Document Type : Original article
Abstract
Background: Congenital Heart Disease (CHD) is the most common congenital malformation in infants. The burden is defined as the perceived caregiver’s sufferings of their emotional or physical health, social and financial life as a result of caring for loved ones. Lifelong CHD endures significant burdens on patients, families, and society. Parents of children with chronic illnesses such as CHD are more likely to be challenged than other parents. Furthermore, evidence shows the impact of this burden on parents’ health. Therefore, this study aimed to evaluate the burden on caregivers of patients with CHD.
Methods: In this cross-sectional study, 72 caregivers of patients with CHD in the Children’s Medical Center, Tehran, Iran were recruited. Face-to-face interviews with caregivers had been done. The demographic and disease-related data were collected. Zarit Burden Interview (ZBI) was applied for disease burden assessment. Statistical analysis was performed in SPSS version 22.
Results: In the present study, most caregivers 34 (47.2%), suffered from moderate to severe burden. The mean caregiver burden score was 42.78 which is categorized as a moderate to severe burden score. The siblings’ number and level of caregivers’ education had a significant association with the caregiver’s disease burden.
Conclusion: CHD is associated with a significant caregivers’ disease burden. Although the disease-related factors were not related to disease burden, the higher caregivers’ education was related to fewer caregivers’ disease burden. Therefore, paying attention to the caregiver’s burden is an important clinical issue.
Keywords: Burden, Caregiver, Congenital heart disease, Zarit burden interview
Introduction
Congenital Heart Disease (CHD) is the most common congenital malformation in infants and is the leading cause of death from congenital anomalie (1). CHD is a structural disorder of the heart caused by abnormal growth and development of the heart and large vessels (2). The prevalence of CHD varies in different geographical places. In North America, CHD occurs in 8.1 per 1000 live births, whereas in Asia the prevalence is 9.3 per 1000 live births (3). In two studies conducted in Iran, the mean prevalence of CHD was reported as 8.6 per 1000 live births and 12.3 per 1000 live births (4,5). CHD is a multifactorial disease in which environmental and genetic factors play an important role in its pathogenesis (6). Over the past decades, the population of patients with congenital heart defects has increased dramatically, which can be attributed to improved surgical outcomes and advances in medical treatment (7). The severity and type of CHD affect the severity and complications of the disease (8). Due to the increment in life expectancy of these patients, the attention of recent studies was shifted towards long-term complications (8). The burden is defined as the perceived caregiver’s sufferings of their emotional or physical health, social and financial life as a result of caring for loved ones (9). Lifelong CHD endures significant emotional and economic burdens on patients, families, and society (3). Children with CHD are more likely to develop psychiatric disorders, neurodevelopmental disorders, and emotional problems (10). CHDs are among the congenital defects of children that lead to the longest hospital stay, the highest mortality rate, and the highest medical and hospital costs (11). Due to the nature of the disease and its complications, patients have an exclusive need for personal, emotional, and social support at different stages of life, and most of the burden of such support and care is on their families. Parents of children with CHD encounter significant emotional stress since they were informed of their child’s CHD, also some of them were informed of the diagnosis before the child’s birth, so they have faced more prolonged stress (12). On the other hand, fear of subsequent treatment plans and illness outcomes may cause a psychosocial problem in caregivers, especially their mothers (13). Parents of children with chronic illnesses such as CHD are more likely to be challenged than other parents. Further, evidence shows the impact of this burden on parents’ health (14). Prolonged caregivers’ burden can result in parents’ social isolation, stress, hopelessness, anxiety, and depression (15,16). Therefore, this study aimed to evaluate the burden on caregivers of patients with CHD.
Materials and Methods
Participants
In this analytical cross-sectional study, the caregivers of patients with CHD who were referred to the Children’s Medical Center, in Tehran, Iran from 2019 to 2020 were selected. Family caregivers were defined as co-resident family members who are responsible for most of the patients’ daily care and needs. Among the referred patients, 79 caregivers met the inclusion criteria, and 72 caregivers were satisfied to participate in this study. All 72 caregivers signed an informed consent. The caregivers’ inclusion criteria were 1. Having a child between the ages of 0 month and 10 years with CHD who are still being treated (Cardiology care), 2. Living with their children at home and, parents were responsible for their care, 3. Not having another child with pervasive developmental disorders such as autism, pervasive genetic disorders, Down syndrome, and intellectual disability, and 4. The child with CHD with no mental disorder such as autism, pervasive genetic disorders, Down syndrome, and intellectual disability. Sampling was done by available and non-random methods. Face-to-face interviews with caregivers had been done. Demographic information such as child and caregiver age, caregiver education, caregiver occupation, marital status, number of children, having another child or children with heart or physical problems, and guardianship by one or both parents were acquired during the face-to-face interviews by the researcher and then entering the special information sheets. Moreover, disease characteristics data like type of CHD, age of CHD diagnosis, history of cardiac surgery, and age of surgery were gathered.
