Document Type : Original article
Abstract
Background: Stunting is a significant public health concern in Indonesia. It represents a form of chronic malnutrition that manifests not only as a short stature for one’s age, but also as a profound challenge affecting children’s physical and cognitive development. This study aims to provide more research basis for the government to formulate stunting policies by exploring the ecological factors associated with stunting, consistent with the goal of reducing stunting according to Sustainable Development Goals (SDGs) targets by 2030.
Methods: Data were collected on stunting and ecological factors from 34 provinces in Indonesia from 2015-18, sourced from Statistics Indonesia and the Ministry of Health. A framework of ecological factors that influence stunting, consisting of health, socioeconomic status, and the environment was developed. A panel data model to test the influence of each ecological factor on stunting was created.
Results: Among the 27 independent variables of health, economic status, and environment, the results of this study show that malnutrition, diarrhea, dependency ratio, and hygiene significantly affect the risk of stunting. Meanwhile, antenatal care, nurses, and sanitation have an effect on reducing the risk of stunting.
Conclusion: To achieve the SDGs targets associated with malnutrition by 2030, addressing stunting in Indonesia requires a comprehensive and multisectoral approach that addresses the fundamental causes of stunting, including health, socioeconomic status, and environmental factors. Addressing stunting is crucial for Indonesia, not only to improve the health and well-being of its children, but also for the long-term benefits of enhancing educational outcomes and economic productivity.
Keywords: Economic status, Indonesia, Public health, Sustainable development
Introduction
The global agenda of the Sustainable Development Goals (SDGs) includes a collective objective of reducing the prevalence of stunting by 2030 (1). Stunting, as defined by the World Health Organization (WHO), refers to a condition when the length or height of a person’s body is less than or equal to two standard deviations compared to their age, which is attributed to malnutrition and illnesses during the initial 1000 days of their existence (2,3). Other factors that can contribute to this phenomenon include advanced age, low birth weight, insufficient exclusive breastfeeding, and inappropriate and poor methods of complementary feeding.
Indonesia, despite its status as the largest economy in Southeast Asia and its ranking of 17th globally, continues to grapple with the issue of malnutrition. According to the World Bank, the nation’s performance in addressing stunting is comparatively inadequate when compared to other middle-income countries (4). It is imperative to acknowledge that the elevated incidence of stunting typically results in diminished cognitive development and learning outcomes among children, hence limiting future generations to only a fraction of their full potential. The government incorporated the objective of decreasing the prevalence of stunting among children aged five and below into the Medium-Term National Development Plan (RPJMN) for the period of 2020-2024, as stated by the Ministry of Health (5).
Individuals who experience stunting typically exhibit short stature syndrome, which is subsequently accompanied with pathological issues, reduced neurocognitive abilities, and an elevated susceptibility to non-communicable diseases during their adult years (6). In addition, individuals in this population are susceptible to the potential transmission of infectious diseases, such as pneumonia and diarrhea, and have a tendency towards diminished academic performance (7). Maternal factors, including lower socioeconomic, low levels of education, poor health conditions, inadequate access to water, sanitation, and hygiene (WASH), and limited access to health facilities, have a significant impact on stunting (8).
Food diversity is indirectly influenced by the biophysical environment, including household food security (9). Biophysical factors, including elevation, rainfall, temperature, humidity, topography, soil type, distance to urban areas, and community access to markets, have been identified as influential factors in determining food security. These factors have been found to have an impact on the occurrence of stunting problems among toddlers (10,11). The phenomenon of climate change has significant implications for environmental dynamics, leading to alterations in both the quantity and quality of food and having an effect on stunting (12). Consequently, these changes have the potential to disrupt food production (13).
Numerous international studies have been conducted to examine the correlation between the prevalence of stunting and the various factors that influence it. The researchers have identified that health, socioeconomic status, and environmental have the potential to impact the prevalence of stunting. However, the generalizability of these findings to the Indonesian context remains uncertain. The aim of this study is to identify ecological factors associated with stunting prevalence using a panel data model. The results of this study will provide valuable insights for evaluating and improving future endeavors aimed at reducing stunting.
