Document Type : Original article
Abstract
Background: Using an effective method to enhance nurses’ knowledge of ECG interpretation is one of the most essential requirements for nursing managers. Self-directed learning approaches can help to introduce lifelong learning in learners, especially in clinical settings. This study purposed to detect the effect of the implementation of the clinical teammate nurse program on the critical care nurses’ knowledge of ECG interpretation on cardiac arrhythmia.
Methods: A pilot study was performed by a quasi-experimental design with a nonequivalent control group. The participants were 32 critical care nurses divided into two groups: the clinical teammate nurse program and control groups. The data were collected by a knowledge assessment questionnaire that measured nurses’ knowledge of ECG interpretation of cardiac arrhythmia. The nurses’ knowledge was measured three times: initial study, one month, and six months later.
Results: The mean and standard deviation of age of participants was 32.38±7.03 years. There was a significant difference between three scores of repeated measurement of nurses’ knowledge (p<0.001), as the nurses’ knowledge one month after the study was significantly higher than in the initial test six months later. Also, pairwise comparisons showed that nurses in the clinical teammate program had higher knowledge scores than the control group (p<0.001).
Conclusion: The clinical teammate nurse program can be used as an easy and economical way to improve nurses’ knowledge in interpreting ECG. This method can also be an excellent alternative to formal and traditional methods such as lecturing programs in continuing education programs.
Keywords: Clinical competence, Control groups, Education, Con-tinuing, Electrocardiography, Humans, Pilot projects, Research design, Surveys, Questionnaires
Introduction
The Electrocardiogram (ECG) is a highly efficient and non-intrusive instrument utilized in a wide range of biomedical contexts, encompassing the measurement of cardiac frequency, the investigation of the regularity of cardiac pulsations, the identification of cardiac irregularities, the recognition of emotional states, and the authentication of individuals based on their physiological characteristics (1). Nurses should have enough efficacy and knowledge when caring for the patients and diagnosing cardiac disorders are among the most critical issues faced. Usually, nurses have an essential role in providing appropriate care in acute situations (2).
In this regard, an ECG is a necessary diagnostic evaluation tool that every nurse requires a high degree of skill and knowledge to interpret its components (3,4). However, despite the importance of correctly interpreting the ECG, some studies showed gaps in this field in regard to nursing knowledge (5,6). In Dogo et al study, the result showed that 58.3% of nurses did not have sufficient knowledge of ECG interpretation. They concluded that nurses’ ECG interpretation knowledge is insufficient and needs training (7). In Fulbrook et al study, 15-33% of critical care nurses acquired scores lower than 50% in ECG interpretation (8). Also, Keller and Raines showed that nurses’ ability to recognize and identify cardiac arrhythmia was insufficient (9). Jessi et al demonstrated through their study that nurses possess inadequate understanding of ECG rhythm identification and interpretation. One potential resolution entails modifying the education and training associated with ECG diagnosis and morphology.
The authors proposed that nurses should enhance their proficiency through training or internal quality improvement initiatives aimed at detecting abnormalities linked to ECG changes beyond easily discernible rhythms, such as atrial fibrillation or ventricular tachycardia (10). Buluba et al discovered in a separate study that ICU nurses exhibited a low level of knowledge regarding ECG interpretation. Despite participants displaying a positive attitude towards ECG interpretation, a negative attitude persisted. Instead of relying on the opinions of physicians, nurses should embrace ECG interpretation as an integral part of their duties and responsibilities in nursing care (11). The findings of the study conducted by Mohammed Saeed Aljohani also indicated a deficient understanding of electrocardiography in intensive care nurses when it came to ECG interpretation and arrhythmia management. Consequently, it becomes imperative to enhance the knowledge of Special Care Nurses pertaining to ECG, as well as their ability to identify and manage cardiac arrhythmias (12). Therefore, nurses must improve their knowledge about ECG and interpretation of primary ECG rhythms (13).
