Document Type : Original article
Abstract
Background: The death and fear of the COVID-19 pandemic has been a major concern in all countries. Estimating the burden of the disease is one of the indicators that estimates the severity of the damage caused by the disease. This study was performed to estimate the burden of years of life lost due to COVID-19 infection and premature death in North Khorasan.
Methods: In this study, all cases of definitive infection (PCR test positive) with COVID-19 from the beginning of the epidemic to April 2021 were included in the study. Disability-Adjusted Life -Years index (DALYs) was used to estimate the burden of the disease.
Results: Since the beginning of the epidemic, 63697 definite cases of the disease have been identified (prevalence equal to 7%) and the total number of years of life lost due to disability and premature death was estimated at 24769 years. This number represents 28.7 years per 100,000 populations, which in women and men, this number was equal to 26.6 and 30.8, respectively.
Conclusion: According to the results of the study, COVID-19 has caused significant loss of years of life, which due to age and concomitant diseases, deaths are more common in the elderly.
Keywords: Adjusted life years, COVID-19, Disability, Mortality, Pandemics, Premature, Prevalence
Introduction
The new coronavirus (Coronavirus 2019), later named COVID-19, emerged in Wuhan, China in December 2019 and spread rapidly around the world (1-3). The spread of the disease was such that on March 11, 2020, it was designated as a global epidemic by the Director-General of the World Health Organization (4). The COVID-19 pandemic is still going on, and it is the biggest public health crisis in the world in a century.
According to the World Health Organization, over 308 million people worldwide have been diagnosed with Corona so far, of which about 5.5 million have died from the disease (4). Iran is also affected by this disease and the first cases were reported in February 2020 from Qom city in the center of the country (5). Recent data from WorldoMeters show that 6.2 million cases and 131000 deaths due to COVID-19 have occurred in the country so far (January 10, 2022)(6).
Evidence shows despite the fact that the mortality rate of this disease in different parts of the world has varied from 1.8 to 1.5 (7), in general it can be stated that it has challenged all countries. It seems that if this epidemic continues with high incidence and mortality, it can reduce life expectancy and consequently increase the burden of disease. According to studies, the Corona epidemic has changed the mortality rankings in some parts of the world. For example, the United States currently ranks death from Corona virus as the third leading cause of death after cancer and cardiovascular disease by 2020 (8,9).
According to the simulation models, in areas with relatively high life expectancy, if the threshold for the prevalence of COVID-19 infection is more than 1 to 2%, this epidemic will break the life expectancy and reduce it. These models show that the high prevalence of infection (50%) can reduce life expectancy from 2 to 8 years in different parts of the world with different life expectancy (10).
Unfortunately, in Iran, reports of new deaths and morbidity show that, despite the recommendations of the World Health Organization to comply with health protocols such as the use of masks, social distancing, avoidance of community attendance and the like, there is still a large-scale challenge (5,11). The generation rate of 0.9 to 4.41 also correctly confirms the progression of the virus in the country (12).
In general, given the extent of the injury, including morbidity, mortality, and decreased life expectancy, COVID-19 appears to be responsible for the largest burden of disease in recent years. However, due to the global burden of diseases, the Disability-Adjusted Life Years (DALY) ratio (an indicator for calculating the burden of disease) for infectious diseases in Iran has decreased from 1990 to 2017, but regarding the current situation, it is predicted that infectious diseases in the near future would take a significant rate of disease burden to themselves (13).
Estimating the burden of COVID-19 can be a good guide for the proper allocation of limited resources and the adoption of appropriate health policies. However, we do not have sufficient and accurate information considering the burden of COVID -19 disease in Iranian society. Therefore, this study was performed to calculate the burden of COVID-19 disease by measuring the index of disability-adjusted life years in northeastern Iran from February, 2019 to the end of April, 2021.
Materials and Methods
The present study was a cross-sectional study that was performed using the information of Coronavirus patients admitted to the COVID-19 registration system of the Ministry of Health from March 2019 to the end of April 2021. All the suspected patients for whom a diagnostic test was recorded were studied. Data from the COVID-19 patient data registration system of the Ministry of Health were used to obtain information on the deceased coronavirus patients.
