Document Type : Original article
Abstract
Background: Temporomandibular Disorders (TMDs) are a group of disorders associated with masticatory dysfunction. TMDs are usually diagnosed late which leads to complicated treatments. Early diagnosis and treatment of TMDs are essential.
Methods: A valid and reliable version of Fonseca’s Anamnestic Index (FAI) was prepared in Persian from the English version. It was used to assess TMD in 350 patients. Clinical signs of TMD were also recorded based on examination.
Results: FAI scores showed 161(46%) people had TMD. There was no significant difference between occlusion classes in terms of the frequency of TMD. There was no significant difference between the mean maximum mouth opening and severity of TMD.
Conclusion: In this study the validity and reliability of the FAI in Persian language, as a simple tool for TMD screening in health centers, was confirmed. Based on results, there is a relationship between clinical findings and the severity of TMD by using FAI and it can be used for screening TMD patients.
Keywords: Early diagnosis, Humans, Language, Mouth, Reproducibility of results, Temporomandibular joint disorders
Introduction
Temporomandibular Disorders (TMD) are a group of disorders that are associated with masticatory dysfunction and pain in masticatory muscles or Temporomandibular Joint (TMJ), limitation in mandibular movement and clicking in the joint. (1) Nowadays TMD is a worldwide problem (2). Okeson et al reported that 50-60% of people had one of TMD signs or symptoms but only a small percentage of these symptoms were so severe that made patients to look for treatment (3). The main signs and symptoms of TMD include: pain in masticatory muscles at rest or function, pain in TMJ, TMJ noises, limitation in mouth opening, deviation in mouth opening and joint locking (4-6). Also, there are some associated symptoms like pain in neck and shoulders, tinnitus, vertigo and otalgia (7). TMD has multifactorial etiology that consists of initiator factors (parafunctional habits, trauma), predisposing factors (genetic and systemic factors) and retentive factors (psychological and metabolic factors) (8).
Early diagnosis and treatment of TMD is very important because TMD has a progressive nature and gets worse over time (9). Treatment in early phase of TMD has good prognosis, but in the late phase, complicated and surgical treatments are necessary and the prognosis is questionable. So availability of screening methods for early diagnosis of TMD is very important (10,11).
Fonseca’s Anamnestic Index (FAI) is a simple and inexpensive screening method. This questionnaire was designed in Portuguese for the first time, but was translated and validated in English and several other languages (12). This questionnaire is fulfilled by patients regarding to the presence of TMD signs and symptoms. The score of questionnaire shows the presence of TMD and classifies it according to its severity. The aim of this study was validation of the Persian version of FAI and its association with clinical features of TMD.
Materials and Methods
Study type & ethical code
This was a descriptive analytical study. It was approved by the ethical committee of Shahid Beheshti University of Medical Sciences (Ethical code NO: IR.SBMU.RIDS.REC.1396.583.).
Subjects
All the patients who attended the Department of Oral Medicine, Dental School of Shahid Beheshti University of Medical Sciences for the first time and filled the consent form entered the study. All cases with known psychological disorders, history of trauma to TMJ and edentulous patients were excluded. The sample size was calculated 350 based on the following formula. According to previous studies TMD prevalence was considered 35% in population (11,13,14).
Method of study
Demographic data for every patient including (age, sex, education level), subjective symptoms based on FAI score (0-100) and objective signs (presence of joint noise, maximum opening of the mouth, classification of occlusion, presence of crossbite and deviation, the length and location of toothless space and the mean of the number of missing teeth) based on examination were collected.
Patients were examined by the researchers. To assess joint sounds, a combination of auscultation by means of stethoscope and palpation was used. The patients were asked to open their mouth slowly as wide as possible and then close it slowly. This was repeated by placing an stethoscope on the joint. Click is a popping sound of TMJ and crepitus sounds like walking on dry leaves (15). To check maximum opening of the mouth, the patient was asked to open their mouth as wide as possible painlessly while resting their head against a firm surface in upright position and then the distance between the incisal edges of upper and lower anterior teeth was recorded by a caliper in millimeter (mm) (16).
To check the jaw relations in this research, the examiner stood facing the patient and asked him to close his mouth and put his teeth together, then the patient’s cheek was pushed aside with an examination stick on both sides and the anteroposterior relationship between the maxilla and the mandible was checked to determine the angle’s classification of occlusion (17).