Various methods such as lecturing, workshop, self-directed learning, web-based learning, and computer program have been used to teach ECG in continuing education courses (14,15). Meanwhile, cooperative and Self-Directed Learning (SDL) are considered methods in which the learner plays an active role in their teaching. There are no formal instructors in this process, and teaching is defined according to learners’ needs (16). Peer-assisted learning is a type of SDL that enhances the self-assessment and learning of learners (17). A review study about strategies of peer learning and its effectiveness indicates that learning was promoted between peers and led to self-development (18). Palsson et al concluded that peer learning was a practical approach to promoting students’ efficacy in clinical practice (19). Park et al expressed that peer interactions can promote knowledge, learning, and self-development among nursing students (18). Also, Cooper et al concluded that the peer-to-peer teaching strategy positively affected nursing students’ learning outcomes (20).
According to mentioned studies, peer-assisted learning was mainly used and investigated in students’ education, and this method has been used less frequently in nursing education programs in clinical settings. In this study, inspired by self-learning principles and peer education, the authors tried to provide a new approach to improve the knowledge of clinical nurses. In the clinical nurse approach, one of the nurses working in a clinical setting was selected among other nurses. Then, after passing a training course, this nurse starts training other clinical nurses in that setting. So, in this study, the efficacy of the clinical teammate approach on the critical care nurses’ knowledge of ECG interpretation of cardiac arrhythmia was detected.
Materials and Methods
Study design
This study was a pilot study with a quasi-experimental design and a nonequivalent control group that was performed on the nurses of the critical care units of the two referral hospitals of Semnan University of Medical Sciences, Semnan, Iran. Since this study aimed to determine the effectiveness of an educational approach on the nurses’ knowledge of ECG interpretation, the researchers had to consider all nurses working in an Intensive Care Unit (ICU) as an intervention group. So, among the six ICUs affiliated with the hospitals of Semnan University of Medical Sciences, two units were randomly selected as the intervention and control groups. Research samples were all of the critical care nurses that worked in these two units, and randomization was not done based on individual nurses in the study groups. There were 16 nurses in each unit. Also, to prevent bias caused by spreading the type of intervention to the control group, each unit was selected from separate hospitals, as the nurses in each unit had no contact with nurses in the other critical care units. The inclusion criteria of the research sample were a bachelor’s degree in nursing and primary membership in the selected ICU. The exclusion criteria were a lack of consent to participate in the research, changing their location of service, and participating in a similar retraining program.
Data collection, instrument, and outcomes
The data were collected by a knowledge assessment questionnaire prepared according to authors clinical experiences and literature review. This questionnaire had 25 questions. It measured nurses’ knowledge of ECG interpretation in cardiac arrhythmia in five domains: basic concepts, supraventricular arrhythmia, ventricular arrhythmia, junctional rhythms, and atrioventricular blocks. The maximum score for each question was five, and the minimum score was zero. The total score of the questionnaire was between 0 and 25, which measured the nurses’ knowledge of ECG interpretation.
The validity of the questionnaire was detected according to face validity (21). In this regard, the questionnaire was given to experts in the field of ECG interpretation to judge the appropriateness of its questions to measure the nurses’ knowledge of ECG interpretation. Then the questionnaire was revised according to their suggestions; the reliability of the questionnaire was calculated by splitting half technique. Finally, the reliability coefficient was estimated at 0.96.
The questionnaires were distributed and collected by a third party separate from the research team among the nurses who were unaware of the intervention and control groups. The questionnaires were distributed three times: at the beginning of the study before applying the clinical teammate nurse approach (as pre-test), one month (as post-test 1), and six months later (as post-test 2).
Interventions and comparison groups
At first, the nurses’ knowledge of ECG interpretation levels was measured in the two groups as a pre-test. Then, one of the nurses in the intervention group who acquired a better score than others was selected as a clinical teammate nurse. The clinical teammate nurse received additional training on ECG interpretation. Then, after coordination and approval from the hospital’s nursing officials, she was responsible for training the ICU nurses in the field of ECG interpretation. Inspired by peer training, in this approach, the clinical teammate nurse, while presenting in various work shifts in the critical care unit, evaluated the training needs of nurses about ECG interpretation and helped to increase their learning with the necessary training. The clinical teammate nurse used formal and informal training methods to train her colleagues.