Disability-Adjusted Life Years (DALY)
The DALY is a measure of the distance between the current state of health and the ideal state of health in which the entire population lives older, free of disease and disability. According to the World Health Organization, a DALY represents a lost year of healthy living. This index consists of two parts: years lost due to premature death and years spent with disability, and the following formula is used to calculate that:
DALY = YLL + YLD
Years lost due to premature death (YLL)
To calculate the YLL component of the DALY index, using the standard life table (standard life table prepared by 2010 GBD), life expectancy at birth was considered 86.02. This standard life table has been the same for men and women (14). The YLL calculation was performed based on the following formula:
YLL = ∑xNxCe (ra) / (β + r) 2 [e- (β + r) (Lx + a) [- (β + r) (Lx + a) -1] - e- (β + r) a [- (β + r) a-1]]
Nx: Number of deaths due to COVID-19
C: Adjustment constant for age weight
r: Discount rate
a: Age of onset of death
Lx: Standard life expectancy at age a
*β: age weight constant (equal to 0.04).
A) Weight for different ages: In the Global Burden of Disease (GBD) study, for a year of healthy living in the early or late years of life, they weighed less than the middle years of life. This choice was based on the results of several studies that indicate a widespread social preference for a healthier year at a younger age compared to childhood or old age, although many researchers disagree with a greater emphasis on youth. The correction coefficient for age weight is 0.1658 (15).
B) Adjustment rate: DALY calculates years of healthy living in the future that are lost due to injury or illness as the adjustment rate. GBD then applies a discount rate of 0.03 to estimate the present value in the years of life lost in the future (16).
Years Lived with Disability (YLD)
For the YLD component of multiplying the number of patient cases by the duration of disability due to the disease and the severity of disability due to COVID 19 disease for the age and sex groups of the subjects, the following formula was used:
YLD = number of cases (∑Ix) * duration of the disability (Lx) * disability weight (DWx) (x is the age and gender category)
A) Number of cases: The information of all people living in North Khorasan province for whom the diagnosis test was registered and according to the care and treatment system of Bojnourd University of Medical Sciences defined as probable or definite, was used.
B) Duration of disability: The duration of disability for COVID 19, according to a study by Mirzaee et al, was 14 days (from infection to recovery or death in 85% of the patients who experienced signs and symptoms for 14 days) (17).
C) Weight of disability: The duration of disability for injuries should be measured and evaluated in numbers. The severity of disabilities is determined by assessing for each disease, a weight ranging from zero (complete health) to one (low health to near death). The meaning of the weight of any disease is that the time spent with a disease is equivalent to how long it is spent in perfect health from the point of view of society. In the present study, the weight of disability was considered 0.14 using the study of Mirzaei et al (17).
To calculate the DALY, the population of North Khorasan province based on the 2016 census of the Statistics Center of Iran was used. The WHO Excel Template and Stata 16 software (Stata Corp. LLC, College Station, United States of America) were used to estimate the burden of COVID-19 disease. The descriptive statistics for quantities and qualities’ variables were mean (standard deviation), and percent (frequency), respectively. p-value lower 0.05 was considered as significance level. The chi-square and T-independent tests examined the relationship between groups of improved and dead patients and demographic variables.
Results
In the present study, from March 2019 to April 2021, a total of 63697 definitive patients with COVID 19 were identified, of whom 1571 (2.5%) lost their lives.
According to the criteria for definitive diagnosis of the disease, the overall prevalence of COVID-19 disease was 7.19 percent, which in women and men was 6.1 and 7.9 percent, respectively. In urban areas (9.3 percent), the overall prevalence of the disease compared to rural areas (3.2%) was tripled. In urban men and women, the prevalence of COVID- 19 was higher in urban men and women than in rural areas.
Out of 62,126 recovered patients, 11,909 (18.7%) had a history of hospitalization due to this disease and the rest were treated on an outpatient basis.
The mean (standard deviation) age of the patients who lost their lives was 68.1 (18.4) years, while the number for those who recovered from the disease was 19.8 (18.4) years, and this difference was significant (p<0.05). The sex distribution of the improved patients showed that 56.8% of these people were men, while for the people who lost their lives due to this disease, 53.9% were men (p<0.05).
Almost 12.1% of the patients who lost their lives had a history of hospitalization in the Intensive Care Unit (ICU), while for those who recovered from this disease, this number was equal to 6.2% and this relationship was statistically significant (p<0.05), as well as 11.5% of people who died from the disease had a history of using a ventilator, compared with 3.9 percent for those who recovered (p<0.05). The majority of recovered patients (79.5%) and 67.1% of those who lost their lives lived in the city (Table 1).