Materials and Methods
In this study, several ecological factors affecting the prevalence of stunting were selected and a panel data model was constructed to test the effect of each ecological factor on the prevalence of stunting. The data analysis in this study is based on published data from the Statistics Indonesia and the Ministry of Health covering 34 provinces in Indonesia in 2015-18. The process involved matching published data for the provincial-level prevalence of stunting against health, socioeconomic status, and environmental factors to assess population levels after adjusting for potential confounders. This is because individual-level analysis is impossible. The data obtained from the Statistics Indonesia and the Ministry of Health is anonymized, and the values reported to the public are averaged. It is important to note that all statistical analyses were performed using Stata v17 software.
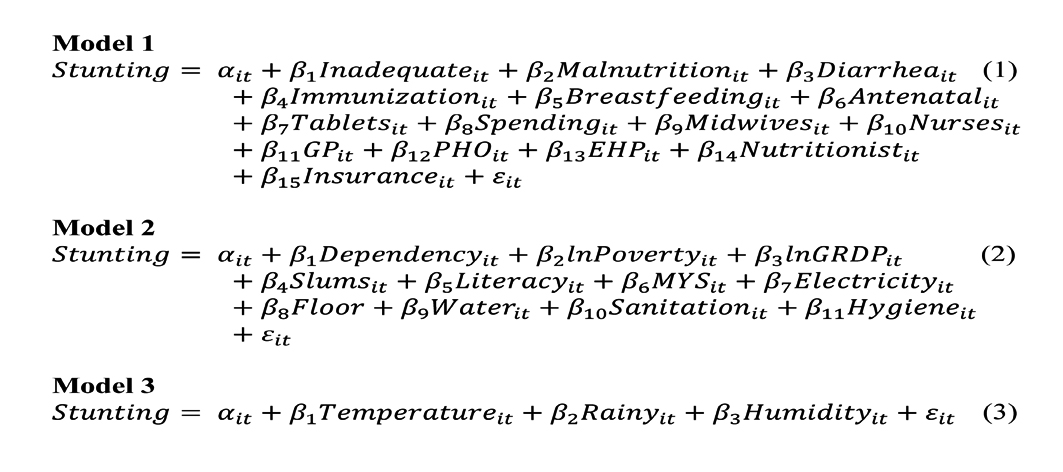
The method used is panel data regression analysis. The panel data regression method combines time series and cross-section. Panel data uses double subscripts (subscripts i and t) in writing. In panel data analysis, there are three estimation model choices: common effect, fixed effect, and random effect. The unit of analysis consists of 34 provinces with one dependent variable and 29 independent variables, including health, socioeconomic status, and environmental. The panel data regression method was used in research on stunting in Indonesia (14). Furthermore, the empirical model used to answer the questions in this study is as follows:
The prevalence of stunting is the dependent variable. The independent variables in Model 1 are health indicators, including: toddler nutrition deficiency (0–23 months); malnutrition deficiency (0–59 months); the percentage of toddlers receiving diarrhea services; the percentage of babies who have received complete basic immunization; the percentage of babies who receive exclusive breastfeeding; the percentage of pregnant women who receive antenatal care according to standards at least four times according to the proposed schedule in each trimester; tablets are iron supplement tablets given to pregnant women; spending is the percentage of budget allocation and realization by the Ministry of Health; the number of midwives; the number of nurses; the number of general practitioners; the number of public health officers; the number of environmental health personnel; the number of nutritionists; the percentage of national health insurance membership.
Model 2 are the independent variables are socioeconomic status, which is measured by the dependency ratio; poverty, which is the percentage of poor people; the growth rate of per capita gross regional domestic product at 2010 constant market prices; the percentage of urban slum households (40% and below); literacy, which is the percentage of women who can read and write; and Mean Years of Schooling (MYS), which is the average number of years women spend in school; the percentage of households that own the lighting source; the floor is the percentage of households that have the largest floor, not land; water is the percentage of households, area type, and source of improved drinking water; sanitation is the percentage of households with access to decent and sustainable sanitation services (40% and below); hygiene is the percentage of the population with access to proper handwashing facilities. While the independent variables in Model 3 are environmental factors, including the average temperature, the average number of rainy days, and the average humidity. The i index refers to provinces that are the research samples, the t index refers to the time period (years), β0 is the intercept, β1 and so on are the estimated slope parameters, and ε is the idiosyncratic error.