In the intervention group, the presence of the clinical teammate nurse was planned in such a way that she was shifted equally with each of the nurses in the unit. Then for one month, she set up eight 45-minute formal sessions in face-to-face training with each nurse in the unit on the principles of ECG interpretation for cardiac arrhythmias. The training session time was immediately after completing the nurses’ shift. Also, the clinical teammate nurse was present in the various shift works and answered the nurses’ questions about ECG interpretation of cardiac arrhythmia. Nurses belonging to the control group were also employed within the ICU. However, it should be noted that these nurses had no interaction or communication with their counterparts in the intervention group, as they were specifically chosen from a separate medical facility. In the control group, nurses were not under any training programs and were asked to learn the principles of ECG interpretation of cardiac arrhythmia individually for one month.
They could freely choose any educational materials and references. After one month, the nurses’ knowledge on ECG interpretation of cardiac arrhythmia was again measured in the two groups as a post-test 1. Also, nurses’ knowledge was acquired after six months to evaluate the retention rate and memorization of educational materials as a post-test 2. Therefore, no further or additional training was considered for the two groups during this period.
Statistics and data analysis
Data analysis was performed by SPSS version 23 software for windows. The following statistical tests were used at a 5% significance level. The Kolmogorov-Smirnov test was used to detect normality of the data. The Chi-square test was used for descriptive variables. According to the normality of data, the T-test or U Mann-Whitney test was used to compare means of the study groups. Also, a mixed-design analysis of variance (ANOVA) was performed for more accurate results.
Ethical considerations
The research ethics committee approved this study at University of Medical Sciences (approval ID:IR. SEMUMS.REC.1391.416). Additionally, informed consent was obtained from all participants. The purpose of the study was explained to each patient. It was explained to the nurses that their participation in the study was voluntary, and they could withdraw from the study whenever they wished.
Results
Data analysis showed that 4 (12.5%) of the nurses were male and 28 (87.5%) were female. The age of the subjects ranged from 22 and 50 years (with a mean of 32.38±7.03 yr.). Also, nurses’ work experience in ICU was less than one year to 15 years (with a mean: 3.34±3.67). There were no significant differences in subjects’ demographic data among the two groups.