To examine the crossbite, the examiner stood in front of the patient and pushed his cheek away with an examination stick while the jaws are occluded. It was clinically identified, when the lower teeth are in a buccal or labial position regarding the upper teeth. The discrepancy could be unilateral, bilateral, anterior or posterior (18).
Deflection refers to visible deviation to one side at the maximum opening. Deviation is defined as visible left or right movement during opening that returns to the midline before or near the maximum opening. Since observational examination by an expert clinician is an accepted clinical tool for checking deflection and deviation, the examiner stood directly in front of the patients and asked them to open their mouths slowly. Then any deviation or deflection from the straight line was recorded (19,20). To assess the relation between the number of missing teeth and TMD the spaces with tooth loss were categorized as it is considered for the fixed partial denture. To assess the relation between the number of missing teeth and TMD the spaces with tooth loss were categorized as it is considered for the fixed partial denture as following:
The short span (up to 3 teeth), long span (more than 3 teeth) and mixed toothless space (short and long span in different locations (21).
Fonseca’s Anamnestic Index (FAI)
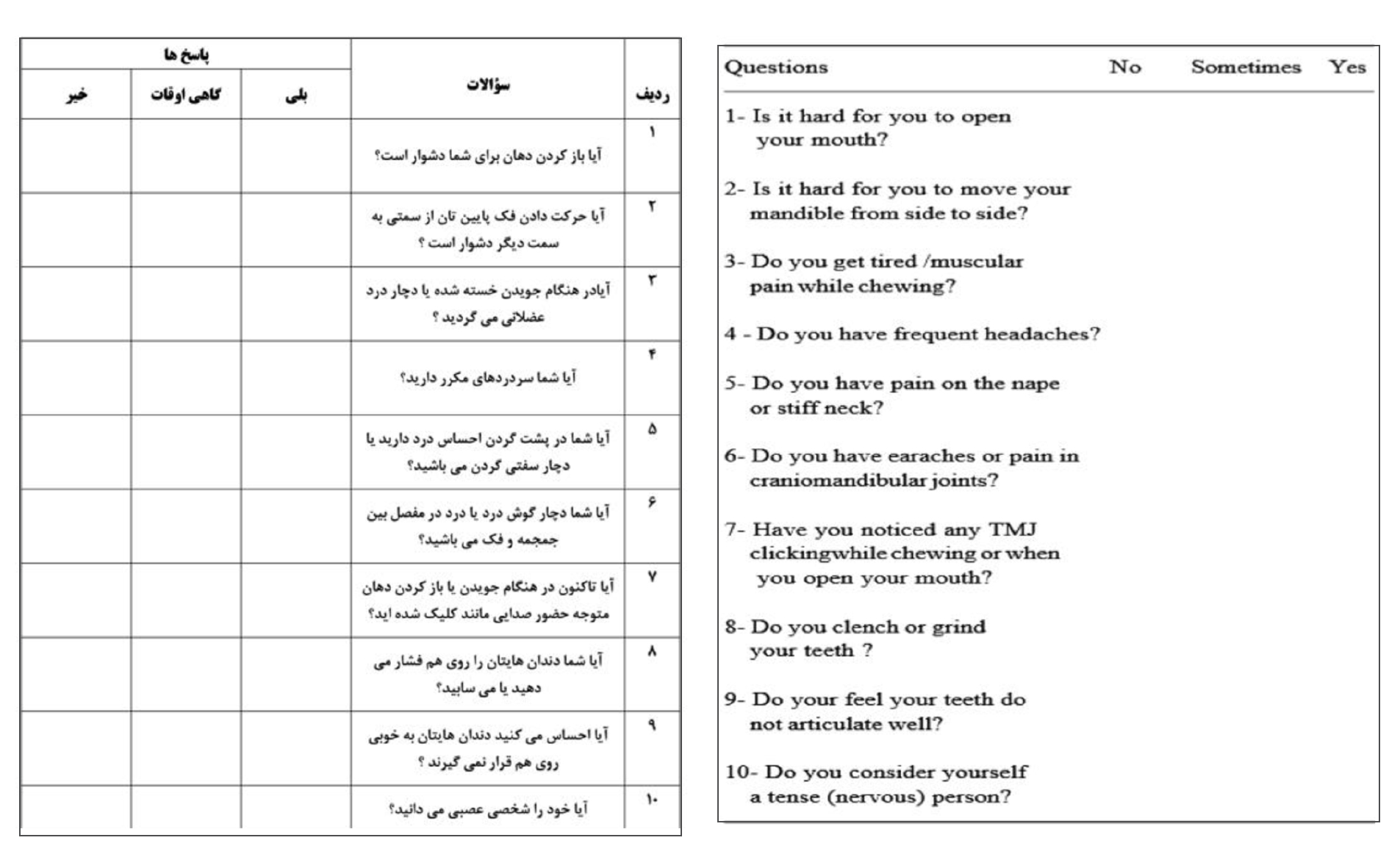
FAI consists of 10 questions. For each question, one of the three: yes (10 score), sometimes (5 score) and no (0 score) answers can be chosen. Sum of the scores classifies patients as: 70-100 as severe TMD, 45-65 moderate TMD, 20-40 mild TMD and 0-15 without TMD.