In this study, omitted variables may occur due to limited sources and weaknesses in the aggregated data from the provincial level. Differences in health and socioeconomic status indicators and environmental factors can cause differences between provinces.
Results
The data obtained from the Statistics Indonesia for the period of 2015-18 revealed that there was variation in the prevalence of stunting across different provinces. The province of Bengkulu exhibited the lowest prevalence of stunting in 2015, with a rate of 18.1%, whereas East Nusa Tenggara reported the greatest prevalence at 41.2%. Moreover, in 2018, Jakarta had the lowest prevalence of stunting at 17.6%, while East Nusa Tenggara had the greatest prevalence of stunting at 42.7%. The results of the study also indicated that provinces situated in Eastern Indonesia exhibit lower economic development indicators in comparison to other regions characterized by a higher prevalence of stunting. The U5 Children’s Nutritional Status Study (SSGBI) conducted in Indonesia in 2019 revealed a reduction of 3.13% in the prevalence of stunting, dropping from 30.8% in 2018 to 27.67% in 2019. The aforementioned figure surpasses the threshold of 20% as advised by the WHO. It is imperative to acknowledge that the issue of stunting is of significant concern due to its detrimental impact on children’s growth, cognitive capacities, and the competitiveness of the nation.
Indonesian toddlers under the age of five require additional food, which is below the norm. This indicates that stunting is more prevalent than the WHO allows. The sample averages for stunting, health, socioeconomic, and environmental factors from 2015 to 2018 are also presented in table 1. According to the macroeconomic data of this investigation, 29.1% of children in Indonesia are too short for their age on average. East Nusa Tenggara and West Sulawesi have a high prevalence of malnutrition, exceeding 40% according to WHO standards. In Jakarta, the lowest category of stunting prevalence, 17.6%, was observed.
Each province in Indonesia has distinct health indicators, as shown in table 1. Malnutrition remains one of the most pressing issues confronting Indonesia. The average rate of inadequate nutrition was 16.04%, and the average rate of malnutrition was 18.80%. The issue of malnutrition can also affect health and create obstacles for human resource development, bearing in mind that, in the long run, it will impact life quality and productivity. Diarrhea in neonates is one of the causes of stunting. The average percentage of toddlers treated for gastroenteritis was 37.04%. If infants do not receive treatment for diarrhea, they will lose fluids and nutrients. The average percentage of toddlers who have received all fundamental immunizations is 85.01%. Complete immunization of toddlers is essential; in addition to reducing infant mortality, it also reduces the risk of infants developing malnutrition. The average exclusive breastfeeding rate was 57.14%. This indicates that the government’s 80% exclusive lactation coverage goal has not been reached.
The average rate of antenatal care was 79.9%, while the average rate of iron supplementation for expectant women was 70.8%. Pregnant women must receive prenatal care and take iron supplement tablets to prevent malnutrition. The average percentage of Indonesians with health insurance is 73.57%. This demonstrates that enrollment in national health insurance continues to rise. The average allocation and utilization of the de-concentration budget for the Ministry of Health is 76.95%. These funds are crucial for the province, which is working to reduce the prevalence of malnutrition to improve the work environment, family life, and health. There were 5081.71 midwives, 8972.64 public health officers, 534.09 general practitioner nurses, 758.61 environmental health personnel, and 561.66 nutritionists on average. Programs to combat stunting are implemented directly on the ground by health personnel. They are at the forefront of the stunting reduction effort in Indonesia. In addition to preventing stunting, health personnel also provide education and collect data.
