Document Type : Short communication
Abstract
Background: Breast cancer, the most common cancer in women, has a significant challenge in the early diagnosis of medicine. This study aimed to evaluate the diagnostic value of the neutrophil-to-lymphocyte ratio in differentiating benign and malignant breast masses by an economical and straightforward test of Complete Blood Count (CBC).
Methods: This study was a retrospective cross-sectional that was performed on 75 patients with breast masse (40 had benign breast mass and 35 had malignant mass). Data was obtained from the patient’s hospital sheets with health ministry ethics permission. This information was demographic data including CBC, CBC diff, neutrophil/lymphocyte ratio, BMI, and pathologic results of biopsies. Data were analyzed by chi-square, Mann-Whitney, fisher’s exact tests, t-test, and ROC maps in SPSS version 16 software.
Results: The diagnostic power of neutrophil-to-lymphocyte ratio in the diagnosis of malignant tumor or benign according to the cut-off point was 1.74, and significant. Sensitivity and specificity were 85.71 and 45%, respectively, and their positive and negative predictive value was also found to be 57.76 and 78.26%, respectively, and the overall accuracy of the test was 64%.
Conclusion: The neutrophil-to-lymphocyte ratio has high sensitivity and low specificity that can help identify positive malignant breast masses. Due to the low specificity, the negative results, however, cannot detect the nature of breast masses with high precision. Therefore, this test is considered a preliminary method that is complementary to other more explicit tests used for the identification of malignant breast masses.
Keywords: Breast cancer, Breast neoplasms, CBC, Neutrophil-to-lymphocyte ratio
Introduction
Breast cancer is the most frequent cancer among women, and the risk of developing it grows as they get older. Breast carcinoma, like other malignancies, may develop because of systemic inflammation. In 1863, Rudolf Carl Virchow characterized the cellular beginnings of cancer for the first time and indicated that lymphoreticular infiltrates mirrored cancer origins at sites of persistent inflammation. Virchow’s concept was confirmed after the investigation, and the resulting links between cancer and inflammation have significant implications for cancer prevention and treatment (1).
The systemic inflammatory response can vary with tumor growth, invasion, angiogenesis, and metastasis (2). These inflammatory responses are used for early diagnosis or as a prognostic marker for different cancers like head and neck and GI. Many inflammatory indicators are elevated in breast cancer patients and hurt survey results (3–5). The incidence and mortality of breast cancer vary a lot depending on where you are in the world. In general, the occurrence is high (greater than 80 per 100,000) in developed parts of the world and low (less than 30 per 100,000) in developing countries, though both are increasing; the range of mortality rates is much lower (approximately 6-23 per 100,000) due to the better survival of breast cancer in (high incidence) developed areas. (4,6) It is expected that the prevalence of cancer in developed countries will have increased by 45 percent by 2040 (5,7). According to Globo cancer in 2018 estimates, Asia accounts for 48.4 percent of cancer incidence and 57.3 percent of cancer mortality (6,8). The developing world (which accounts for 82 percent of the global population) has seen an increase in cancer incidence and death due to population aging, population growth, and rising trends in the prevalence of cancer risk factors (7,9). As a developing country, Iran has been confronted with issues in recent decades, particularly population aging and rising cancer risk factors. Cancer has been indicated as the third major cause of death in Iran after traffic accidents and cardiovascular mortality (8–11). According to regional studies from Iran, various malignancies are on the rise, particularly breast and colorectal cancers. As a result, cancer control programs are high on Iran’s agenda for combating Non-Communicable Diseases (NCDs) (8,10). With increasing breast cancer primal diagnosis is hypercritical for prognosis and survival of breast cancer, therefore non-invasive, non-expensive diagnostic methods are valuable, like hematologic assessment, tumor markers, or sonography (12–15).
Several studies assessed the role of the peripheral blood test as a diagnostic marker in various types of solid cancer, and Neutrophil to Lymphocyte Ratio (NLR) is one of them. However, there is no evidence of the role of this index in breast cancer (15).