The questionnaire was translated from English version to Persian by use of “Translation-Re-translation’’ method. Two oral medicine specialists and one prosthodontist translated it to Persian. Then a final form of translated version was extracted. This version was retranslated to English by a native specialist. The first and the final version of English questionnaire were compared by translators and they agreed on the final Persian version of questionnaire.
In a pilot study 20 samples fulfilled this version and after 1 month they fulfilled the questionnaire again. The reliability and validity of Persian version by was calculated by using the kappa coefficient. Then this valid and reliable questionnaire was used for study (Figure1).
Statistical analysis
SPSS version 23 was used for statistical analysis. For reliability and validity of questionnaire Kappa coefficient, Pearson’s correlation coefficient and CronbBach’s coefficient were used respectively. Kruskal-Wallis test was used to evaluate the relationship between clinical symptoms and severity of TMD. In all tests, p<0.05 was considered significant.
Results
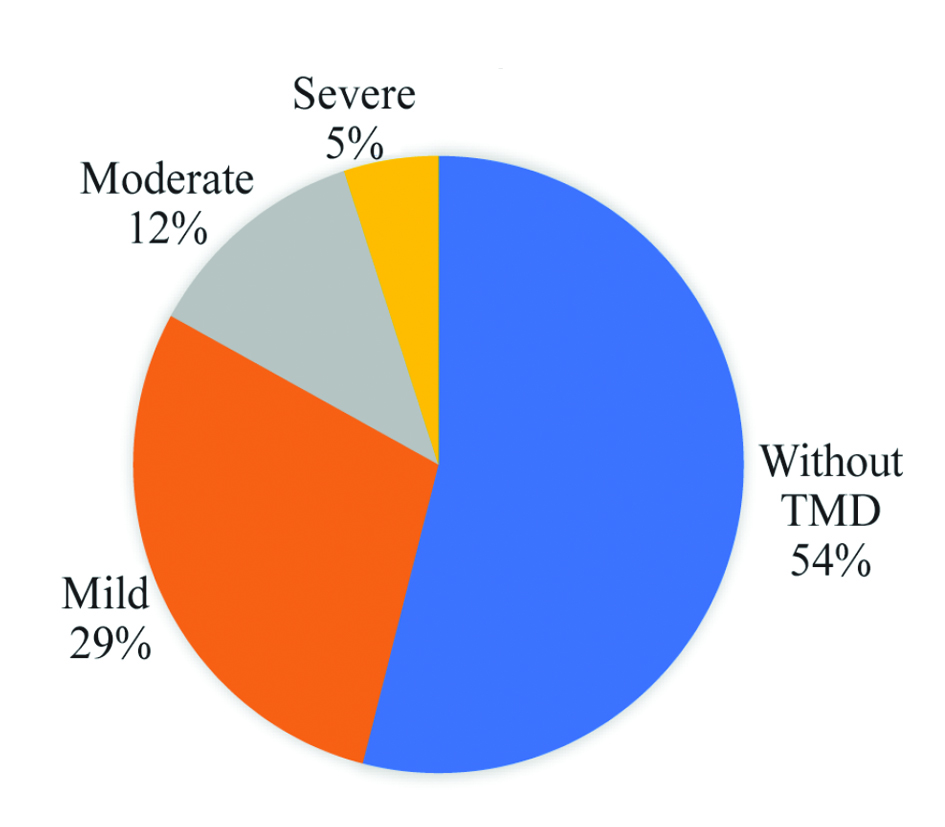
From 350 samples who precipitated in this study 192 (54.8%) were female and 158(45.2%) were male. Mean age of them was 34.29±12.26 yr. Based on Fonseca’s scores 161(46%) samples had TMD: 102(29%) mild, 43(12%) moderate and 16(5%) severe TMD. Figure 2 shows frequency of TMD in the study.