The Repeated measure analysis showed a significant difference in nurses’ knowledge measurement scores among the two groups (Table 1), as pairwise comparisons showed that nurses in the clinical teammate program had higher knowledge scores than the control group (Table 2).
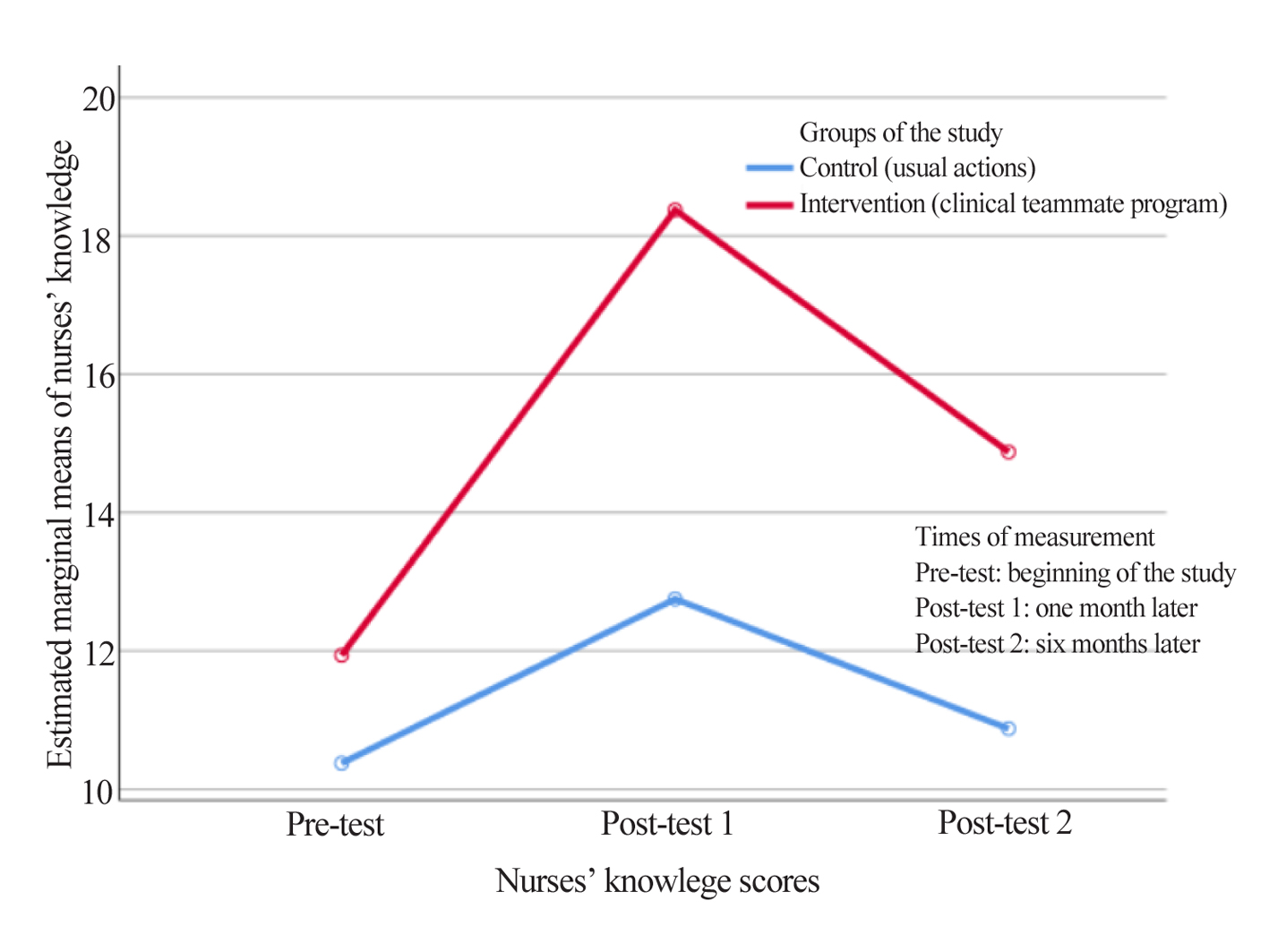
The nurses’ knowledge one month after the study (15.56±4.35) was significantly higher than at the beginning of the intervention (11.16±3.57, P<0.001) and six months later (12.88±4.57, p=0.012) (Figure 1).
There was no significant difference between nurses’ knowledge between the initial test and six months later (p=0.139).
Comparing nurses’ knowledge between two groups of three times measurements showed that the nurses’ knowledge at the beginning of the study did not do not have any significant difference among the groups in the initial test. Then, one month after the initial test and the intervention/ routine actions, the nurses in the clinical teammate approach group acquired higher scores than the control group (Table 3).
Table 1. Repeated measure analysis of nurses’ knowledge scores according to the two groups
|
Source |
Sum of squares |
df |
Mean square |
F |
p-value |
|
Nurses’ knowledge scores |
315.646 |
2 |
157.823 |
14.902 |
<0.001* |
|
Groups of study |
333.760 |
1 |
333.760 |
16.81 |
<0.001* |
|
Interaction effect of nurses’ knowledge * groups |
66.896 |
2 |
33.448 |
3.158 |
0.051 |
* Mauchly’s test of Sphericity is assumed.
Table 2. Pairwise comparisons of nurses’ knowledge in the two groups of study based on estimated marginal means
|
Groups of study (mean) |
Mean difference |
p-value * |
95% confidence interval for the difference |
|||
|
Mean |
Standard error |
Lower bound |
Upper bound |
|||
|
Clinical teammate nurse program (15.06) |
Control (11.33) |
3.729 |
0.909 |
<0.001 |
1.872 |
5.586 |
*Adjustment for multiple comparisons: Bonferroni.
Table 3. Nurses’ knowledge scores between two groups according to times of the measurements
|
Varibles |
Clinical teammate nurse program |
Control |
Interquartile range (IQR) |
Z value |
p-value |
||
|
Mean rank |
Sum of ranks |
Mean rank
|
Sum of ranks |
||||
|
Initial test (Pre-test) |
18.50 |
296 |
14.50 |
232 |
6 |
-1.21 |
0.225* |
|
After one month (Post-test1) |
22.31 |
357 |
10.69 |
171 |
7 |
-3.52 |
p<0.001* |
|
After six months (Post-test2) |
20.63 (14.88±4.63)$ |
330 |
12.38 (10.88±3.63)$ |
198 |
8 |
-2.71# |
0.011** |
* Mann-Whitney test. $ Mean and standard deviation for t-test. # t value. ** T-test.