The issue of stunting is not solely health-related; it is extremely complex. The prevalence of stunting is also influenced by socioeconomic status. The average rates of dependency and poverty are 46.90 years and 6.02, respectively. This demonstrates that demographic data, particularly the dependency ratio, can be considered when formulating policies to combat stunting. Poverty is also a significant factor in the high prevalence of stunting because the wealthier a family is, the less likely a toddler is to be stunted. The mean Gross Regional Domestic Product (GRDP) per capita is 10.41. This demonstrates that economic development accompanied by an increase in income can reduce the prevalence of stunting. The average percentage of urban shanty households is 10.12%. Residents of urban slums are exposed to poor environmental conditions, including overcrowding, inadequate water and sanitation, and inadequate sewage systems. This places children in the area at high risk for malnutrition-related health issues.
The average female literacy rate is 94.31%, and the average length of education is 8.40 years. Investing in education is one method to break the cycle of problems associated with stunting. The percentages of households with access to electricity and those with the largest non-soil floor are 95.28 and 95.53%, respectively. Access to electricity is essential for existence, as it allows other facilities such as water and sanitation to operate effectively. In addition, the floor area of the home that is not land is essential for the welfare of children. The average percentage of households with access to clean water, sanitation, and hygiene is 61.11, 50.25, and 70.30%, respectively. WASH is one of the fundamental requirements for a wholesome lifestyle. Its function in reducing stunting is crucial because it is closely linked to efforts to prevent disease transmission. The average temperature is 27.43°C, the average number of rainy days is 176.42, and the average humidity is 80.34%. The availability of food in households is affected by environmental factors such as temperature, precipitation, and humidity, thereby increasing the risk of malnutrition and stunting among children.
Table 2 depicts the selection of a model between the Fixed Effect Model (FEM) and the Random Effect Model (REM) to be used for panel data regression analysis of health indicators, socioeconomic status, and environmental factors on the prevalence of stunting in Indonesia. The tests administered were the Chow and Hausman tests. The conclusion of this study’s three models indicates that the REM model is superior because the significance value is greater than (5%). Following the selection of REM, panel data regression analysis is conducted. This analysis was conducted by identifying factors that influenced the reduction of the prevalence of stunting in Indonesia.
In table 3, REM was selected as the optimal model using the Chow test and the Hausman test. In this study, indicators of health, socioeconomic status, and the environment influenced the decrease in stunting prevalence from 2015-18. According to the results of the panel data regression test, only 7 of the 29 independent variables had a significant effect on the prevalence of stunting. Malnutrition, diarrhea, dependency ratio, and sanitation variables have a positive and statistically significant effect on stunting prevalence. The variables of antenatal care, nurses, and sanitation had a negative and statistically significant impact on the prevalence of stunting.
Table 1. Summary statistics
|
Variables |
Unit |
Mean |
Std. Dev. |
Min |
Max |
|
Stunting |
Percentage |
29.1 |
5.66 |
17.60 |
42.7 |
|
Inadequate |
Percentage |
16.04 |
3.99 |
5.73 |
24.50 |
|
Malnutrition |
Percentage |
18.80 |
4.85 |
7.18 |
29.50 |
|
Diarrhea |