Out of 192 women, 107 (55.7%) and out of 158 men, 54 (34.2%) had TMD. Based on Man-Whitney test there was significant difference between two genders in terms of frequency of TMD (p=0.000). Out of 116 patients with class I occlusion, 47 (40.5%), out of 202 patients with class II occlusion, 99 (49%) and out of 32 patients with class III, (46.9%) had TMD problem. Based on Kruskal-Wallis test there was no significant difference between occlusion classes in term of frequency of TMD (p=0.138).
Out of 17 patients with anterior crossbite, 9 (52.9%) had TMD and out of 27 patients with unilateral posterior crossbite, 16 patients (59.3%) had TMD. Out of 306 people who did not have unilateral or bilateral crossbite, 136 (44.4%) had TMD. Based on Kruskal-Wallis test there was significant difference between crossbite status of samples in term of frequency of TMD (p=0.009).
Table 1 shows Maximal Mouth Opening (MMO) measurement in the present study. The evaluation of the MMO is frequently used as a clinical indicator of the TMJ pathology; therefore MMO was measured with other variables (22). Interestingly the mean of MMO of the patients who entered the study was 42.7±4.65 which was within the normal range reported for both healthy and symptomatic subjects in Iranian population (23). Based on Kruskal-Wallis test there was no significant correlation between mean MMO and severity of TMD (p=0.819).
In this study, out of 136 patients with deviation, 74 patients (54.4%) and among 17 patients with deflection, 9 patients (52.9%) had TMD. Based on Kruskal-Wallis test there was significant difference between samples with deviation with other conditions (deflection or straight mouth opening) in terms of severity of TMD (p=0.002). That means, patients with deviation showed more severe TMD compared to those with deflection or straight mouth opening.
86 (34.8%) patients out of 247 people whose joints did not have clicking and crepitus sounds were diagnosed with TMD. Among 90 people who had joint click, 65(72.2%) and among 9 people who had crepitus, 7 (77.7%) had TMD. Interestingly of 4 people with click and crepitus, 3 people (75%) had TMD. Based on Kruskal-Wallis test there was significant difference between presence of click or crepitus conditions in terms of frequency of TMD (click: p=0.000 and crepitus: p=0.003). In general patients with sounds of click and/or crepitus had more severe TMD in comparison to those without joint sounds.
Out of 197 people who did not have a toothless space, 8 (38.5%) had TMD. Among 116 people with short toothless space (up to 3 teeth) 65 (56%), and among 5 people with long toothless space (more than 3 teeth) 2 people (40%), and among 32 people with mixed toothless space (short and long spaces in different location) 18 people (56.3%) had TMD. Based on Kruskal-Wallis test there was significant difference between short toothless space and no toothless space in terms of frequency of TMD (p=0.002). The mean number of missing teeth among all patients was 2.22± 3.63. Table 2 shows the mean of tooth loss in patients with and without TMD. Based on Kruskal-Wallis test there was a significant relationship between the number of missing teeth and the severity of the TMD (p=0.01). The patients’ answers to each question separately (350 patients: 161 with and 189 without TMD) are shown in table 3.
Table 1. Maximal Mouth Opening (MMO) measurement
|
Temporomandibular disorder severity |
Number |
Mean of maximum opening |
|
Without |
189 |
42.62 |
|
Mild |
102 |
42.79 |
|
Moderate |
43 |
43.02 |
|
Sever |
16 |
42.19 |
|
Total |
250 |
42.70 |
Table 2. Mean of tooth loss in patients with and without TMD
|
Temporomandibular disorder severity |
Number |
Mean of tooth loss±SD |
|
Without |
189(54%) |
1.78±3.46 |
|
Mild |
102(29.14%) |
2.20±3.45 |
|
Moderate |
43(12.29%) |
3.16±4.04 |
|
Severe |
16(4.57%) |
5±4.27 |
|
Total |
350(100%) |
2.22±3.63 |
Table 3. Frequency of patients’ answer with and without TMD to each FAI’s question
|
Questions |
Answers |
Total |
|
||
|
No |
Sometimes |
Yes |
|||
|
Is it hard for you to open your mouth? |
75(46.5%) |
64(39.8) |
22(13.7%) |
161(100%) |
With TMD |
|
255(72.8%) |
73(20.9) |
22(6.3%) |
350(100%) |
Total |
|
|
Is it hard for you to move your mandible from side to side? |
107(66.5%) |
44(27.3%) |
10(6.2%) |
161(100%) |
With TMD |
|
291(83.1%) |
49(14%) |
10(2.9%) |
350(100%) |
Total |
|
