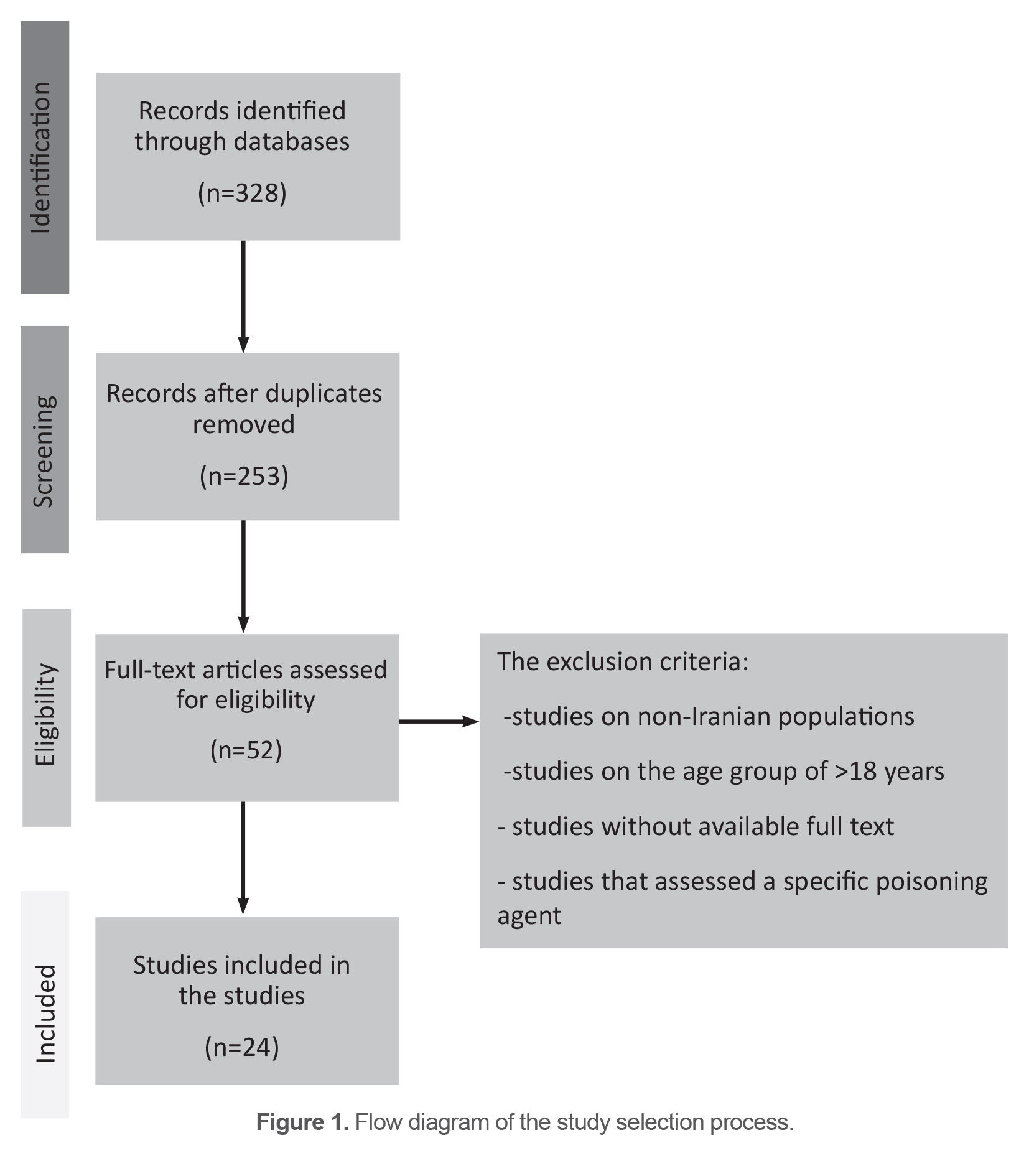
In this review study, all studies related to poisoning in children in Iran from 2000 to 2022 were evaluated and the articles were searched through PubMed, Scopus, Science Direct and Google Scholar databases using the keywords “Poisoning”, “Poisoning in children”, “Poisonous substances”, and “Iran”. The inclusion criteria included all Persian and English articles that evaluated the epidemiology of childhood poisoning in the Iranian population and age less than 18 years. Exclusion criteria consisted of studies on non-Iranian populations, studies in the age group above 18 years, studies without full text available, and studies that evaluated a specific toxic agent. A total of 253 articles were extracted in the primary search. After reviewing the full texts of these articles, finally 24 articles that met the necessary criteria were selected and fully evaluated. The flow diagram of the study selection process is shown in figure 1.