Since one characteristic scientific definition for suspicion of a benign or malignant mass of breast is age, some physicians might not appreciate that they can find malignant tumors in younger patients. Therefore, they might not emphasize and meticulously follow up breast mass in younger women. For awareness of physicians and patients, we decided to examine a simple, rapid, and non-expensive investigating way, NLR, to differentiate the benign and malignant mass of breast in our hospitals and prove if it is applicable.
Materials and Methods
In this retrospective cross-sectional study, the patients admitted with breast mass diagnosis were studied at 22 Bahman Hospital in Mashhad in 2020. This study has been conducted with the national health ministry’s ethics permission code, IR.IAU.MSHD.REC.1398.019. Researchers in two groups in a blind manner investigated the patient’s hospital datasheets. One team separately and blindly investigated the microscopic results of breast mass biopsies or excisions. The other team peruses the patient’s hospital sheets for the result of preoperative White Blood cell Count (WBC), cell differentiation, Body Mass Index (BMI), and other demographic and clinical information. According to our hospital policy, all patients must have at least one preoperative cell count with a cell counter, which was performed with a Mindray BC 3000 Plus brand device made in China. BMI was calculated by dividing weight in kilograms by the square of height in meters.
Since in different articles, the NLR is expressed with different cut-offs, in this study, the cut-off is calculated based on the results of samples. Reported by the Roc Curve method (receiver operating characteristic curve or ROC curves are a potent tool as a statistical performance measure in detection/classification theory and hypothesis testing since they allow having all relevant quantities in one plot (10,16). After calculating the NLR and cut-off point, the data was analyzed. Also, during this study, the percentage of sensitivity and specificity were determined and the diagnostic value of NLR was compared to breast mass biopsy. Moreover, in our study, the relationship between BMI and type of breast tumor was examined.
After data collection, all patients with breast mass in the range of 20 to 60 years old with complete hospital files for CBC diff, and breast mass pathology results were included in the study. Patients with a history of steroids, antibiotics, chemotherapy, or immunosuppressive drugs consumption, history of breast operations, symptoms of any infection, history of blood dyscrasia, history of any other cancers, history of autoimmune or inflammatory disease were excluded from the study.
By using SPSS Version 16 software, quantitative data were expressed as mean and standard deviation, and qualitative data were expressed as ratio and percentage. To compare the quantitative variables in the two groups, first, the normality of the data was checked by Smirnov Kolmogorov test, and if data was normal by t-test and if there was no normality, Mann-Whitney test was utilized. Unique formulas were also used to calculate the sensitivity, specificity, positive and negative predictive value of NLR. The significance level of tests was considered less than 0.05.
Results
In this study, 103 patients were admitted to our hospitals in 2020 for breast mass. Due to exclusion criteria, 22 patients have been excluded, and from 81 remaining cases, six of them did not have pathology results on their sheets because the patients took their specimens out of our hospitals for histopathological analysis. Therefore 75 patients were included in the study (40 with benign breast mass and 35 with malignant mass), all of whom were female. The mean age of the subjects was 36.65 years (in the range of 20-60 years).
Our results showed that the hypothesis of normality of data regarding age, neutrophils, and neutrophil to lymphocyte ratio was not normal (p<0.05). However, lymphocyte distribution is normal (p>0.05). In other words, we used qualitative tests inevitably in some statistics. As mentioned, the age distribution is abnormal (p<0.05). According to the results of our study, age in patients with benign breast mass was significantly lower than in patients with malignant mass (30.2 vs. 44.02 years) (p<0.05).
The frequency of BMI greater than 25 in patients with malignant mass was significantly higher than in patients with benign mass (65.7 vs. 25%) (p<0.05) (Table 1). Other characteristic variables like the affected side, the site of breast masses, preoperative diagnostic method, and family history by use of Fishers’ exact test were not significant (>0.05). As can be seen in microscopic diagnosis, the most common findings were fibroadenoma (37.5%) and fibrocystic disease (35%) in patients with benign mass and invasive ductal carcinoma (77.1%) in patients with malignant mass.