|
Do you get tired/muscular pain while chewing? |
61(37.9%) |
71(44.1%) |
29(18%) |
161(100%) |
With TMD |
|
238(68%) |
83(23.7%) |
29(8.3%) |
350(100%) |
Total |
|
|
Do you have frequent headaches? |
48(29.8%) |
67(41.6) |
46(28.6%) |
161(100%) |
With TMD |
|
208(59.4%) |
95(27.2%) |
47(13.4%) |
350(100%) |
Total |
|
|
Do you have pain on the nape or stiff neck? |
67(24.2%) |
55(34.2) |
39(41.6%) |
161(100%) |
With TMD |
|
237(67.7%) |
73(20.9%) |
40(11.4%) |
350(100%) |
Total |
|
|
Do you have earaches or pain in craniomandibular joint? |
115(71.4%) |
29(18%) |
17(10.6%) |
161(100%) |
With TMD |
|
295(84.2%) |
38(10.9) |
17(4.0%) |
350(100%) |
Total |
|
|
Have you noticed any TMJ clicking while chewing or when you open your mouth? |
83(51.6%) |
38(23.6%) |
40(24.8%) |
161(100%) |
With TMD |
|
246(70.3%) |
60(17.1%) |
44(12.6%) |
350(100%) |
Total |
|
|
Do you feel your teeth do not articulate well? |
57(35.4%) |
72(44.7%) |
32(19.9%) |
161(100%) |
With TMD |
|
224(64%) |
91(26%) |
35(10%) |
350(100%) |
Total |
|
|
Do you feel your teeth do not articulate well? |
56(34.8%) |
42(26.1%) |
63(39.1%) |
161(100%) |
With TMD |
|
228(65.1%) |
53(15.2%) |
69(19.7%) |
350(100%) |
Total |
|
|
Do you consider yourself a tense (nerves) person? |
33(20.5%) |
61(37.9%) |
67(41.6%) |
161(100%) |
With TMD |
|
147(42%) |
120(34.3%) |
83(23.7%) |
350(100%) |
Total |
|
Discussion
TMDs are important health issues, but they are usually diagnosed with delay because of unawareness of patients and unexpert clinicians. This results in complicated and surgical treatments. Early diagnosis and treatment of TMD is very crucial. There are several tools to detect and diagnose TMD; of which the Research Diagnostic Criteria for Temporomandibular Disorders (RDC-TMD) is the most common of them. (11) Because of some limitation in use of RDC-TMD (such as time consuming and need the presence of patients) there is an interest toward using other questionnaires. FAI is a simple and reliable tool for screening and diagnosing TMD that is fulfilled by the patients themselves (12). This questionnaire is translated to many languages and in this study it was translated and validated into Persian language. Then the relationship between the results and clinical conditions was evaluated.
Frequency of TMD was 46% in this study. Various studies show different frequencies in terms of TMD. Chaulagain reported that frequency of TMD was 31.9% in clients who referred to Patan dental department (24), but this was reported to be 42, 46.5, 45 and 58.7% by Sousa, Islamian, Mahshid and Alfawza, respectively (25-28). This difference may be due to difference in samples (people or special groups such as dental students) or difference in diagnostic criteria (questionnaire type, with or without clinical examination).
According to the results of the present study, 55.7% of women and 34.2% of men had TMD and there was a significant difference between them in term of TMD frequency (p<0.001). Many studies showed higher frequency of TMD in women and some reported that TMD in women was more severe and needed treatment, but Karthik reported that in his study there was no difference in TMD frequency between men and women (29). A 2007 study by Poveda et al found that the prevalence and severity of TMD in women was four times higher than in men, and the rate of positive response to treatment was up to three times higher in women than in men (10). Differences in the ability to cope with stress, more sensitivity to pain and hormonal differences may be the causes of difference in TMD frequency between two genders (8).
Similar to Lasemi’s study, in the present study there was no significant relationship between age and TMD frequency (30). Meanwhile, Carlsson reported that TMD frequency was higher in young people compared to children (31) and Tecco showed that oral muscular pain was lower in children (6).
In this study there was no relationship between occlusion type and TMD. Manfredini conducted a study to find the relationship between Angel’s classification for molar and canine relationship on both sides and the presence of TMD and stated that there is no such relationship (32). Also, in Poveda’s study, as in the present study, no association was found between TMD and occlusion type (10). But Bilgic in 2017 showed a significant relationship between class 2 and 3 malocclusion and TMD (4).