The total burden of COVID disease was 24,769 years (28.7 years per 1,000 people). The number of years lost due to premature death was 24,443 (99.6% of the total burden) and the number of years of life with disability due to COVID 19 was estimated to be 326 (0.4% of the total burden). The overall burden of COVID 19 in urban patients (16396 years) was twice as high as in rural patients (8259 years). Also, years of life with disability in urban patients (254 years) were four times greater than rural patients (65). The years lost due to premature death in patients with 19 years of age corona virus disease (16,143 years) were twice as high as rural patients (8,194 years) (Table 2).
The burden of COVID 19 was higher in men (13,339 years) than in women (11,430). Also, the total burden in urban men (8904 years) and women (7493 years) was twice as high as rural men (4352 years) and women (3907). Men (185 years) had more years of disability than women (141 years). Also, in urban men (148 years) and women (106) compared to rural men (33 years) and women (32 years), the number of years of life with disability was reported. The number of years lost due to premature death from COVID 19 was slightly higher in men (13,145 years) than in women (11,289 years). On the other hand, the number of years lost due to premature death in urban men and women was twice as high as rural areas (Table 2).
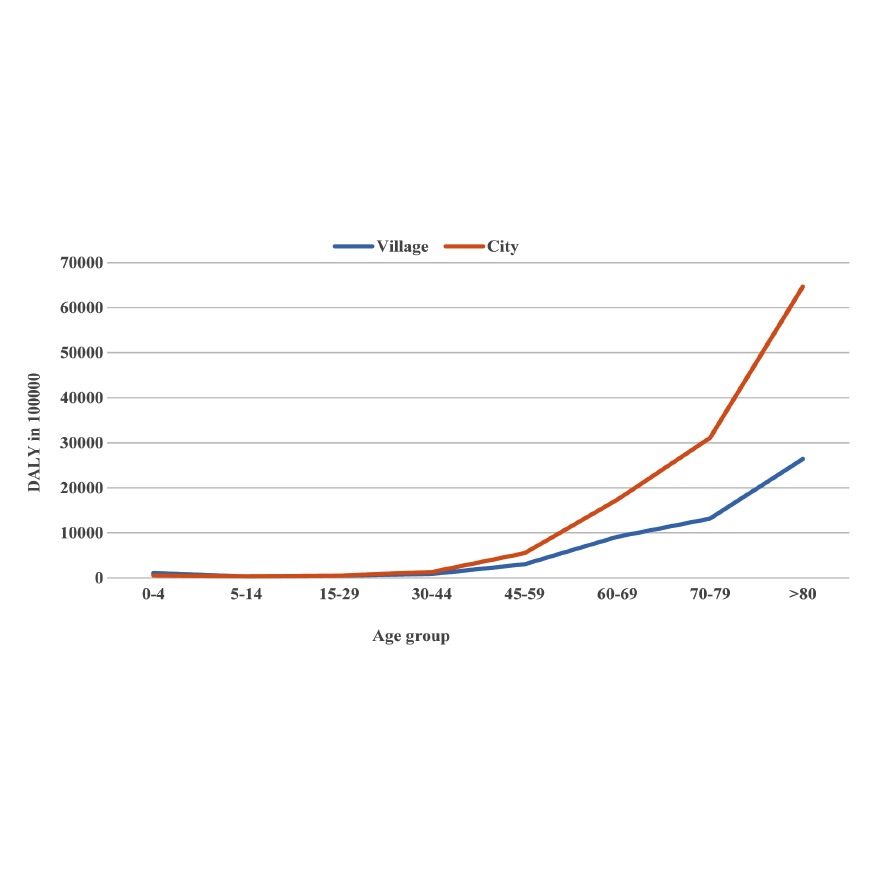
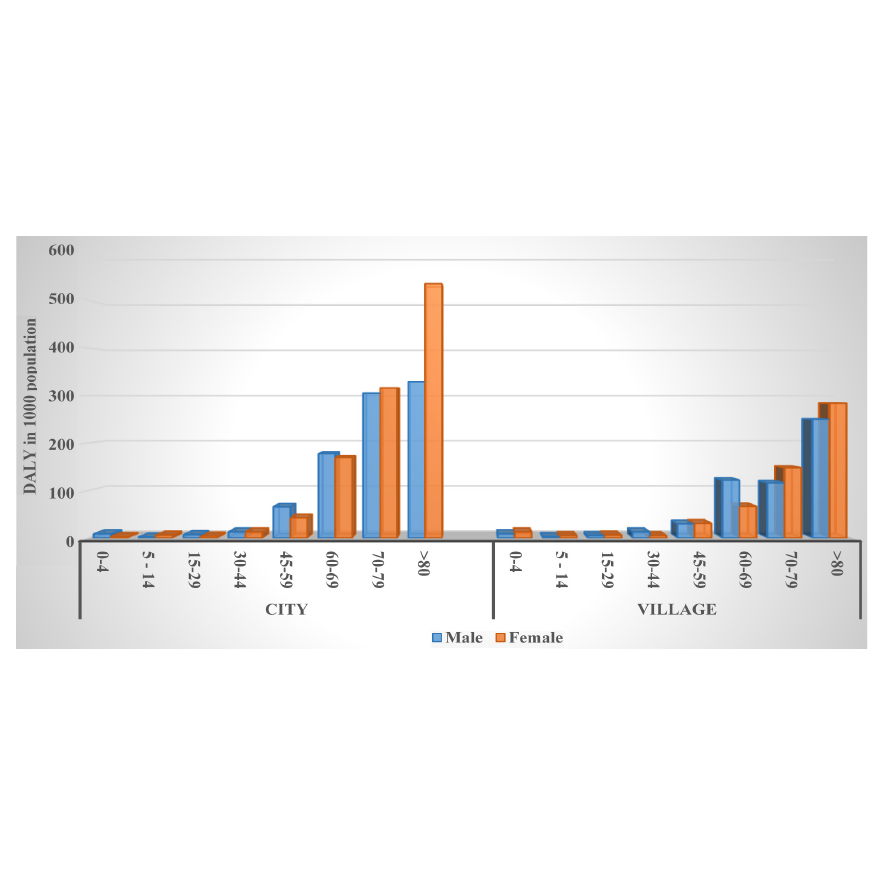