Table 1. Trends of sex, age, location, and geographical area of childhood poisoning in Iran
|
|
No. |
Sex |
Age (years) |
Location |
Area |
|
Arjmand Shabestari et al (9) |
224 |
54.9% boys |
3.54±2.99 50.9%(1-3 ys) |
Arak |
|
|
Momayyezi et al (10) |
238 |
58% girls |
<15 |
Yazd & Taft |
82.8% urban areas |
|
Nafei et al (11) |
105 |
61.9% boys |
55.2% in the 1-4 age group |
Yazd |
|
|
Shirdelpour et al (12) |
2160 |
64.3% boys |
51.4% in the 1-3 age group |
Rasht |
|
|
Mojtabayi et al (13) |
141 |
|
Mostly in the age range of 1-5 y |
Rasht |
|
|
Gheshlaghi et al (4) |
344 |
50.6% boys |
3.07±1.43 |
Isfahan |
|
|
Shirkosh et al (14) |
408 |
55.4% boys |
36.27±2.8 55.1% (1-3 y) |
North of Iran |
56.6% urban areas |
|
Ayubi et al (15) |
140 |
42.8% boy |
3.7±2.5 |
Tehran |
|
|
Ahmadabadi et al (20) |
102 |
59% boys |
Mostly between 1-3 y |
Tabriz |
58.8% urban area |
|
Manouchehrifar et al (16) |
414 |
57.5% boys |
4.2±3.43,67.9% (0-4 y) |
Tehran |
|
|
Mohammadi et al (21) |
184 |
59.8% boys |
3.4±2.4 |
Qazvin |
|
|
Pirzadeh et al (17) |
434 |
63.36% boys |
79.5% <6 y |
Qazvin |
|
|
Talebian et al (18) |
119 |
66.4% boys |
66.3% between 1-4 y |
Kashan |
68% urban area |
|
Zare et al (23) |
729 |
50.1% boys |
Mostly <5 y |
Urmia |
|
|
Haresabadi et al (19) |
211 |
58.8% boys |
Mostly <6 mo |
Bojnurd |
56.9% rural area |
|
Ghoreyshi et al (26) |
306 |
53.3% boys |
31% (1-2 y) |
Tabriz |
|
|
Kashef et al (25) |
690 |
60% boys |
Mostly (1-5 y) |
Shiraz |
|
|
Motlagh et al (24) |
110 |
58.2% boys |
Mostly (1-3 y) |
Ahvaz |
|
Age and gender
In a study in Arak on children with acute poisoning, 54.9% of them were boys and 50.9% of the children were in the age range of 1 to 3 years (9). In another study in Yazd and Taft cities on children who were less than 15 years old, 58% of the children were girls (10). Another study in Yazd showed that among 105 under the age of 18, 61.9% were boys. The age group of 1 to 4 years indicated the highest rate of poisoning (11). In Shirdelpour et al’s study on cases of poisoning, 64.3% of them were boys and 51.4% of the children were between the ages of 1-3 years (12). Mojtabayi et al study demonstrated that 86.5% were below the age of 5 years and most of the cases were in the age range of 1-5 years (13). In another study in Isfahan, of 344 children, 50.6% were males with a mean age of 3.07±1.43 years. 89.5% of them were under 6 years and 10.5% were between 6-10 years. 44.7% of the intoxicated children were between 1-3 years of age (4). Out of 408 poisoning cases among children in a study in Northern Iran, 55.4% were boys, and the mean age of the cases was 36.27±2.8 months. 55.1% were in the age range of 1-3 years (14). Ayubi et al assessed 140 poisoned children in Tehran and reported that 42.8% of them were boys and the mean age of the cases was 3.7±2.5 years (15). Manouchehrifard et al’s study in Tehran city showed that out of 414 poisoned children, 57.5% were male. The mean age of the patients was 4.2±3.43 years and 67.9% of the children were in the age range of 0-4 years (16). Pirzadeh et al’s study in Qazvin reported that 63.36% of the poisoned cases were male and 79.5% of the patients were under 6 years old (17). The rate of boys was shown to be 66.4% among 119 cases in a study in Kashan and the main age range of poisoning was between 1 to 4 with the rate of 66.3% (18). In an epidemiological study in Urmia on children poisoning the rate was almost similar in boys (50.1%) and girls (49.9%), and the uppermost rate was observed among children under 5 years old (46%). According to studies, boys have accounted for a higher percentage of poisoning cases and most of the poisoned cases were under the age of 5 years old and mostly between 1-3 years old which are mentioned in table 1 (19-25).