Neutrophils in patients with benign breast mass were significantly lower than patients with malignant mass (60.35 vs. 65.82) (p<0.05). Lymphocytes in patients with benign breast mass were significantly higher than patients with malignant mass (32.92 vs. 27.68) (p<0.05). The ratio of neutrophils to lymphocytes in patients with benign breast mass was significantly lower than patients with malignant mass (2.09 vs. 2.8) (p<0.05) (Table 2).
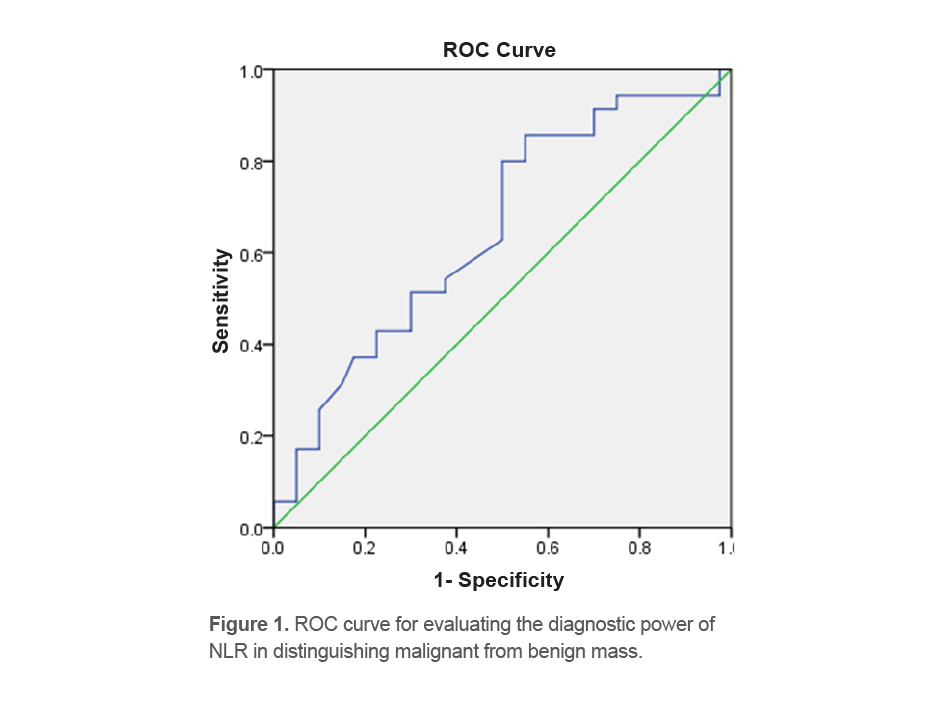
The area under the ROC curve regarding the diagnostic power of NLR in distinguishing malignant from benign mass is equal to 0.64 (p<0.05) (Figure 1). According to this analysis, the best NLR cut-off point in distinguishing malignant from benign mass, which has the highest sensitivity and specificity, is the cut-off point of 1.74 (Table 3).
The NLR diagnostic power in distinguishing malignant from benign mass based on a cut-off point of 1.74, sensitivity and specificity were 85.71 and 45%, respectively, as well as its positive and negative predictive value, 57.69 and 78.26% were obtained, respectively, and the overall accuracy of the test was 64% (Kappa equal to 0.29, p=0.004) (Table 4).