Discussion
Improving nurses’ knowledge of the principles of ECG interpretation is an essential priority of critical care nurses’ continuing education programs. In this study, the effect of the clinical teammate nurse program on the nurses’ knowledge and learning of ECG principles was compared.
The study showed that the clinical teammate nurse program effectively taught the principles of ECG interpretation of cardiac arrhythmia. The clinical teammate nurse program as an active teaching approach can be a considerable replacement for traditional methods such as lecturing programs. Sawatsky et al showed that an ACTIVE teaching format (assembling into groups, conveying learning objectives, teaching background information, inquiring through cases and questions, verifying understanding, and explaining answers) improved the internal medicine residents’ knowledge scores more than the standard lecture format. In the ACTIVE teaching method, participants actively participated in their learning (22). Similarly, Jang et al compared the efficacy of the SDL method, such as a web-based ECG program, with a didactic lecture method (2 hr of instruction, twice per week, for four weeks). They concluded that SDL methods such as web-based ECG learning programs were more effective than traditional lecture methods for nursing students in their ability to interpret ECG recording. However, they did not observe a significant difference in terms of learning motivation and satisfaction in learning (23). Mansouri and Lockyer, in a meta-analysis of the effectiveness of continuing education programs, found that the traditional approaches such as lectures and conferences had lower efficacy than multifaceted educational programs such as longitudinal workshops and small interactive groups (24).
However, contrary to this study, some evidence was shown that the SDL programs had similar or lower effects than the lecture program. In Zhang and Hsu’s study, the lectured-base program (in the two 1.5 and 3 hours) and self-learning handbook material were compared to evaluate nurses’ knowledge of ECG interpretation. They found that both methods effectively enhanced nurses’ knowledge (25). Also, in Raupach et al study, ECG interpretation skills of medical students were compared according to the method of teaching: near-peer teaching and traditional lecture. Their study showed that the two teaching formats were equal (26). Mahler et al, in comparing three teaching formats on ECG interpretation scores among medical students, found that the SDL format had a lesser impact on students’ scores than lecture- and workshop-based formats (27). Fent et al concluded there was no difference in ECG interpretation scores between lecture and a novel ECG simulator program (28).
This study’s clinical teammate program was administered as a new approach based on SDL and peer-teaching. The clinical teammate nurse was available as a trainer to other nurses during various work shifts and would address their educational needs on clinical problems and materials. The lecturing programs are usually performed for part of the day, and nurses should leave their clinical ward to participate in a continuing education class. While in the clinical teammate program, nurses do not leave the unit, and in addition to providing patient care, they can receive the necessary training in less-paid hours. The Katsikitis et al study showed that nurses valued ongoing learning, preferred education development programs to occur within working hours. The research conducted by Katsikitis and colleagues demonstrated that nurses placed a high value on continuous learning, expressed a preference for educational development initiatives to take place during working hours, and viewed their work environment as conducive to embracing change (29).
Conclusion
The results of the study showed that the clinical teammate nurse program could be used as an easy and economical way to improve nurses’ knowledge on the interpretation of ECG. The clinical nurse is selected from among the unit’s nurses as an educator and can better understand and evaluate the educational needs of other nurses. The clinical teammate nurse is available to other nurses during various work shifts. So, the clinical teammate nurse approach can be an appropriate alternative to formal and traditional methods such as lectures in continuing education programs. However, further studies are suggested to evaluate the effectiveness of this approach in other clinical fields.
Study limitations
Although this study attempted to minimize the relationship between the nurses of the intervention and control groups by considering two wards from two separate hospitals, it was still not possible to completely quarantine the nurses relative to each other. Also, since a whole unit was considered as an intervention or control group, randomly assigning each nurse to the study groups was impossible.
Acknowledgement
We would like to thank the Nursing Care Research Center of Semnan University of Medical Sciences for providing facilities for this work and all nurses that participated in this study and their sincere cooperation. The research ethics committee approved this study at Semnan University of Medical Sciences (approval ID: IR.SEMUMS.REC.1391.416).
Conflict of Interest
The authors declared no conflict of interest.