In urban and rural areas, the estimated disease burden is the same until the age of 44, but after the age of 45, COVID 19 disease in urban patients has imposed a greater burden on society than rural patients (Figure 1). In both sexes in urban and rural areas, the disease burden increased after the age of 45. The share of years lost due to premature death in the estimated disease burden was higher than the YLD index (Figure 2, Table 2).
Also, in urban and rural areas, the estimated disease burden in men 45-70 years old was higher than women in the same age group, but after 60 years, the estimated burden in urban women was higher than men in the same age group (Figure 2).
Table 1. Descriptive statistics of some demographic variables of the patients hospitalized with COVID-19 in North Khorasan, February 2020 to April 2021
|
p-value |
Dead patients |
Improved patients |
Variables |
|
|
0.001* |
68.1 (19.5) |
39.8 (18.4) |
Age, Mean (SD) |
|
|
0.03* |
848 (53.9) |
35295 (56.8) |
Male |
Sex, frequency (%) |
|
|
723 (46.1) |
26819 (48.2) |
Female |
|
|
0.001* |
1049 (67.1) |
47669 (79.5) |
City |
Place of residence, frequency (%) |
|
|
516 (32.9) |
12287 (20.5) |
Village |
|
|
0.001* |
282 (19.1) |
674 (6.2) |
Yes |
Hospitalized in ICU, frequency (%) |
|
1193 (80.9) |
10223 (93.8) |
No |
||
|
|
167 (11.5) |
417 (3.9) |
Yes |
Use of ventilator, frequency (%) |
|
0.001* |
1268 (87.6) |
10067 (94.9) |
No |
|
|
|
13 (0.9) |
128 (1.2) |
Unknown |
|
* p<0.05 is significant. SD: Standard Deviation.