Geographical area
In the study by Momayyezi et al in Yazd and Taft cities, 82.8% of poisonings in children happened in urban areas (10). In a study in Northern Iran, 56.6% of the children’s poisoning cases were related to the urban area (14). According to the study in Tabriz city, 58.8% of the poisoned children lived in urban areas. Drugs, pesticides, and detergents were the main reason for poisoning in urban areas. Poisonous mushrooms and petroleum products were the main agents of poisoning the rural areas (20). The reason for a higher rate of poisoning in urban areas in comparison to rural areas may be due to easier accessibility of drugs and the higher consumption of drugs, chemical materials, as well as cleansing products in urban areas. Moreover, the higher population and the accessibility of hospitals and medical centers are easier in the urban areas and the hospitalization of children due to poisoning is, therefore, higher in these areas. In a study in Kashan, 68% of the cases were residents in the urban area. In urban areas, drugs were the main agents and in rural areas, oil was the main agent of poisoning among children (18). However, in the Haresabadi et al’s study, 56.9% of the poisonings occurred in rural areas (19) (Table 1).
Type of poisonous agents
In the Momayyezi et al’s study, drug poisoning was defined as the main cause of poisoning in children (60.5%), followed by cleansing products (10.1%), drugs-opioids, and pesticides (10). In Nafei et al study in Yazd, 51.4% of the poisoning cases were associated with drugs and opioid analgesics were the most prevalent drugs (11). According to Ayubi et al study, the main types of poisoning were related to narcotics, and among them, methadone was the most common poisoning agent (15). Arjmand Shabestari et al in a study in Arak reported that drugs mainly benzodiazepines, gastrointestinal drugs, and opioid analgesics (65.2%), kerosene (7.1%), as well as food poisoning (5.4%) are the most prevalent reason for poisoning (9). According to Gheshlaghi et al’s study, 58.1% of the agents causing the poisoning were drugs, 13.1% were hydrocarbons, and 9.3% were opioids (4). Ahmadabadi et al in Tabriz showed that pharmaceutical products accounted for 50% of the poisoning agents followed by pesticides, poisonous mushrooms, and petroleum (20). In a study in Tehran city, methadone (29.7%) was determined as the most prevalent toxic agent in children (16). In a study in Qazvin on 184 cases, it was demonstrated that methadone, other narcotics, as well as psychotropic medications were the main poisoning agents (21). In Bojnurd, the most common causes of poisoning in children were opium (63.5%) and then drugs (19). Mansouri et al revealed that 58.6% of childhood poisoning was associated with narcotics and that methadone was the most common poisoning narcotics (74.7%) (27). According to a study in Loghman Hakim poison control center on 1120 children, pharmaceuticals were the main reason for poisoning among children (28) According to Sabzi et al ‘s study in Gorgan on 6053 poisoned children, 39.63% of poisoning was related to opium and 24.39% to drugs and kerosene, household chemicals, methadone, and mouse killer were at next places (29). Concerning the studies, drugs were the main reason for poisoning in many of the children (12,13,17,18,22,24-26) (Table 2).