Percentage |
37.04 |
15.76 |
4.06 |
96.94 |
|
Immunization |
Percentage |
85.01 |
13.22 |
29.60 |
105.30 |
|
Breastfeeding |
Percentage |
57.14 |
14.02 |
15.22 |
90.79 |
|
Antenatal |
Percentage |
79.96 |
16.73 |
21.00 |
114.37 |
|
Tablets |
Percentage |
70.84 |
18.68 |
24.36 |
99.94 |
|
Insurance |
Percentage |
73.57 |
21.23 |
40.19 |
165.45 |
|
Spending |
Percentage |
76.95 |
16.11 |
29.10 |
98.64 |
|
Midwives |
Person |
5081.71 |
5269.29 |
364.00 |
25140.00 |
|
Nurses |
Person |
8972.64 |
9655.56 |
1086.00 |
52406.00 |
|
GP |
Person |
534.09 |
503.51 |
45.00 |
2074.00 |
|
PHO |
Person |
758.61 |
621.23 |
121.00 |
3156.00 |
|
EHP |
Person |
432.77 |
324.96 |
41.00 |
1460.00 |
|
Nutritionist |
Person |
561.66 |
497.57 |
54.00 |
3023.00 |
|
Dependency |
Year |
46.90 |
4.62 |
37.00 |
57.20 |
|
lnPoverty |
Natural logarithm |
6.02 |
1.10 |
3.71 |
8.47 |
|
lnGRDP |
Natural logarithm |
10.41 |
0.55 |
9.31 |
12.01 |
|
Slums |
Percentage |
10.12 |
5.38 |
2.74 |
28.13 |
|
Literacy |
Percentage |
94.31 |
6.17 |
64.6 |
99.92 |
|
MYS |
Year |
8.40 |
0.93 |
5.40 |
10.75 |
|
Electricity |
Percentage |
95.28 |
8.34 |
50.90 |
100.00 |
|
Floor |
Percentage |
95.53 |
6.05 |
72.07 |
99.95 |
|
Water |
Percentage |
61.11 |
12.27 |
26.91 |
92.38 |
|
Sanitation |
Percentage |
50.25 |
16.16 |
8.68 |
86.06 |
|
Hygiene |
Percentage |
70.30 |
13.93 |
19.63 |
92.78 |
|
Temperature |
°C |
27.43 |
0.94 |
23.33 |
29.75 |
|
Rainy |
Day |
176.42 |
53.25 |
70.00 |
86.90 |
|
Humidity |
Percentage |
80.34 |
4.01 |
65.00 |
304.00 |
Table 2. The result of Chow and Hausman test
|
Model 1 chow test |
|
|
|
|
|
Statistics |
Prob. |
Conclusion |
|
Cross-section chi-square |
131.525916 |
0.0000 |
Fixed effect model |
|
Hausman test |
|
|
|
|
|
Chi-Sq. statistics |
Prob. |
Conclusion |
|
Cross-section random |
16.964335 |
0.3210 |
Random effect model |
|
Model 2 chow test |
|
|
|
|
|
Statistics |
Prob. |
Conclusion |
|
Cross-section chi-square |
109.358234 |
0.0000 |
Fixed effect model |
|
Hausman test |
|
|
|
|
|
Chi-Sq. statistics |
Prob. |
Conclusion |
|
|
10.749424 |
0.4645 |
Random effect model |
|
Model 3 chow test |
|
|
|
|
|
Statistics |
Prob. |
Conclusion |
|
|
176.247638 |
0.0000 |
Fixed effect model |
|
Hausman test |
|
|
|
|
|
Chi-Sq. statistics |
Prob. |
Conclusion |
|
|
1.024744 |
0.7953 |
Random effect model |
Table 3: The estimation result of random effect model
|
Variable |
Model 1 |
Model 2 |
Model 3 |
|
Stunting |
Stunting |
Stunting |
|
|
Inadequate |
0.011533 (0.278719) |
|
|
|
Malnutrition |
0.817064 (0.276456)* |
|
|
|
Diarrhea |
0.093074 (0.043154)** |
|
|
|
Immunization |
0.006904 (0.055696) |
|
|
|
Breastfeeding |
0.028949 (0.029512) |
|
|
|
Antenatal |
-0.091149 (0.050865)*** |
|
|
|
Tablets |
0.008477 (0.030250) |
|
|
|
Insurance |
-0.039970 (0.030061) |
|
|
|
Spending |
-0.083912 (0.073807) |
|
|
|
Midwives |
0.000238 (0.000303) |
|
|
|
Nurses |
-0.000355 (0.000200)*** |
|
|
|
GP |
0.001617 (0.002603) |
|
|
|
PHO |
0.001612 (0.001863) |
|
|
|
EHP |
-0.001055 (0.003848) |
|
|
|
Nutritionist |
0.003480 (0.003273) |
|
|
|
Dependency |
|
0.369386 (0.0400)** |
|
|
lnPoverty |
|
0.015960 (0.770707) |
|
|
lnGRDP |
|
0.166668 (1.707847) |
|
|
Slums |
|
0.195164 (0.118441) |
|
|
Literacy |
|
-0.016142 (0.222357) |
|
|
MYS |
|
-1.505705 (1.305771) |
|
|
Electricity |
|
0.042124 (0.186997) |
|
|
Floor |
|
0.088109 (0.198565) |
|
|
Water |
|
0.119280 (0.074152) |
|
|
Sanitation |
|
-0.237479 (0.071213)* |
|
|
Hygiene |
|
0.144618 (0.037688)* |
|
|
Temperature |
|
|
0.333836 (0.467264) |
|
Humidity |
|
|
0.151992 (0.116525) |
|
Rainy |
|
|
-0.002404 (0.007694) |
|
Observations |
136 |
136 |
136 |
|
R2 |
0.717596 |
0.411046 |
0.017112 |
|
RE provinces |
Yes |
Yes |
Yes |
|
Year RE |
Yes |
Yes |
Yes |
Standard errors in parentheses. *** p<0.01, **p<0.05, *p<0.1.
