Document Type : Original article
Abstract
Background: The outbreak of COVID-19 has been associated with various physical and psychological effects. The role of exercise in strengthening the immune system and reducing inflammation has already been proven. Moderate levels of exercise can enhance overall immunity. Exercise can improve intracellular metabolism and increase cell defense activity by improving inflammatory cytokines, immature B cells, and cytotoxic T cells. Therefore, exercise is known as a defense strategy against respiratory infections. Here the role of exercise in improving respiratory function and physical activity in hospitalized patients with COVID-19 was evaluated.
Methods: The present study was performed as a randomized clinical trial on 90 hospitalized patients with COVID-19. Both groups received all routine treatments (medication, invasive or non-invasive ventilation, physiotherapy). Then, in the experimental group, standard exercises were provided to improve the patients’ physical condition and exercise capacity. After two weeks and one month later, all indices were measured again in two groups.
Results: The results of the present study showed that exercise causes significant changes in indicators such as 6-Minute Walk Test (6MWT) (p=0.001), balance score (p=0.02), and Sf1 score (p=0.05) in two time periods before and after rehabilitation in two groups.
Conclusion: Performing standard and defined exercise exercises for patients with the new coronavirus improves the physical activity and respiratory function of patients.
Keywords: COVID-19, Physical activity, Rehabilitation
Introduction
Outbreaks of acute coronary syndrome (SARS-COV-2) have led to widespread death worldwide. According to statistics, millions of people have been infected so far. Many discharged patients suffer from physical and psychological complications of this disease (1,2). COVID-19 involves systemic inflammation with increased oxidation depending on the degree and severity of the symptoms (3). The systemic inflammatory condition persists over time and defines what the scientific literature describes today as the “long COVID” (4). Meanwhile, due to the infectious nature of SARS-COV-2, the lungs are one of the most vulnerable organs and many people suffer from lung diseases caused by this disease. Therefore, paying attention to improving the clinical condition or reducing pulmonary complications in such patients is one of the priorities of treatment-rehabilitation teams. Pulmonary rehabilitation refers to the treatment and individual rehabilitation of patients with chronic lung disease after careful evaluation. The purpose of pulmonary rehabilitation is not only to improve the patient’s physical and mental condition but also to help the patient return to family and community more quickly (5).
Choosing a well-structured, directed, or supervised physical exercise will restore antioxidant defenses when an inflammatory condition occurs (6). Various studies have confirmed the role of exercise training, including respiratory muscle strengthening exercises, and endurance and strength exercises, in improving the symptoms of COVID-19, physical activities, and improving the quality of life of patients (7). Exercise and physical activities prevent or control physical injuries such as inflammation, cartilage, and bone degeneration, improve aerobic capacity, strengthen memory and learning power, and improve neurological and cognitive functions (8).
Physical exercises should be used according to the severity of the symptoms, the level of the disease and the general condition of each patient. For example, in cardiovascular patients, high-intensity interval training is more beneficial than moderate-intensity training due to increased heart pumping and hypoxia. However, this type of exercise is not recommended for everyone with any sports background. Meanwhile, in patients with pulmonary failure, whole-body vibration termination and modified rehabilitation exercises can help improve lung function (7,9).
On the other hand, various scientific sources point to the positive and enhancing effects of exercise on the expression and function of the ACE2 cell receptor at the level of various cells in the body. Therefore, the effects of exercise on preventing the entry of COVID-19 virus into the cell and the infection of people with COVID-19, has become an important challenge. However, it can be concluded that exercise can help athletes fight the virus by strengthening the immune system, reducing inflammation, and creating favorable physiological and immunological conditions. It can also limit disease spread and lower mortality in physically active people. Therefore, the present study investigates the effect of exercise on improving respiratory function and physical activity of patients admitted to COVID-19.