Measures
Disease burden assessment was done by Zarit et al’s questionnaire (9). All of the participants completed Zarit Burden Interview Questioner (ZBI). It is the most common tool for measuring disease burden. This questionnaire includes 22 questions about the psychological burden and personal, social, emotional, and economic pressures. Each question has a Likert range from 0 to 4: (0), rarely (1), sometimes (2), often (3), and always (4). The results of this questionnaire are based on the sum of the scores. The total score obtained by caregivers shows the amount of stress and the psychological burden they have endured in an estimated range between 0 and 88. A higher score indicates a higher burden of disease. The severity of the disease burden is classified into four groups:
0-20: Little or no burden
21-40: Mild to moderate burden
41-60: Moderate-to-severe burden
61-88: Severe burden
The reliability and validity of the ZBI Interview have been acceptable according to previous studies. Also, the Persian version of the ZBI Interview has acceptable reliability according to internal consistency (Cronbach’s alpha 0.77) and test-retest (coefficient 0.78) (17,18).
Statistical analysis
Statistical analysis was performed in SPSS version 22. Descriptive statistics (frequency, mean, and standard deviation) were calculated, and an independent t-test was used to compare variable means. Pearson’s Chi-square test (two-tailed) was also utilized to assess the correlations between variables. The multivariate logistic regression model was used to determine the relationship between the psychological burden of care and the factors related to the child and the family. A P-value of less than 0.05 was considered statistically significant.
Ethical considerations
The present study was approved by the ethics committee of Tehran University of Medical Sciences (IR. Tums. IKh.Rec.1397.013) and is in accordance with the Declaration Institutional of Helsinki.
Results
In the present study, 79 patients with their caregivers who met the inclusion criteria were included. Seven patients were excluded due to parental dissatisfaction. The response rate was 88%.
All the caregivers in this study were mothers with a mean age of 27.33±4.36 years. 25% of caregivers were illiterate, 15.27% had a low education level (lower than Diploma) and 48.62% had a high education level (upper than Diploma). All caregivers lived in the same house with their spouses and only 21.43% of them were employed and the rest were housewives.
The mean age of the patients was 29.85±33.11 months with a minimum of one month and a maximum of 9 years. The mean age of patients at the time of diagnosis was 1.29±3.22 months and the mean disease duration was 28.56±32 months. The average number of siblings was 1.10 (min: 0, max: 3). The most frequent CHD in our study was Ventricular Septal Defect (VSD) with a prevalence of 20.83%, and the least of them was pulmonary hypertension+VSD and Tricuspid Atresia (TA) with a prevalence of 1.39%. Approximately half of (51.4%) the subjects had surgery (mean age of surgery: 11.40, min: 0.5, max: 72 months). The other participants’ characteristics are presented in table 1.