Based on our results, there was a significant relationship between unilateral posterior crossbite and severity of TMD (p=0.009). This finding is similar to Bilgic and Poveda results (4,10). Other studies have reported asymmetric masticatory muscle activity on sides with and without crossbites following differences in muscle thickness. The resultant incoordination in muscles activity may lead to TMD.
In this study, average of maximum mouth opening was 42.7 mm and there was no relationship between severity of TMD and MMO. Although Karthik stated that the most common symptom of TMD among the 402 students studied was limitation in opening their mouths (29) but based on Bevilaqua-Grossi study limitation in mandibular movements isn’t a reliable criterion for TMD severity (33).
According to the results of the present study, there was a significant relationship between deviation during mouth opening and the severity of TMD (p=0.002). In Son Nguyen’s study, there was also a significant relationship between deviation during mouth opening and TMD. These problems with the mouth opening pattern can be due to muscle misalignment or joint immobility due to an intracapsular defect (34).
In this study, there was a significant relationship between click and crepitus sounds and severity of TMD (p=0.000 and p=0.003, respectively). Bevilaque reported that those who answered positively to the questions of masticatory muscle pain and temporomandibular joint noise, were significantly included in the severe TMD group. (33) Also in Karthik and Son Nguyen studies, there was a significant relationship between joint noise and TMD however Manfredini’s study found no relationship between articular sound and TMD (29,34).
According to the results of the present study in regards to the missing teeth, short edentulous space (one or two teeth) (p=0.005) and bilateral edentulous space (p<0.001) and edentulous space in the middle or the end of the arch (p=0.007) and the posterior edentulous space (p=0.007) had a significant relationship with the severity of TMD. Also, the average number of missing teeth had a significant relationship with the severity of TMD (p=0.010).
Chairunnisa reported that TMD symptoms increase in people who have lost more teeth (35). The role of the posterior teeth is to help reduce the size of food in the act of chewing. The occluding of the posterior teeth reduces the high pressure and also spreads the force on the teeth during mastication, which results in reduction of the pressure on the TMJ; this shows the important role of the posterior teeth.
This study also showed that people who lost posterior teeth in all quadrants were the highest group with TMD (95.7%). According to the Chi-square test, there was a significant relationship between TMD and occlusal support (p<0.05). Weakening of the occlusal system may cause a defect in the chewing function and the neuromuscular pattern of mastication, and it seems to be important in the function of cranio-maxillary complex (36,37).
The absence of several teeth can disrupt the balance in the dental arch and this can put more force on the remaining teeth. Unbalanced stresses imposed on the TMJ structure can affect its function (38). Also in 2009, Wang stated that if a person with posterior tooth loss, loses more posterior teeth in other quadrants, he is more likely to have TMD compared to the situation that he loses one posterior tooth adjacent to the existing toothless space (38). Meanwhile in 2014 Sousa stated that there is no relationship between losing more than 5 teeth or posterior tooth loss and TMD (39).
It seems that more studies are needed to assess the relation between dental features of patients and the frequency and severity of TMD.
Conclusion
In this study the validity and reliability of the FAI in Persian language, as a simple tool for TMD screening in health centers, was confirmed. Based on the results of the present study, there is a relationship between clinical findings and the severity of TMD by using FAI and it can be used for screening TMD patients.
Conflict of Interest
The authors declared no conflict of interest.