Table 1. Frequency of BMI in patients with benign and malignant breast mass
|
BMI |
Benign |
Malignant |
Total |
Test statistics |
p-value |
|
|
BMI<18 |
Number |
5 |
2 |
7 |
12.55 |
0.002 |
|
Percent |
12.5 % |
5.7% |
9.3% |
|||
|
18<BMI<25 |
Number |
25 |
10 |
35 |
||
|
Percent |
62.5% |
28.6% |
46.7% |
|||
|
BMI>25 |
Number |
10 |
23 |
33 |
||
|
Percent |
25.0% |
65.7% |
44.0% |
|||
|
Total |
Number |
40 |
35 |
75 |
||
|
Percent |
100.0% |
100.0% |
100.0% |
|||
Table 2. Mean and standard deviation of the studied variables in patients with benign and malignant breast mass
|
Variable |
Mass |
Number |
Mean |
Standard deviation |
Test statistics |
p-value |
|
Neutrophil |
Benign |
40 |
60.35 |
9.45 |
-2.54 |
0.011 |
|
Malignant |
35 |
65.82 |
10.48 |
|||
|
Lymphocyte |
Benign |
40 |
32.92 |
9.51 |
2.55 |
0.013 |
|
Malignant |
35 |
27.68 |
8.03 |
|||
|
NLR |
Benign |
40 |
2.09 |
1.00 |
-2.2 |
0.027 |
|
Malignant |
35 |
2.80 |
1.71 |
Table 3. Level of ROC curve regarding the diagnostic power of NLR in distinguishing malignant from benign mass
|
Confidence 95% |
|||||
|
NLR |
Level Below Standard |
Error Curve |
Significance |
Lower Limit |
Upper Limit |
|
0.648 |
0.064 |
0.028 |
0.523 |
0.773 |
|
Table 4. NLR diagnostic power in distinguishing malignant from benign mass based on cut-off point 1.74
|
NLR (cut-off point:1.74) |
||
|
True Positive |
Number |
30 |
|
False Positive |
22 |
|
|
True Negative |
18 |
|
|
False Negative |
5 |
|
|
Sensitivity |
Percent |
85.71 |
|
Specificity |
45 |
|
|
Value Positive Predictive |
57.69 |
|
|
Value Negative Probability |
78.26 |
|
|
Overall accuracy |
64 |
|
|
Positive probability |
1.55 |
|
|
Negative probability |
0.317 |
|
|
Kappa |
0.29 |
|
|
Significance (p) |
0.004 |
|
Discussion
Due to our study, neutrophils in patients with benign breast mass were significantly lower, and Lymphocytes were significantly higher than in patients with malignant mass. The ratio of neutrophils to lymphocytes in patients with benign breast mass was significantly lower than in patients with malignant mass. According to this analysis, the best NLR cut-off point in distinguishing malignant from benign mass, which has the highest sensitivity and specificity, is the cut-off point of 1.74. Sensitivity and specificity were 85.71 and 45%, respectively, as well as its positive and negative predictive value, 57.69 and 78.26% respectively, and the overall accuracy of the test was 64%.
Inflammation is widely established to play a role in developing and progressing several malignancies. Inflammatory cells have a significant role in the growth and progression of several malignancies (11,17,18) the present spatial analysis of breast cancer incidence in Iran in 2009 was conducted using data from the national cancer registry system. The reported incidences of the disease were standardized according to the World Health Organization population and the direct method. Then data was inserted into the GIS software and finally, using the Hot Spot Analysis (Geties-Ord Gi. NLR is a low-cost and straightforward indicator of systemic inflammation. It has been linked to a better prognosis in gastrointestinal tract malignancies, hepatocellular carcinoma, non-small cell carcinoma, and cervical carcinoma (12-14,19-21). In Benign Proliferative Breast Disease (BPBD) and breast cancer that are associated with inflammation, preoperative NLR readings can help clinicians with diagnosis and prognosis.
Many immune cells have infiltrated malignant tissue. Many neutrophils in the tumor microenvironment have been linked to a poor prognosis. Neutrophils accelerate tumor angiogenesis and promote tumor progression and metastasis by secreting cytokines, chemokines, and chemical mediators (1,2). It has been discovered that NLR calculated from systemic blood components predicts the level of tumor-promoting inflammation and that antineoplastic immune cell response has predictive importance (13,20).