Materials and methods
The present study was conducted as a trial (IRCT20160516027929N10) and approved by the Ethics Committee (IR.SBMU.NRITLD.REC.1400.002) in the period from March to July 2021. After obtaining the consent and considering the inclusion criteria, including COVID-19 infection with CT SCAN or PCR test, sedation below 90%, and the ability to perform physical exercises, 90 patients referred to the rehabilitation ward of the hospital were examined. Patients who were unable to exercise, patients with acute neuromuscular disease or multiorgan failure, or those with incomplete medical records were excluded. The patients were divided into two groups based on the code assigned to each patient using a random number method using a random number table. Patients who had odd codes were in the control group and patients who had even codes were in the experimental group.
In both groups, after explaining how to do the work and signing the consent form, all indicators were measured. Both groups received all the usual treatments (drug therapies, invasive or non-invasive ventilation, physiotherapy). Then, in the experimental group, standard exercises were provided to patients to improve their physical condition and exercise capacity. After two weeks and one month later, all indicators were measured again in two groups. Also, during the exercise period, patients, physiotherapists, and physicians were in contact and the exercises were closely monitored.
Quality of life was assessed using the Sf1 questionnaire, exercise capacity using the 6-Minute Walk Test (6MWT), respiratory status with the Borg shortness of breath index, as well as oxygen saturation level (spo2), and physical activity was assessed using the short physical performance battery questionnaire.
Statistical analysis
All quantitative variables as a mean and standard deviation; and qualitative variables were expressed as numbers (percentage). The normality of the quantitative variables was evaluated by the Kolmogorov-Smirnov test and box diagrams and the probability of normality. All statistical tests were analyzed in two domains at a significance level of 5% using SPSS 21 software.
Results
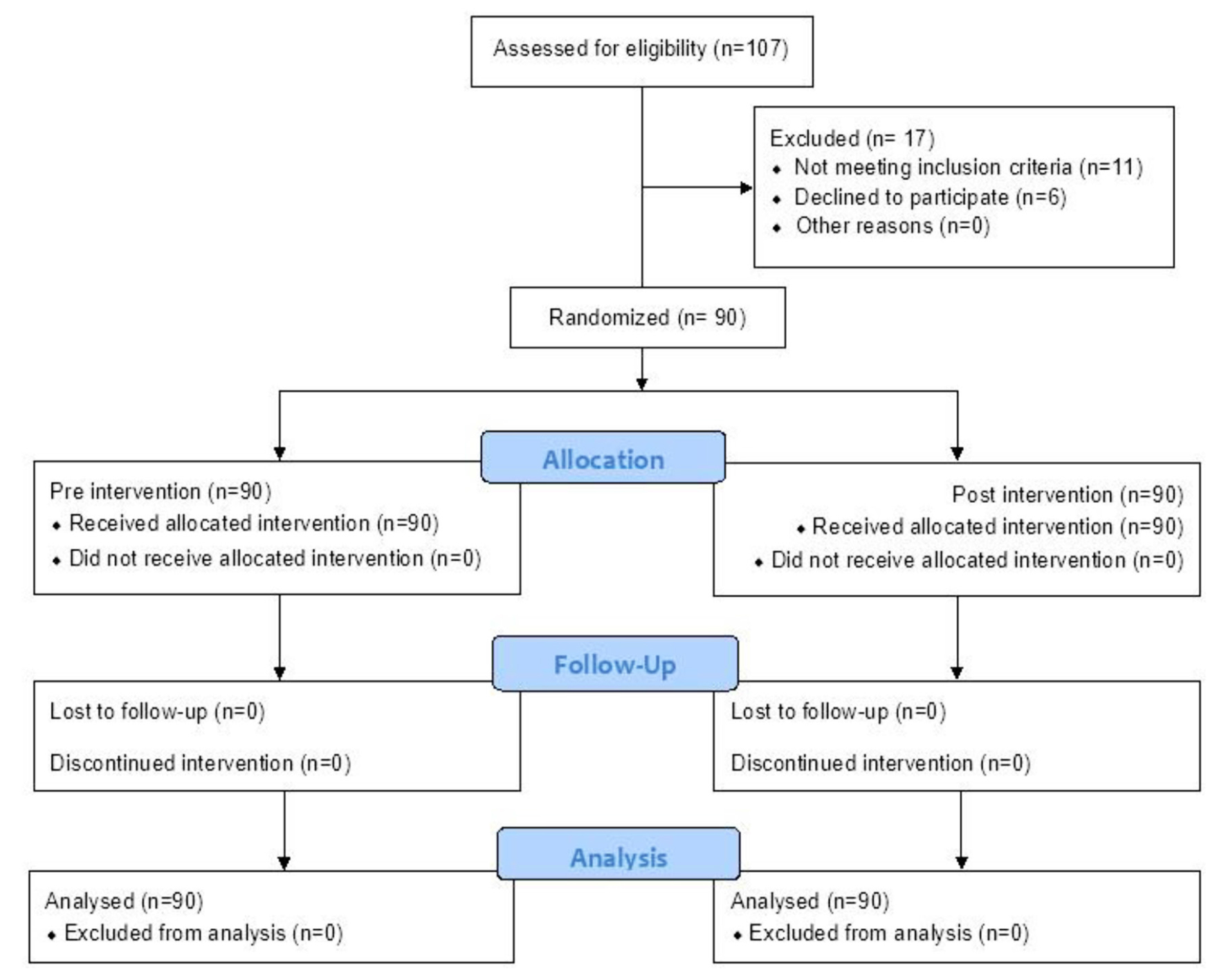
Among 107 patients with COVID-19 referred to Masih Daneshvari Hospital, 90 patients admitted to the COVID-19 ward were included in the study after fulfilling the admission conditions and screening the exclusion criteria (Figure 1).