Discussion
Based on the Indonesian Nutritional Status Survey results, 21.6% of Indonesian toddlers will be stunted in 2022. Thus, almost a quarter of toddlers in Indonesia were stunted that year. However, this percentage has decreased compared to the previous few years. In 2021, the prevalence of stunting in Indonesia was predicted to be 24.4%. Seeing the trend, the prevalence of stunting in Indonesia jumped to 37.2% in 2013 and 30.8% in 2018. As previously mentioned, these numbers have tended to decrease in recent years. A government target also aims to reduce the prevalence of stunting in Indonesia below 14% by 2024 (an annual reduction of 2.7%).
This study was conducted in 34 Indonesian provinces between 2015-18. The numerous effects of health, socioeconomic status, and environmental on the prevalence of stunting are illustrated by the panel data regression results. Indicators of health are compiled into 15 independent variables. Inadequate nutrition has a positive and significant effect on the prevalence of stunting, according to the findings. Previous studies stated that inadequate nutrition had created a “vicious circle” characterized by the nutritional status of toddlers who are susceptible to infection, which in turn causes a decrease in appetite, impaired intestinal absorption, increased catabolism, low immunity, and a decreased response to vaccines (15-17). We argue that malnutrition can cause stunting, but it is not the only cause, and stunting can occur even if a child receives adequate nutrition if other factors are not addressed.
The prevalence of stunting is positively and significantly impacted by malnutrition deficiency (0-59 months) and diarrhea. Malnutrition is a dietary deficiency that can cause growth and development delays. Children who do not receive adequate nutrition, particularly during the first 1,000 days of existence, are more likely to develop stunted growth (18,19). In addition, if infants with diarrhea do not receive immediate medical care, they can lose essential nutrients and become dehydrated, which can lead to stunting (20-24). Both malnutrition and diarrhea can impair children’s immune systems, leaving them more susceptible to infections and other diseases. This can exacerbate the cycle of malnutrition, as sick children are less likely to consume and absorb the nutrients necessary for appropriate growth and development.
Immunization and breastfeeding are essential interventions for protecting infants from infectious diseases and promoting healthy growth and development (25-27). If immunization increases the frequency or severity of infections, it can increase the risk of stunting. Vaccines may not provide adequate protection against certain infections, or children may be exposed to infections not targeted by vaccines. In such circumstances, the child’s immune system may be repeatedly activated, resulting in chronic inflammation and increased nutrient needs. This may contribute to malnutrition and short stature. According to the findings of this study, the coverage of complete basic immunization in infants has a positive but insignificant effect on the prevalence of stunting. These findings contradict the findings, who concluded that immunization is a major risk factor for stunting (25,28,29). It is argued, based on the findings of this study, that complete infant immunization cannot directly address the problem of stunting, as stunting is more closely associated with nutritional status and complex socioeconomic factors. Nonetheless, full immunization in neonates can help prevent infections and diseases that can cause growth retardation in children, and it can help improve the long-term health and nutritional status of infants.
According to the findings of this study, exclusive breastfeeding has a positive but insignificant effect on the prevalence of stunting. This study contradicts the findings that exclusive lactation influences the incidence of stunting. This study found that the percentage of infants 0-6 months old who are exclusively breastfed is still relatively low (25,30). Unfortunately, exclusive breastfeeding provides protection from malnutrition and stunting. Multiple factors, including the coverage of the fourth antenatal care visit, the coverage of deliveries in health facilities, the coverage of early breastfeeding initiation, and the percentage of mothers who smoke, contribute to the low rate of exclusive breastfeeding in Indonesia (31). In addition, lactating mothers frequently face obstacles that prevent them from expressing breast milk or giving their children formula milk. Additionally, many dearest relatives frequently provide foods that children should have avoided and this can influence the prevalence of stunting (32).