Increased NLR was discovered in numerous tumors during a literature search. There have been numerous studies looking for a link between the prognostic role of Neutrophil, Lymphocyte, and NLR in breast cancer metastasis; however, there have been few studies looking at the diagnostic role of NLR differentiation of benign and malignant breast masses. With 15 studies assessing the NLR, overall survival, and disease-free survival, Ethier et al (22) performed a systematic review to explore the prognostic relevance of NLR in breast cancer (disease-free survival). They discovered that a high NLR was linked to worse breast tumor behavior, confirming our findings that a high NLR is linked to worse tumor behavior. Since a higher NLR of 1.74 was linked to more malignancies, and because this test has a high sensitivity (85%), this approach can be utilized to detect positive cases with 85% accuracy. However, it has low power and is ineffective in detecting negative situations.
Noh et al did a retrospective cohort research on 442 breast cancer patients to investigate the benefits of employing the NLR in predicting survival. The findings demonstrated that high levels of NLR (NLR>2.5) were linked to reduced illness-specific survival rates and that higher NLR rates along with negative estrogen receptors, and positive nodal status were linked to a worse disease prognosis. Finally, the study found that patients with higher NLR values before therapy had poorer survival rates than those with lower NLR values (23). The findings of this investigation are consistent with those of ours. NLR was shown to be considerably increased in patients with malignant mass and high sensitivity at the cut-off value of 1.74, which was 2.5 in the Noh et al’s investigation (23).
Okuturlar et al, in a retrospective study, found that the leukocyte, neutrophil, and NLR were higher in the patient group (p values 0.001, 0.0001, and 0.0001, respectively). Logistic regression analysis demonstrated that elevated neutrophils and platelet distribution width (OR: 0.627, 95%CI: 0.508-0.774, p=0.001 and OR: 1.191 95%CI: 1.057-1.342 p=0.003) were independent variables for predicting breast cancer. The cut-off value for the NLR was 2.56 in their study (24). This study was like our study. However, the cut-off value for NLR was higher than our study (1.76).
Ozyalvacli et al did a retrospective cohort study to determine the diagnostic and predictive role of NLR in 120 patients with primary breast cancer and 50 patients with benign primary breast disease. The cut-off rate for NLR was 2.96, and the sensitivity and specificity were 79.7 and 76.2% in breast cancer patients. Finally, they concluded from this study that high NLR values are considered as predictor and differentiator between breast cancer and benign breast mass, and the increase in NLR is used as a predictor of primary cancer invasion (25). Also, Fang et al claimed a higher preoperative NLR in breast cancer patients compared with breast benign disease patients. Therefore, intermediate-to-high NLR levels substantially increased breast cancer risk (26). However, in our study, it was found that the diagnostic power of NLR in distinguishing malignant from benign mass based on the cut-off point of 1.74, sensitivity and specificity were 85.71 and 45%, respectively, and the value of its positive and negative news were equal to 57.69 and 78.26%, respectively. Also, the test’s overall accuracy was 64%, which had a higher sensitivity and lower specificity than the study. This difference may be due to differences in the sample size, differences in patients’ demographic indicators, and differences in inclusion and exclusion criteria.
Tripathi et al concluded that a low NLR value can be related to a greater survival rate in breast cancer patients. They stated that with complete blood count, NLR can be an alternative marker in breast cancer risk (27). In contrast, the NLR in our patients with malignant tumors was significantly greater than in individuals with benign masses. This difference may be due to differences in the sample size, in controlling the effect of confounders, patients’ demographic indicators, inclusion and exclusion criteria, and sampling methods.