The mean age of the participants was 13.69 5 51.33 years, while 45.6% (n=41) of the patients were men and 54.4% (n=49) were women. According to the results in table 1, the Body Mass Index (BMI) index in patients was 26.22±4.39, while none of the demographic indicators in patients in the two groups were significantly different. Based on table 2, the independently self-report of daily life activity index was observed after rehabilitation in 89 (98.9%) patients.
A comparative study of the effect of exercise on the indicators studied in table 3, shows that the use of these exercises causes significant changes in indicators such as 6MWT (p=0.001), Balance score (p=0.02), and Sf1 score (p=0.05) in two time periods, before and after rehabilitation in two groups of control and intervention.
Table 1. Evaluation of patients’ demographic conditions by study groups
|
p-value |
Post rehabilitation |
Pre rehabilitation |
Total (n=90) |
Index |
|
0.803 |
21(23.33%) |
20(22.22%) |
41(45.6%) |
Gender (male,n%) |
|
0.371 |
51.71±14.81 |
51.02±12.83 |
51.33±13.69 |
Age (Mean±SD) |
|
0.209 |
174.46±9.04 |
169.02±8.82 |
171.5±9.28 |
Height (cm) (Mean±SD) |
|
0.394 |
77.54±12.68 |
76.16±13.14 |
76.79±12.88 |
Weight (kg) (Mean±SD) |
|
0.138 |
25.43±3.4 |
26.87±5.01 |
26.22±4.39 |
BMI (kg/m2) (Mean±SD) |
Table 2. Intra-group evaluation and evaluation of evaluated indicators in patients
|
Post rehabilitation N (%) |
Pre rehabilitation N (%) |
Variable |
|
|
1(1.1%) |
4(4.4%) |
Dependent |
Self report of daily life activity |
|
89(98.9%) |
86(95.5%) |
Independent |
|
|
30(33.3%) |
73(81.1%) |
Train |
Self report of physical activity |
|
60(66.7%) |
17(18.9%) |
Control |
|
Table 3. The effect of exercise on the indicators
|
P |
F |
Post test (M ± SD) |
Pre test (M ± SD) |
Variable |
|
|
0.001* |
3.34 |
394±109 |
349±108 |
Train |
6 min walk (distance) |
|
350±95 |
325±93 |
Control |
|||
|
0.32 |
-0.98 |
1.39±1.14 |
3.77±3.29 |
Train |
Drop of Spo2 |
|
2.29±1.98 |
4.22±2.9 |
Control |
|||
|
0.02* |
2.36 |
11.68±1.21 |
10.91±2.1 |
Train |
Balance score |
|
11.26±1.3 |
11±1.6 |
Control |
|||
|
0.005* |
2.84 |
35.57±6.44 |
28.16±2.84 |
Train |
Sf1 score |
|
31.37±6.36 |
27.22±4.34 |
Control |
|||
Discussion
The results of the present study showed that the use of exercise in patients with COVID-19 significantly improved physical activity, exercise capacity, and quality of life index in patients. Recent studies have shown that exercise as a non-drug treatment plays an important role in regulating and reducing inflammatory cytokines (10,11). In recent years, it has been shown that there is a strong relationship between disease and inactivity (12).