The administration of iron tablets to expectant women has significant health benefits, including the prevention of anemia and improvement of fetal health. In spite of this, the findings of this study indicate that giving blood supplement tablets to expectant women has a positive but insignificant effect on the prevalence of stunting. Nutritional interventions, such as administering iron tablets to expectant women, can reduce stunting (33). However, the results of this study contradict this theory.
Healthcare professionals play a crucial role in the intervention and eradication of stunting and are actively engaged in the prevention, education, advocacy, and data collection surrounding stunting (34,35). The findings of this study indicate that health professionals such as midwives, general practitioners, and public health officers have a positive but negligible impact on the prevalence of stunting. Although midwives, general practitioners, and community health workers play a significant role in providing health information and services related to child nutrition and growth, other factors such as access to healthy food, poor sanitation, and socioeconomic factors also contribute to stunting. However, midwives, general practitioners, and community health workers continue to play crucial roles in Indonesian efforts to prevent stunting.
In Indonesia, the prevalence of stunting is influenced by socioeconomic status such as per capita income, poverty, urban slum dwellers, access to electricity, the broadest non-soil floor, and access to clean water. However, the results of this study indicate that the influence of these factors on the prevalence of stunting is only occasionally significant and may differ depending on the circumstances and conditions in each region. This research contradicts the findings of other studies suggest that per capita income can affect access to nutritious food, which in turn can affect the incidence of stunting (36-39). Through inadequate sanitation and environmental factors, poverty, urban slum dwellers, access to electricity, the widest non-soil floor, and access to clean water can affect the prevalence of stunting. However, the effect of these factors on the prevalence of stunting can vary depending on socioeconomic, infrastructure availability, and government policies. Despite the fact that these socioeconomic do not always correlate substantially with the prevalence of stunting, they remain crucial in Indonesia’s efforts to prevent the condition.
It is the public knowledge that access to improved and sustainable water brings health and non-health benefits as it has been well documented in several empirical studies (40,41). However, the results of this study indicate that access to adequate and sustainable drinking water has a positive and insignificant effect on the prevalence of stunting. A study conducted by the Ministry of Health of Indonesia found that seven out of ten households in Indonesia consume drinking water contaminated with Escherichia coli (E. coli), which could indicate poor household sanitation conditions and potentially affect child nutrition and growth (42). It is important to note that access to safe and sustainable drinking water has been shown to have a positive impact on nutrition and health outcomes, including reducing stunting. A study by the Ministry of Health of Indonesia found that access to safe and adequate drinking water in Indonesia reaches an average of 93%, with access to safe drinking water in urban areas reaching 97.6% and 87.1% in rural areas.
However, access to safe drinking water is low, at only 11.9% on average (43). Therefore, while various factors may contribute to the prevalence of stunting in Indonesia, access to safe and sustainable drinking water is still important for reducing the risk of water-borne diseases and improving child nutrition and growth. While the impact of access to safe drinking water on stunting prevalence in Indonesia may not be statistically significant, it still plays an essential role in promoting overall health and well-being.
The Earth’s environment has been gravely damaged by human-caused global warming, with potential consequences that may worsen in the coming decades (44). According to the findings of this study, temperature and humidity have a positive and insignificant effect on the prevalence of stunting. Predicting child stunting based on temperature has significant implications for future child malnutrition attributable to climate change (12).
This study also discovered that insurance, expendi-tures, environmental health personnel, female literacy, female mean years of schooling, and rainy days had a negative and insignificant influence on the prevalence of stunting. Indonesia has instituted several strategies to reduce the prevalence of stunting, including mapping the nutritional status of children at the most granular level, promoting exclusive breastfeeding, and expanding access to clean water and sanitation. In 2021, the Ministry of Health will receive an indicative budget allocation of Rp. 84.3 trillion to combat malnutrition and improve the national health system (45). According to former Minister of Health Nila F. Moeloek, the prevalence of stunting in Indonesia decreased to 27.67% in 2019, a decrease of 10% from 2017, when the country was ranked third in Asia with the highest prevalence of stunting (46). However, the prevalence rate is still above the WHO’s threshold of 20%.