Clinical symptoms
The most common symptoms of poisoning in children in the Arjmand Shabestari et al’s study included neurological, gastrointestinal, respiratory, psychological, and fever (9). Neurological signs and hypoglycemia are determined as the main clinical symptoms of poisoning in the Momayyezi et al study (10). In Gheshlaghi et al’s study, neurological signs and then lethargy were the most common signs in children (4). In Shirkosh et al’s study, the loss of consciousness was the main manifestation (14). Neurological signs such as lethargy and coma were the most signs observed in Sadeghi-Bojd and Khajeh’s study (22). Mohammadi et al revealed that lack of consciousness (77.7%), nausea, and vomiting (30.4%) were the main symptoms of poisoning (21). Pirzadeh et al reported neurologic symptoms as the most prevalent presentation of acute poisoning in children (17). In the Talebian et al’s study, the main symptom was gastrointestinal generally. Respiratory symptoms were the main symptom of oil poisoning and neurological symptoms were the main signs of drug poisoning (18). According to Nafei et al’s study, 23% of the poisoned children were asymptomatic, 33% showed loss of consciousness, 20% had gastrointestinal symptoms and respiratory symptoms, restlessness, and seizure were other symptoms in these children (11) (Table 2).
Clinical outcomes
In the Mohammadi et al’s study, 1.1% of the patients were discharged with neurological complications. 65.8% of the patients were discharged with well and 33.2% with satisfactory conditions (21). Pirzadeh et al showed that 10.36% of the patients were admitted to the pediatric intensive care unit. %0.06 of the deaths happened with monoxide carbon and methadone (17). Zare et al’s study reported 2.9% deaths among 729 poisoned children (23). In the Gheshlaghi et al’s study, 91.6% of the patients were discharged with complete treatment, 6.7% were discharged with rare problems and 1.5% of the patients died due to poisoning (4). In the Nafei et al’s study, all of the children were discharged after recovery and the mean hospitalization time was 2 days and 8 hours (11). In a study in Zahedan, the rate of death as a result of poisoning in children was almost 2%. The deaths occurred due to drug poisoning, hydrocarbon intoxication, and kerosene. Dysrhythmia was the cause of death in two children (22). Shirkosh et al’s study reported that the mean duration of hospital stay in children was 2.7±2.1 days, and 68.3% of the children treated and discharged, and only one death occurred (0.2%) (14). In the Haresabadi et al’s study, the mean time of hospitalization as a result of poisoning was 2.6 days (19). According to Ghoreyshi et al’s study, the mean duration of hospitalization was 2 days and 2 out of 306 patients died (26). The mortality rate in pediatric poisoning was 0.8% in Kashef et al’s study (25) (Table 2).