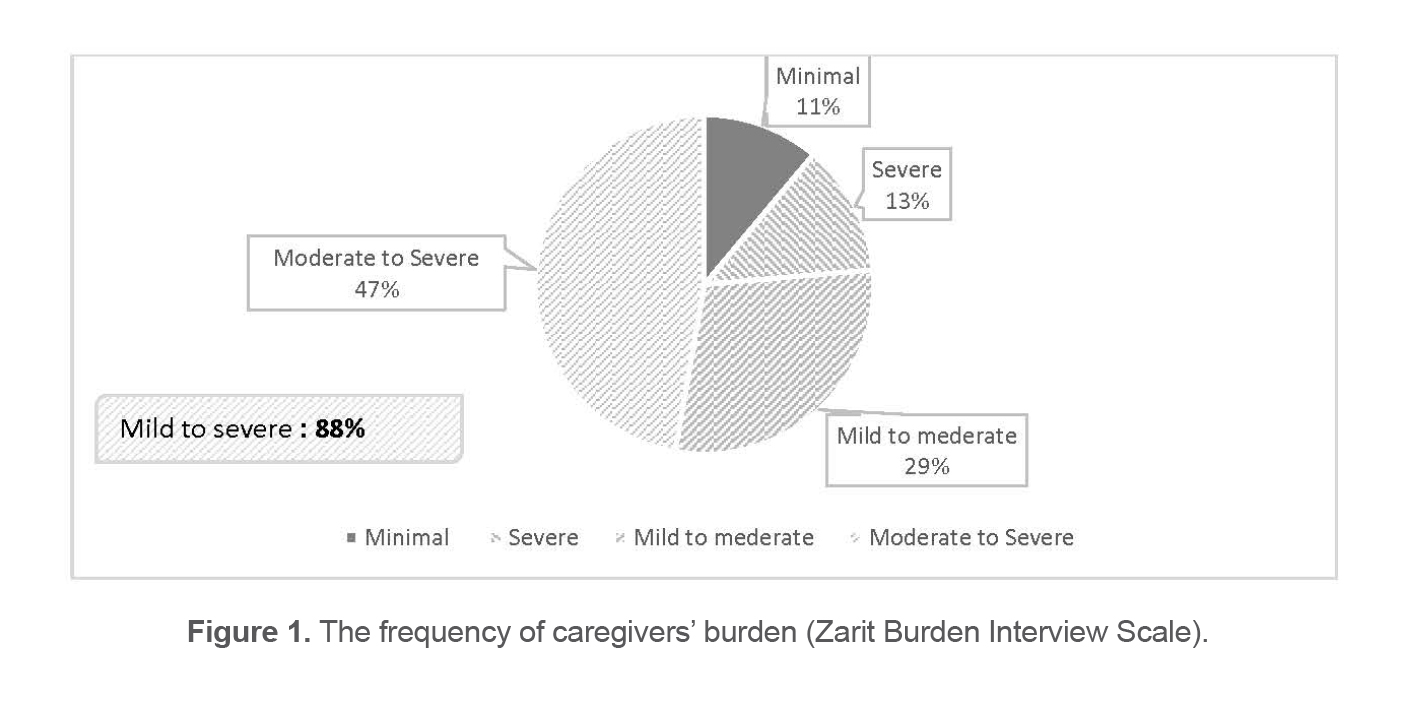
In this study, 8 (11.1%) of caregivers experienced a little or no burden, 9 (12.5%) did severe burden, and 21 (29.2%) experienced mild to moderate burden, while most of them,34 (47.2%), suffered from moderate-to-severe burden. The mean caregiver burden score was 42.78 which is categorized as a moderate-to-severe burden score (Figure 1).
Factors affecting the burden of disease on caregivers such as the age of the patient, age at the time of diagnosis, disease duration, age at the time of surgery, age of caregiver, siblings’ numbers, type of CHD, and level of caregivers’ education were examined. The more the number of siblings, the greater the association with the caregiver’s disease burden (p-value<0.0001). Moreover, the higher level of caregivers’ education had a significant association with the more caregiver’s disease burden (p-value <0.0001).
In order to investigate the predictability of variables (the number of siblings and the level of education of the caregivers), the regression method was used. The only independent variable conversely correlated with the disease burden of caregivers was the caregiver’s educational level. It means that a higher level of education in caregivers of children with CHD was correlated with a lower disease burden (Table 2).
Table 1. The participants characteristics
|
Patients’ age group |
N=72 |
|
0-2 m |
14(20%) |
|
2m-1 year |
26(37.2%) |
|
1-5 years |
15(18.6%) |
|
>5 years |
17(24.2%) |
|
Caregivers’ education level |
|
|
Illiterate |
25% |
|
Low |
15.27% |
|
Intermediate |
41.67% |
|
High |
18.06% |
|
ZBI categoty |
|
|
Minimal |
8(11.2%) |
|
Mild to Moderate |
21(32.8%) |
|
Moderate to Severe |
34(53.12%) |
|
Severe |
9(14.06%) |
Zarit Burden Interview.