By addressing the underlying causes of malnutrition, environmental health personnel can reduce the prevalence of stunting (34). This can involve a variety of interventions, such as improving access to safe drinking water and sanitation facilities, promoting proper hygiene and sanitation practices, providing nutrition education and counseling to mothers and caregivers, and supporting the implementation of programs designed to increase food security. However, environmental health personnel may not have a significant impact on reducing the prevalence of stunting. Other factors, such as poverty, education, and access to healthcare, play an important role in preventing and reducing stunting.
Female literacy and mean years of schooling can reduce the prevalence of stunting. This is because education, particularly for women, can enhance knowledge and skills regarding nutrition, health, and hygiene, resulting in improved health outcomes for both mothers and children (47,48). A comprehensive and multisectoral approach to addressing the underlying causes of malnutrition is required to mitigate their effects. In the case of Indonesia, additional efforts are required to combat poverty, enhance access to healthcare and sanitation facilities, and promote nutrition and health practices supported by scientific evidence.
Rainfall can enhance access to water and sanitation, thereby reducing the risk of waterborne diseases that contribute to malnutrition and stunting. Additionally, precipitation can promote crop growth, thereby enhancing food security and nutrient accessibility (49). Without a comprehensive strategy addressing the fundamental causes of malnutrition and stunting, their effect may be negligible.
The findings of this study must be interpreted in light of the limitations of comprehensive data and sample size for analyses that continue to use macroeconomic data. This is likely to result in a number of variable indicators of health, socioeconomic status, and the environmental, none of which have a substantial impact on the prevalence of stunting. Despite these limitations, this research can contribute to the advancement of public health and health economics in Indonesia with regard to the causes of the prevalence of stunting.
Conclusion
This study employs macroeconomic panel data from the Central Statistics Agency and the Ministry of Health for 34 provinces in Indonesia from 2015-18 to examine the relationship between indicators of health, socioeconomic status, and the environment and the prevalence of stunting. West Nusa Tenggara, West Sulawesi, South Kalimantan, Gorontalo, and Central Sulawesi were the provinces with the highest prevalence of stunting from 2015-18. Meanwhile, the Jakarta has the lowest prevalence of stunting. Several independent variables, including malnutrition, diarrhea, dependency ratio, and sanitation, had a positive and significant effect on the prevalence of stunting, according to our analysis. In contrast, antenatal care, nurses, and sanitation have a significant and negative impact on the prevalence of stunting.
To achieve the SDGs targets associated with malnutrition by 2030, addressing stunting in Indonesia requires a comprehensive and multisectoral approach that addresses the fundamental causes of stunting, including health, socioeconomic status, and environmental. Addressing stunting is crucial for Indonesia not only to improve the health and well-being of its children but also for the long-term benefits of enhancing educational outcomes and economic productivity. By tackling the root causes of stunting, Indonesia can ensure a healthier, more prosperous future for the next generation. This strategy should involve enhancing access to healthcare, promoting nutrition and health practices supported by scientific evidence, and addressing poverty and other social determinants of health. To reduce the prevalence of stunting in Indonesia, efforts to enhance WASH, and air quality should be prioritized.
Ethical approval
The Institute of Research and Community Services, Universitas Sultan Ageng Tirtayasa, granted ethics approval for this study under the number B/19/UN43.9/KP.06.05/2024.
Acknowledgement
The authors would like to express their sincere gratitude to Statistics Indonesia and the Ministry of Health for providing the essential data for this research and to TULUS and Yura Yunita for their support during the writing process. Furthermore, the authors thank the editor and two anonymous reviewers for their valuable comments on this manuscript.
Conflict of Interest
The authors declare that there are no conflicting financial, professional, or personal interests that could have affected the execution or delivery of the research described in this manuscript.