Table 2. Trends of poisoning agents, symptoms, outcome, and risk factors of childhood poisoning in Iran
|
|
Poisonous agents |
Symptoms |
Outcome |
Risk factors |
|
Arjmand shabestari et al (9) |
Benzodiazepines, gastrointestinal drugs, and opioid analgesics (65.2%), kerosene (7.1%), food poisoning (5.4%) |
Neurological, gastrointestinal, respiratory, psychological, and fever |
|
|
|
Momayyezi et al (10) |
Drug poisoning (60.5%), cleansing products (10.1%), drugs-opioids, and pesticides |
Neurological signs and Hypoglycemia |
|
|
|
Nafei et al (11) |
Drugs and opioid analgesics |
Loss of consciousness, gastrointestinal symptoms followed by respiratory symptoms, restlessness, and seizure |
All of them discharged |
Family size of 5 or more |
|
Shirdelpour et al (12) |
Medicine (51.4%), Opium and its derivatives (11.4%), and cleaner (7.1%) |
|
|
Father’s level of education, the mother’s job, and low rate of parental awareness |
|
Mojtabayi et al (13) |
Drugs (56.73%) and kerosene (9.92%) |
|
|
|
|
Gheshlaghi et al (4) |
Drugs (58.1%), hydrocarbons (13.1%), opioids (9.3%) |
Neurological signs and then lethargy |
91.6% were discharged with complete treatment, 6.7% were discharged with rare problems and 1.5% died |
|
|
Shirkosh et al (14) |
|
Loss of consciousness |
68.3% discharged, and one death |
|
|
Ayubi et al (15) |
Narcotics (mainly methadone) |
|
|
No supervision, parents were narcotic addicted, lack of attention to the storage of toxic materials |
|
Ahmadabadi et al (20) |
Pharmaceutical products (50%) followed by pesticides, poisonous mushrooms, and petroleum |
|
|
Parental smoking and the rate of storage of drugs in unsafe places |
|
Sadeghi-Bojd et al (22) |
Drugs and analgesics-antipyretics |
Neurological signs such as lethargy and coma |
2% death due to Dysrhythmia |
|
|
Manouchehrifar et al (16) |
Methadone (29.7%) |
|
|
History of addiction in the family |
|
Mohammadi et al (21) |
Methadone, other narcotics, psychotropic medications |
Lack of consciousness (77.7%), Nausea, vomiting (30.4%) |
1.1% were discharged with neurological complications. 65.8% were discharged with well and 33.2% with the satisfactory condition |
|
|
Pirzadeh et al (17) |
Mostly drugs followed by methadone, benzodiazepines, and kerosene |
Neurologic symptoms |
10.36% were admitted to the pediatric ICU, % and 0.06% died |
|
|
Talebian et al (18) |
drugs, oil, and food |
Gastrointestinal, Respiratory symptoms, neurologic symptoms |
|
|
|
Zare et al (23) |
Drugs followed by petroleum and food |
|
2.9% death |
|
|
Haresabadi et al (19) |
Opium (63.5%) and then drugs |
|
|
|
|
Ghoreyshi et al (26) |
Drugs and hydrocarbons |
|
2 deaths |
|
|
Kashef et al (25) |
Drugs, chemicals, and narcotics |
|
0.8% death |
|
|
Motlagh et al (24) |
Kerosene (43.6%), drugs (31.8%), narcotic substances (13.6%) |
|
|
|
|
Mansori et al (27) |
58.6% narcotics mostly methadone |
|
|
Addiction in the family, previous poisoning, maternal occupation, and inaccessibility of poisoning products |
|
Sabzi et al (29) |
39.63% opium and 24.39% drugs and kerosene, household chemicals, methadone, and mouse killer |
|
|
|
Risk factors
According to Mansori et al’s study in Tehran, addiction in the family (OR=14.6), previous poisoning (OR=7), maternal occupation (OR=4), and inaccessibility of poisoning products (OR=0.03) were the most common risk factors in accidental childhood poisoning (27). In the Shirdelpour et al’s study, a significant difference was observed between case and control groups in terms of the father’s level of education and the mother’s job. They believed that the low rate of parental awareness contributed to these children’s poisoning (12). In the Nafei et al study, 50% of the cases had a family size of 5 or more. They reported that in families with more than 2 children, parents perhaps have less supervision of their children, and this increases the risk of unintentional poisoning in children (11). In Ayubi et al’s study, 25% of the poisoning occurred while children were not supervised by parents or caregivers. The largest Population Attributable Risk (PAR) was observed when parents were narcotic addicts (57%). The PAR for lack of attention to the storage of toxic materials and their accessibility and parental smoking were 54, 41, and 54%, respectively (15). In Ahmadabadi et al’s study on poisoning in children, the rate of parental smoking was 88.2% and the rate of storage of drugs in unsafe places was 83.3% (20). According to Manouchehrifar et al’s study, the history of addiction in the family was significantly higher in unintentional poisoning of children (16) (Table 2).