1.LeResche L, Saunders K, Von Korff MR, Barlow W, Dworkin SF. Use of exogenous hormones and risk of temporomandibular disorder pain. Pain 1997;69(1-2):153-60. https://pubmed.ncbi.nlm.nih.gov/9060026/
2.Zwiri AM, Al-Omiri MK. Prevalence of temporomandibular joint disorder among North Saudi University students. Cranio 2016;34(3):176-81. https://pubmed.ncbi.nlm.nih.gov/25832332/
4.Bilgiç F, Gelgör İE. Prevalence of temporomandibular dysfunction and its association with malocclusion in children: An epidemiologic study. J Clin Pediatr Dent 2017;41(2):161-5. https://pubmed.ncbi.nlm.nih.gov/28288293/
5.Ryalat S, Baqain ZH, Amin WM, Sawair F, Samara O, Badran DH. Prevalence of temporomandibular joint disorders among students of the University of Jordan. J Clin Med Res 2009;1(3):158-64. https://pubmed.ncbi.nlm.nih.gov/22493650/
6.Tecco S, Nota A, Caruso S, Primozic J, Marzo G, Baldini A, et al. Temporomandibular clinical exploration in Italian adolescents. Cranio 2019;37(2):77-84. https://pubmed.ncbi.nlm.nih.gov/29072541/
7.Manfredini D, Olivo M, Ferronato G, Marchese R, Guarda-Nardini L. Prevalence of tinnitus in patients with different temporomandibular disorders symptoms. Int Tinnitus J 2015;19(2):47-51. https://pubmed.ncbi.nlm.nih.gov/27186932/
8.Motghare V, KuMar J, Kamate S, KuShwaha S, Anand R, Gupta N, et al. Association between harmful oral habits and sign and symptoms of temporomandibular joint disorders among adolescents. J Clin Diagn Res 2015;9(8):ZC45. https://pubmed.ncbi.nlm.nih.gov/26436046/
9.Barone A, Sbordone L, Ramaglia L. Craniomandibular disorders and orthodontic treatment need in children. J Oral Rehabil 1997;24(1):2-7. https://pubmed.ncbi.nlm.nih.gov/9049912/
10.Poveda Roda R, Bagán JV, Díaz Fernández JM, Hernández Bazán S, Jiménez Soriano Y. Review of temporomandibular joint pathology: Part I: Classification, epidemiology and risk factors. Med Oral Patol Oral Cir Bucal 2007;12(4):292-8. https://pubmed.ncbi.nlm.nih.gov/17664915/
11.Dworkin SF. Research diagnostic criteria for temporomandibular disorders: review, criteria, examinations and specifications, critique. J Craniomandib Disord 1992 Fall;6(4):301-55. https://pubmed.ncbi.nlm.nih.gov/1298767/
12.Campos JADB, Carrascosa AC, Bonafé FSS, Maroco J. Severity of temporomandibular disorders in women: validity and reliability of the Fonseca Anamnestic Index. Braz Oral Res 2014;28(1):16-21. https://pubmed.ncbi.nlm.nih.gov/25000601/
13.Lasemi E, Navi F, Basir Shabastari S. Prevalence of Temporomandibular Disorders and it’s Related Factors in Dental School of Azad University of Tehran in 2005. Journal of Mashhad Dental School 2008;32(1):59-64.
14.Valesan LF, Da-Cas CD, Réus JC, Denardin ACS, Garanhani RR, Bonotto D, et al. Prevalence of temporomandibular joint disorders: a systematic review and meta-analysis. Clin Oral Investig 2021 Feb;25(2):441-53. https://pubmed.ncbi.nlm.nih.gov/33409693/
15.Huddleston-Slater JJ, Van Selms MK, Lobbezoo F, Naeije M. The clinical assessment of TMJ sounds by means of auscultation, palpation or both. Journal of Oral Rehabilitation 2002 Sep;29(9):873.
16.Fatima J, Kaul R, Jain P, Saha S, Halder S, Sarkar S. Clinical Measurement of Maximum Mouth Opening in Children of Kolkata and Its Relation with Different Facial Types. J Clin Diagn Res 2016 Aug;10(8):ZC01-5. https://pubmed.ncbi.nlm.nih.gov/27656546/
17.Garbin AJ, Perin PC, Garbin CA, Lolli LF. Malocclusion prevalence and comparison between the Angle classification and the Dental Aesthetic Index in scholars in the interior of São Paulo state-Brazil. Dental Press Journal of Orthodontics 2010;15:94-102.
18.Varghese RM, Keziah VS. A Study Assessing the Prevalence of Crossbite among Patients Reporting for Orthodontic Treatment and its Association with Different Factors. J Res Med Dent Sci 2022;10(5):019-025.
19.Jeon KJ, Kim YH, Ha EG, Choi HS, Ahn HJ, Lee JR, et al. Quantitative analysis of the mouth opening movement of temporomandibular joint disorder patients according to disc position using computer vision: a pilot study. Quant Imaging Med Surg 2022 Mar;12(3):1909-18. https://pubmed.ncbi.nlm.nih.gov/35284273/
20.Danis CG, Mielenz TJ. Reliability of measuring active mandibular excursion using a new tool: the Mandibular Excursiometer. J Orthop Sports Phys Ther 1997 Mar;25(3):213-9. https://pubmed.ncbi.nlm.nih.gov/9048328/
21.Maghrabi AA ,Bedaiwi AM, Hashem AH, Toras MM, Bajukhaif AM ,et al. A Clinical Study Assessing Complications of Different Types of Fixed Prosthesis in Multi Governmental Dental Centres. J Res Med Dent Sci 2021;9(12):37-44.