On the other hand, in several studies, the role of exercise in increasing the expression and activity of ACE2 receptors in humans has been mentioned (13,14). Therefore, the effects of exercise on the pathogenicity of COVID-19 should be compared to a paradox. On the other hand, with additive effects on the function and expression of the ACE2 enzyme receptor, it may not have much effect on preventing the virus from entering the cell. However, due to its physiological, immunological, and anti-inflammatory effects, it can create a reliable safety and physiological barrier to prevent the spread of injury and infection and reduce the risk of death in athletes.
Consistent with what has been presented, Nunes-Silva et al in a study confirmed the relationship between increase of ACE2 function and physical activity (15). In general, many physiological responses of the Renin-Rngiotensin 2 System (RAS) are associated with two opposing pathways: The first pathway, known as the classical pathway, is accompanied by the enzyme angiotensin converter and the conversion of angiotensin I to angiotensin II. This pathway leads to vasoconstriction, cell proliferation, hypertension, sodium retention, and aldosterone secretion. The second pathway, which is an anti-regulatory pathway, differs from the first pathway by converting angiotensin II to angiotensin 1-5, dilating blood vessels, reducing cell proliferation, lowering blood pressure, and protecting the heart and arteries (16). The number of studies on the relationship between exercise and its effects on the 2-5 Ang-ACE2 axis is increasing and most studies are on rats (17,18). Numerous studies have not yet provided a clear idea of the role of exercise in activating or deactivating the Ang-ACE2 pathway. In addition, exercise protocol, intensity, and duration of exercise can have different effects on the components of the Ang-ACE2 2-7 axis (19). In this regard, Silva et al investigated the role of exercise on RAS axis components in tissue, structure, and function of rat heart (20).
Numerous studies provide evidence that moderate-intensity exercise reduces the incidence of infections such as colds. On the other hand, high-intensity exercise can destroy these effects and cause an Upper Respiratory Tract Infection (URTI) (21). Researches suggests that physical activity can improve heart disease, type 2 diabetes, malnutrition, high blood pressure, obesity, sleep disorders, and other physical and mental illnesses, all of which can by weakening the immune system, intensify the pathogenicity of COVID-19 (22).
Due to the development of cytokine storms and widespread inflammation in the infection caused by COVID-19, the anti-inflammatory effects of exercise can also be mentioned. Consistent with this issue, exercise through its anti-inflammatory effects mediates beneficial results in diseases (23). Exercise can also reduce the expression and activation of the 4-TLR receptor in various tissues and cell types, and this is due to the ability of exercise to protect against the inflammatory effects of pathogens (24).
According to the proposed theoretical foundations, it can be said that exercise with anti-inflammatory effects and regulating the function of TLRs, which are important receptors in the path of identifying the immune system against pathogens such as viruses, can increase the level of production of pro-inflammatory agents and interleukins and regulate and control inflammatory cells. On the other hand, reducing inflammation and preventing the formation of cytokine storm in the encounter with COVID-19, is one of the important therapeutic goals of health professionals.
The present study has faced limitations such as the limited study population and the uniqueness of the sampling site. However, in the forthcoming studies, it is suggested that while using a larger community of patients, the disease be treated on a larger scale or in a multi-center manner. However, to improve the quality of future studies, more indicators can be used at the clinical and even molecular level of patients.
Conclusion
Based on the results of the present study, it can be said that performing standard and defined exercise for patients with the new coronavirus, improves physical activity of patients. However, conducting complementary studies with a larger statistical population and reviewing more indicators can provide reliable and more citational results.
Acknowledgement
The authors express their gratitude to all the colleagues of Masih Deneshvari Hospital and all the people who participated in this study.
Conflict of Interest
The authors declare no conflict of interest.