Discussion
According to the results of the studies evaluated, almost all of the studies showed that the prevalence of childhood poisoning is higher among boys (9,11,12,14-22) and only one study in Yazd demonstrated that the rate of poisoning is higher in girls (10). Maybe it is due to the nature of the boys who are more hyperactive and adventurous than the girls. Studies showed that children within the age group of 1 to 3 years are more likely to be poisoned (4,9,12,14,20). Children in the age range of 1 to 3 years are in the curiosity stage of development and want to explore their environment and therefore are at risk of accidental poisoning.
Concerning the studies, a greater rate of poisoning was observed in urban areas (10,14,18,20). The reason for the increase in poisoning in urban areas is more access to drugs, detergents and chemicals in urban areas. In addition, the population is more in urban areas, and as a result, poisonings have more referrals to hospitals.
The drug was reported as the most common poisoning agent in children (4,9-12,18,25,26). After drugs, narcotics, and opium (11,12,15,19,25), mostly methadone,(16,17) were reported as the highest poisoning agents. Kerosene (9,13), hydrocarbons (4,26), and food poisoning (9,18,23) were other poisoning factors for children which are mentioned in the studies. Studies revealed Neurological symptoms as the main symptoms in poisoned children (4,9,10,17,18,22). After that loss of consciousness (11,14,21), gastrointestinal symptoms (9,11,18), respiratory signs (9,11,18), and lethargy (4,22) are the most common signs and symptoms of poisoning among children.
With regard to the clinical outcome, most of the children were discharged with complete recovery, and a low percent were discharged with rare complications (4,11,21,22). The rate of death as a result of childhood poisoning was between 0.06 to 2.9% (4,14,17,22,23,25). The length of hospitalization was from 2 to 2.7 days among poisoned children (11,14,19,26). The most common risk factors for childhood poisoning were addiction in the family, unsafe storage of drugs, parental smoking, maternal occupation, father’s level of education, and lack of supervision of a child by parents or caregivers (12,15,16,20,27).
The result of the present study is consistent with a result of a recent systematic review by Ghasemlo et al in Iran that reported a higher prevalence of poisoning among boys and children under 3 years of age. They reported medication and opium as the main toxic agents (30). Another systematic review in Iran by Alijani et al reported that 54.7% of the participants were boys, mostly in the age range of 3-5 years. Non-pharmaceutical agents were the most common causes of poisonings (59.2%) and among them, illicit drugs (mainly opioids) and hydrocarbons were the most common non-pharmaceutical poisonings. Among pharmaceutical agents, especially benzodiazepines and analgesics were the most frequent poisoning agents implicated. Regarding symptoms, CNS complaints, as well as gastrointestinal complaints, were the prevalent symptoms. The mortality rate was 0.8% (31).
The strength of this study is that it has evaluated many regions and cities of Iran and can provide comprehensive information about the trend of child poisoning in Iran. The present study also had limitations. Most of the studies used in this review are retrospective studies based on hospital data, which may be recorded with low precision, which can be considered as a weakness of this study.
Conclusion
In developing countries, accidental poisoning is still one of the main causes of complications in children. Considering the significant prevalence of drug poisoning in Iran, storing drugs in a safe place is of great importance. Therefore, increasing knowledge and awareness about the types of poisoning and ways to prevent it through educational workshops, media and health centers can be an important step towards maintaining children’s health.
Ethical considerations
The study was performed according to Helsinki’s Principles of Ethics. Since this is a literature review, the study is exempt from obtaining an ethical code.
Acknowledgements
There is no acknowledgment for the present study.