22.Juca KF, Galdames IC, Guimarães AS. Mandibular condyle position in maximum mouth opening. A magnetic resonance imaging evaluation. Int J Morphol 2009 Sep 1;27(3):867-71.
23.Yaghoubi S, Mosallanezhad Z, Mokhtarinia HR, Philip Gabel C. Sonographic Measurement of Condylar Translation, Joint space and Mouth Opening in Healthy and Subjects with Temporomandibular Joint Disorders. Iranian Rehabilitation Journal 2022 Dec 10;20(4):491-500.
24.Chaulagain R, Maharjan A. Prevalence of Temporomandibular Joint Disorders and its Association with Para Functional Habits in the Patients Attending Tertiary Care Hospital. J Nepal Health Res Counc 2019;17(3):376-81. https://pubmed.ncbi.nlm.nih.gov/31735935/
25.Sousa D, Belindro P, Sousa R, Paulo Sousa J, Pereira Â. Symptoms of temporomandibular joint disorders in university students–a correlational study. Annals of Medicine 2019;51(Sup1):227
26.Esmailian L, Alizadehagha F. [Epidemiology of temporomandibular joint disorders in dental students at Shahid Beheshti university 1999]. Journal of Dental School Shahid Beheshti University of Medical Sciences 2001;19(1):9-15. Persian
27.Alfawzan AA. An Assessment of the Prevalence and Severity of Temporomandibular Disorders among Undergraduate Dental Students at Qassim University. World J Dent 2020;11(2):134-8.
28.Mahshid m, Ejmali M, Nouri Mahtab, Shalchizade A, Doroudian Ali Akbar. [Prevalence of temporomandibular disorders in clinics and health centers in tehran during summer 2002]. Journal of Dental School Shahid Beheshti University of Medical Sciences 2007;25(2):200-208. Persian
29.Karthik R, Hafila MF, Saravanan C, Vivek N, Priyadarsini P, Ashwath B. Assessing prevalence of temporomandibular disorders among university students: a questionnaire study. J Int Soc Prev Community Dent 2017;7(Suppl 1):S24-S29. https://pubmed.ncbi.nlm.nih.gov/28713764/
30.Eshagh L, Fina Navi, Samira Basir SH. [Prevalence of Temporomandibular Disorders and it’s Related Factors in Dental School of Azad University of Tehran in 2005]. Journal of Mashhad Dental School 2008;32(1):59-64. Persian.
31.Carlsson GE, Magnusson T. Management of Temporomandibular Disorders in the General Practice. Quintessence; 2000.
32.Manfredini D, Segù M, Arveda N, Lombardo L, Siciliani G, Rossi A, et al. Temporomandibular joint disorders in patients with different facial morphology. A systematic review of the literature. J Oral Maxillofac Surg 2016;74(1):29-46. https://pubmed.ncbi.nlm.nih.gov/26255097/
33.Bevilaqua-Grossi D, Chaves TC, De Oliveira AS, Monteiro-Pedro V. Anamnestic index severity and signs and symptoms of TMD. Cranio 2006;24(2):112-8. https://pubmed.ncbi.nlm.nih.gov/16711273/
34.Nguyen MS, Jagomägi T, Nguyen T, Saag M, Voog-Oras Ü. Symptoms and signs of temporomandibular disorders among elderly Vietnamese. Proceedings of Singapore Healthcare 2017;26(4):211-6.
35.Chairunnisa R, Sihombing RJ, editors. The Association between Number of Tooth Loss, Tooth Loss Quadrants, and Occlusal Support with Temporomandibular Disorders in Partially Edentulous Patients. International Dental Conference of Sumatera Utara 2017 (IDCSU 2017); 2018: Atlantis Press.
2005;7(3):77-80. 2005;7(3):77-80. https://pubmed.ncbi.nlm.nih.gov/16340271/
38.Wang M, Xue F, He J, Chen J, Chen C, Raustia A. Missing posterior teeth and risk of temporomandibular disorders. J Dent Res 2009;88(10):942-5. https://pubmed.ncbi.nlm.nih.gov/19783804/
39.Sousa STd, Mello VVCd, Magalhaes BG, Morais MPLdA, Vasconcelos MMVB, Junior AdFC, et al. The role of occlusal factors on the occurrence of temporomandibular disorders. Cranio 2015;33(3):211-6. https://pubmed.ncbi.nlm.nih.gov/25027731/