Table 2. Incidence rate, YLLs, YLDs, and DALYs for COVID -19 patients by age, sex and place of residence, North Khorasan, February 2020 to April 2021
|
DALYs/ 1000 population |
Total DALYs |
Total YLLs |
Total YLDs |
Case leading to Death |
Incidence rate per100000 population |
Total cases of COVID-19 |
Sex |
Variables |
|||
|
30.8 |
13339 |
13154 |
185 |
848 |
7942 |
24440 |
Male |
Total |
|||
|
26.6 |
11430 |
11289 |
141 |
723 |
6103 |
26212 |
Female |
||||
|
28.7 |
24769 |
24443 |
326 |
1571 |
7027 |
60652 |
Total |
||||
|
36.1 |
8904 |
8756 |
148 |
1049 |
10290 |
27499 |
Male |
City |
Place of residence |
||
|
31.1 |
7493 |
7387 |
106 |
478 |
8206 |
19768 |
Female |
||||
|
33.8 |
16396 |
16143 |
254 |
1049 |
9302 |
47267 |
Total |
||||
|
23 |
4352 |
4319 |
33 |
273 |
3267 |
6149 |
Male |
Village |
|||
|
21 |
3907 |
3875 |
32 |
243 |
3195 |
6006 |
Female |
||||
|
21.8 |
8259 |
8194 |
65 |
516 |
3232 |
12200 |
Total |
||||
|
- |
- |
- |
1.3 |
7 |
542 |
244 |
Male |
0-4 |
Age groups (years) |
Place of residence (City) |
|
|
- |
- |
- |
0.9 |
3 |
803 |
184 |
Female |
||||
|
- |
- |
- |
4.4 |
3 |
2022 |
817 |
Male |
5-14 |
|||
|
- |
- |
- |
4.4 |
7 |
2127 |
823 |
Female |
||||
|
- |
- |
- |
38.5 |
13 |
11436 |
7166 |
Male |
15-29 |
|||
|
- |
- |
- |
24.9 |
8 |
7209 |
4647 |
Female |
||||
|
- |
- |
- |
61.9 |
30 |
18110 |
11521 |
Male |
30-44 |
|||
|
- |
- |
- |
39.8 |
30 |
11855 |
7413 |
Female |
||||
|
- |
- |
- |
24.9 |
106 |
13058 |
4629 |
Male |
45-59 |
|||
|
- |
- |
- |
19.2 |
65 |
10517 |
3569 |
Female |
||||
|
- |
- |
- |
8.5 |
99 |
15961 |
1590 |
Male |
60-69 |
|||
|
- |
- |
- |
8.3 |
105 |
14150 |
1552 |
Female |
||||
|
- |
- |
- |
4.1 |
115 |
15652 |
766 |
Male |
70-79 |
|||
|
- |
- |
- |
4.8 |
124 |
17180 |
892 |
Female |
||||
|
- |
- |
- |
4.1 |
198 |
14683 |
766 |
Male |
>80 |
|||
|
- |
- |
- |
3.7 |
137 |
31019 |
688 |
Female |
||||
|
- |
- |
- |
0.9 |
6 |
824 |
171 |
Male |
0-4 |
Age groups (years) |
Place of residence (Village) |
|
|
- |
- |
- |
0.8 |
8 |
826 |
159 |
Female |
||||
|
- |
- |
- |
1.6 |
3 |
846 |
300 |
Male |
5-14 |
|||
|
- |
- |
- |
2.1 |
5 |
1134 |
384 |
Female |
||||
|
- |
- |
- |
8.9 |
9 |
3223 |
1674 |
Male |
15-29 |
|||
|
- |
- |
- |
6.8 |
9 |
2723 |
1270 |
Female |
||||
|
- |
- |
- |
8.4 |
19 |
4047 |
1572 |
Male |
30-44 |
|||
|
- |
- |
- |
7.7 |
8 |
3468 |
1443 |
Female |
||||
|
- |
- |
- |
5.2 |
33 |
3958 |
966 |
Male |
45-59 |
|||
|
- |
- |
- |
6.1 |
38 |
4227 |
1147 |
Female |
||||
|
- |
- |
- |
3.5 |
66 |
6800 |
648 |
Male |
60-69 |
|||
|
- |
- |
- |
4.1 |
45 |
6541 |
774 |
Female |
||||
|
- |
681 |
678 |
2.4 |
52 |
7750 |
454 |
Male |
70-79 |
|||
|
- |
822 |
820 |
2.7 |
63 |
9163 |
510 |
Female |
||||
|
- |
737 |
734 |
2.2 |
85 |
13902 |
409 |
Male |
>80 |
|||
|
- |
580 |
579 |
1.7 |
67 |
15584 |
319 |
Female |
||||
Discussion
Studies have shown that the overall prevalence of this disease is equal to 7% and this disease has caused a total of 28.7 years of life lost per 100,000 people, which is reported equal to 30.8 and 26.6 for men and women, respectively.