Duan et al conducted a review study to assess the diagnostic association of NLR with breast cancer. A total of 21 studies were examined. In patients with breast cancer who underwent surgery, the increase in NLR was significantly associated with less survival (HR=2/45, 95%CI: 1 / 69-3 / 54), survival without disease (HR=1/54, CI: 1 / 28-1 / 87), and increased recurrence (HR=4/05, 95%CI: 1 / 94-8 / 47). Furthermore, ethnicity classification, clinical-stage, neoadjuvant and adjuvant treatment did not affect the strong correlation between elevated NLR before surgery and poor outcome (28). These findings indirectly support our finding that high NLR is higher in patients with malignant mass.
A study by Nakano et al (1) showed a relation between high NLR (cut off more than 2.16) and breast cancer stage. They reported that preoperative NLR might be an independent prognostic factor for survival in Japanese patients with breast cancer. They also claimed that a weakly-positive correlation was observed between BMI and total leukocyte counts. In addition, patients with breast cancer with lower BMI had significantly higher NLR. Although in the first part, their result agrees with our result, in the second part, we found a substantial relationship between BMI and evil cellularity in breast masses.
Gago-Dominguez et al, in a study, aimed at the evaluation of the inflammatory parameters in breast cancer cases in non-Asian women, found that the leukocyte, neutrophil, and NLR were higher in the patient group (p values 0.001, 0.0001, and 0.0001, respectively) compared to normal controls. Logistic regression analysis indicated that elevated neutrophils and platelet distribution width (OR: 0.627, 95%CI: 0.508-0.774, p=0.001 and OR: 1.191 95%CI: 1.057-1.342 p=0.003) were independent variables for predicting breast cancer. The cut-off value for the NLR was 2.56. in their study. They concluded that neutrophil levels and NLR as part of complete blood count might be used as an independent predictor of breast cancer risk (29). This study is aligned with our study for diagnosing malignant breast masses.
In another systemic review by Corbeau et al NLR was found to be an independent prognostic factor for survival in most of the adjuvant treatment studies (75%). However, no significant correlation was found between survival and NLR for early breast cancer patients receiving neoadjuvant chemotherapy, and advanced breast cancer patients. Most studies failed to find a significant correlation between NLR and complete pathological response after neoadjuvant chemotherapy (30). Our study was not in the management field, however, it showed that the diagnostic power of NLR in distinguishing malignant from benign mass based on a cut-off point of 1.74, sensitivity and specificity were 85.71 and 45%, respectively and its positive and negative predictive value were equivalent to 57.69 and 78.26%, respectively, and the total accuracy of the test was equal to 64%. Therefore, this test has high sensitivity but low specificity and helps diagnose positive cases but cannot detect negative cases with high accuracy. However, this result might be nonconclusive due to the small population and needs more investigation with larger groups.
Conclusion
The NLR test in cut-off point 1.74 in our study has a high sensitivity of more than 85% and low specificity that can help identify positive malignant breast mass cases. However, because of the low specificity (45%), the negative test results cannot detect the nature of breast masses with high precision. Therefore, this test is considered a primary method complementary to other more explicit tests used to identify malignant breast masses. This study demonstrated that the diagnostic power of NLR in distinguishing malignant from benign mass based on a cut-off point of 1.74, sensitivity and specificity were 85.71 and 45%, respectively, and its positive and negative predictive values were equivalent to 57.69 and 78.26%, respectively. The total accuracy of the test was equal to 64%. Therefore, this test has high sensitivity and an accepted accuracy value. But low specificity helps diagnose positive cases but cannot detect negative cases with high accuracy. However, this result might be nonconclusive because of the small population and needs more investigation with larger groups.
Study limitations
One of the limitations of our study is the small number of samples.
Acknowledgements
The authors would like to express their profound gratitude to medical personnel in 22 Bahman Hospital.
Conflict of Interest
The authors declare that there is no conflict of interest.
Ethical Statement
This study was approved by the Research Ethics Committees of Islamic Azad University- Mashhad Branch with the code IR.IAU.MSHD.REC.1398.019.
Funding
None.