Table 2. Analysis of factors affecting the caregivers’ burden
|
Variables |
Significancy |
|
Patents’ age |
0.73 |
|
Age at the time of CHD diagnosis |
0.65 |
|
Age at the time of surgery |
0.54 |
|
Number of siblings |
0.000 |
|
Caregivers’ Age |
0.93 |
|
CHD Type |
0.89 |
|
Caregivers’ Education |
0.000 |
|
Disease duration |
0.42 |
Discussion
In the present study, most caregivers 34(47.2%), suffered from moderate-to-severe burden. All caregivers of children with CHD were biological mothers with a mean age of 27.33±4.36 years and most of them were literate and unemployed. This finding is the same as other studies that showed most caregivers were mothers (15,16,19). Also, according to sociocultural issues, mothers were the main caregiver of children.
At the base of the main purpose of our study, most caregivers (47.2%) suffered from moderate-to-severe burden, and, the mean caregiver’s burden (ZBI score) was in the range of moderate-to-severe disease burden. To the best of our knowledge, no study has assessed the burden of disease in CHD caregivers using the ZBI. However, studies that have examined psychosocial distress, anxiety, depression, and hopelessness in caregivers of CHD patients, have demonstrated a significant prevalence of these problems in caregivers (17).
In similar studies examining the burden of disease on caregivers of other chronic illnesses, most caregivers experienced moderate-to-severe disease burden and the caregivers of chronic illnesses suffered from the burden as much as the burden of caregivers of children and adolescents with Down syndrome and caregivers of adults with psychiatric patients (such as schizophrenia and mood disorders) (20,21). Also, Kobos et al found moderate-to-high disease burden in caregivers of children with type 1 diabetes which was consistent with the perceived suffering by the caregiver of children with CHD in our study (22). It is noteworthy that in a study conducted on caregivers of autistic children, the assessed burden of disease was lower than the burden of disease in caregivers of patients with CHD in this study (23). As discussed before, most chronic psychiatric and non-psychiatric disorders impose a significant burden on their caregivers. The higher disease burden in the caregivers of children with CHD than in caregivers of children with autism can be due to different tools used for the assessment of the burden.
Age of the patient, age at the time of diagnosis, disease duration, age at the time of surgery, age of caregiver, and type of CHD did not have any significant relationship with the burden of caregivers. These findings were the same as the results of a study of diabetic children caregivers’, which indicated that disease-related factors were not associated with disease burden, and that disease burden was more influenced by concerns about disease progression than the disease itself (22). The siblings’ number and level of caregiver’s education had a significant relationship with the caregivers’ psychological burden, but the only independent variable which was conversely correlated with the disease burden of caregivers was the caregiver’s educational level. As shown in previous studies, high educated mothers have experienced a lower disease burden (22). It also seems that the number of siblings affects the economic situation of the family, and this financial burden can lead to an increase in the burden of illness in child caregivers (24). Furthermore, siblings can have a paradoxical effect on the burden of disease so that older siblings can reduce the burden of disease by helping parents, and the younger siblings can increase the burden of the disease by their own need for extra care. In the present study, the sibling number could not predict the burden of the disease. It may be due to the point that we did not consider the age of siblings and the financial status of the family in our study.
The first limitation of our study is that we only included mothers in the study since they were more accessible. It is better to evaluate the disease burden in fathers in future studies. Second, we did not evaluate the socioeconomic status of caregivers. The socioeconomic status of caregivers could influence the disease burden. Third, as previously mentioned, we did not consider the age of siblings. Finally, the study included the children from 0 month to 10 years and they were not divided into different age groups. Given that child care needs are more at a younger age; caregivers’ burden is affected. Fourth, caregivers were not interviewed for detecting the present and past history of psychiatric disorders, so the presence of psychiatric disorders can affect the disease burden.
Further research
The authors recommend further studies that address the impact of disease burden on the mental health of children and their caregivers. For this purpose, other studies could be designed that use semi-structured interviews and psychometric tools to assess the mental health of children with CHD and their caregivers.
Conclusion
CHD is associated with a significant caregivers’ disease burden. Although the disease-related factors were not related to disease burden, the higher caregivers’ education was related to fewer caregivers’ disease burden. Therefore, paying attention to the caregiver’s burden is an important clinical issue.
Funding
This research received no specific grant.
Acknowledgements
The authors have such deep respect for Dr. Azin Kamali’s diligent efforts and how much time she had taken to do this well.
Conflict of Interest
The authors have no competing interests to report.
23.Lerthattasilp T, Charernboon T, Chunsuwan I, Siriumpunkul P. Depression and burden among caregivers of children with autistic spectrum disorder. J Med Assoc Thai 2015 Mar;98 Suppl 2:S45-52. https://pubmed.ncbi.nlm.nih.gov/26211103/