The overall prevalence of this disease seems to be slightly higher than the national average at the time of the study, but due to the nature of the disease, which often occurs asymptomatic or with mild symptoms, this difference can be due to better diagnosis in North Khorasan province. However, a study conducted in Iran based on serological findings on random samples showed that the prevalence of the disease in Iran as of August 21, 2019 was about 14.2%. The mentioned study cannot be compared with our study in terms of prevalence, since our study was based on diagnosed cases, while the study conducted nationwide was serological, which also includes asymptomatic cases (18).
COVID 19 disease was most often because of premature death due to this disease, which was consistent with various studies in Iran (17) (98.4%), Italy (more than 99%) and South Korea (90%)(19,20). The age combination in North Khorasan, Italy and South Korea seems to have caused a slight difference in premature deaths between these regions.
In this study, the total disease burden for men and women per 1000 people was estimated to be 30.8 and 26.6 years, respectively. The sex difference observed in the burden of COVID-19 disease is consistent with the findings of studies conducted throughout Iran (17) and Fars Province (21) as well as studies conducted in South Korea (19) and Italy (20). The higher incidence observed in men than women can be due to gender differences in disease and death. This is because studies have shown that the risk of morbidity and death due to COVID-19 is higher in men than women (22). Another point about the difference in the prevalence of COVID- 19 disease in men and women is that this difference can be due to differences in other diseases. In terms of age distribution of disease burden, the findings of this study showed that age groups 60 years and older in both sexes have imposed more burden on society. This finding is also consistent with the findings of studies conducted in Iran (21), South Korea (19) and Italy (20). The higher incidence of the disease in the age group over 60 years can be considered a higher risk of disease and a higher risk of death in this age group (23,24). Other age groups, such as hypertension, diabetes, respiratory diseases, and cardiovascular disease, which increase the risk of developing and dying from COVID- 19, are also more common in these age groups (22,25).
For men and women, the total burden per 1000 people was estimated to be 30.1 and 26.6 years, respectively. However, according to estimates by the Institute for Health Metrics and Evaluation (IHME), the burden of respiratory infections and tuberculosis in 2017 in Iran was 4.71 DALY per 1000 population (22). Although tuberculosis can cause a much more severe disease, it has a lower transmission power than COVID 19, which has increased the prevalence of this disease in the community, which in turn can increase mortality, especially in individuals in older groups.
Another point to note here is that before the onset of the COVID-19 pandemic, infectious diseases were at a much lower rate of disease burden than non-infectious diseases, for example, according to IHME estimates, respiratory infections and tuberculosis in Iran in 2017 were rated as the most important infectious diseases in the ranking of 11 burden diseases (22), while despite the presence of COVID-19, it seems to be a large shift in the ranking of disease burden in the world and most countries all over the world. Therefore, it seems that new studies should be conducted considering COVID-19 disease to calculate and classify the burden of diseases in countries.
Strengths and limitations
The present study is the first study on the burden of COVID-19 disease in North Khorasan province, therefore it can be used as a basis for comparing the trend of disease burden in this province. Also, the methods and results of this study can be a model for measuring and comparing the results of the disease burden in other provinces. Regarding the weaknesses of this study, it should be noted that this study was performed on patients admitted to hospitals in North Khorasan Province, while a large number of patients with mild symptoms were not hospitalized. Therefore, caution should be exercised in generalizing the results of this disease to the entire population. The second point about the limitations of this study is that, the present study is based on current scientific information, and long-term complications for this disease are not considered, while this disease is new and may have chronic complications as a result of this disease in infected people; these cases have not been identified yet and have not been included in this calculation. In the presence of such complications, the burden of the disease can be greatly affected by these complications.
Conclusion
The findings of this study showed that the burden of COVID-19 disease is higher in men and older age groups, thus health policy makers should pay special attention to at-risk populations, especially age and design and implement programs to reduce morbidity and mortality in the elderly population in addition to taking into account the general population.
Ethical Approval
The draft proposal of this article with the ethics ID IR.NKUMS.REC.1400.031 has been approved by the ethics committee of North Khorasan University of Medical Sciences.
Acknowledgements
This study was financially supported by North Khorasan University of Medical Sciences. The authors thank the Vice Chancellor of Health of North Khorasan University of Medical Sciences for providing the data and Behnaz Neshati for English translation.
Conflict of Interest
The authors declare that there is no conflict of interest.