Document Type : Original article
Abstract
Background: External-Beam Radiation Therapy (EBRT) is one of the most important treatments for prostate cancer. Metformin is a multifunctional drug that can control complications following radiotherapy.
Methods: This double-blind, randomized clinical trial was conducted on patients with prostate cancer candidates for EBRT. Patients were randomly assigned to two groups receiving oral Metformin (n=20) or placebo (n=20). The incidence of acute complications was investigated using radiation therapy oncology group acute complications criteria.
Results: There was no significant change in the number of blood cells before and after treatment in the two groups (p<0.05). The micronuclei number in both groups showed a significant increase during radiotherapy, immediately and one month later (p<0.001). There was no significant difference in number of micronuclei between the two groups (p<0.05). The frequency of urinary complications ≥ grade 2 in the metformin group was lower (p=0.005). There was no significant difference in the incidence of gastrointestinal complications ≥ grade 2 between the metformin and placebo groups (p=0.5).
Conclusion: It is recommended that further studies on Metformin as a radioprotective agent in prostate cancer patients who are candidates for radiotherapy be carried out. This research project was registered in the clinical trial center (IRCT: IRCT20211213053377N1).
Keywords: Blood cells, Gastrointestinal diseases, Humans, Incidence,
Male, Metformin, Prostatic neoplasms, Radiation-protective agents
Introduction
Low toxicity, minimal side effects, cost-effectiveness, and reduced cancer development in patients with type 2 diabetes are the main advantages of Metformin attributed to its antitumor activity (1,2). Many clinical studies have shown the association between Metformin with improvement of cancer outcomes, reducing cancer mortality, and reduced incidence of various hormone-sensitive tumors, including colon, breast, pancreatic, and prostate (3-5). Since steroid hormones are cholesterol derivation, it can traverse across the plasma membrane and regulate gene expression (6,7).
Based on the report of Global Statistic Cancer 2022, the incidence and mortality rate of prostate cancer has raised significantly (8). In contrast, a national cancer survival study in Iran revealed that even with a high five-year survival, Iranian cancer patients experience a worse prognosis than developed countries (9). In addition to the prevalence, several risk factors contribute to second cancer development following treatment begins in prostate cancer (10). In this line, there is a need to conduct clinical studies to improve progression-free survival and cancer patients’ time to progression.
Radiotherapy (RT) is a vital cancer treatment strategy, and half of cancer patients undergo RT. External-Beam Radiation Therapy (EBRT) has been used to treat prostate cancer since the 1950s and is still widely used in prostate cancer. Radiation-related lymphopenia and reduced DNA damage response are radiotherapy complications which was demonstrated to reduce overall survival (11,12). Due to the proximity of the prostate to the rectum and bladder, pelvic irradiation makes the irradiation of these areas unavoidable. As a result, it limits the required dose intended for the tumor. Complications such as burning and discomfort in the anus, diarrhea, rectal bleeding, stool incontinence, urinary urgency, urinary frequency, and hematuria faces the treatment with challenge (13,14).
Many studies have shown that Metformin significantly reduces DNA damage caused by toxic agents (15). In this study in order to decrease the radiation-related adverse events, the efficacy of Metformin in clinical outcome improvement was evaluated. Metformin with anticancer properties may help reduce treatment-related complications in prostate cancer.
Materials and Methods
Selection of patients
This double-blind, randomized clinical trial study was conducted on patients with prostate cancer candidates for EBRT, in 2021. Patients with localized prostate adenocarcinoma who were prescribed definitive or postoperative EBRT, aged more than 18 years old, with normoglycemic patients (HemoglobinA1C <6.5% or fasting plasma glucose ≤6.9 mmol/L) (16) were included in the study.
The exclusion of patients was conducted based on the following criteria: patients with metastatic prostate cancer, previous treatment (radiotherapy or chemotherapy), lactic acidosis (eGFR<45 ml/min/1.73 m2) (16), liver dysfunction, cardiovascular disease, severe respiratory disorders, blood disorders, diabetic patients, and subjects with hypersensitivity to Metformin. Also, smoking and lymph node metastatic subjects were excluded, too.
All demographic and clinical information of the patients was collected. Informed consent was obtained from each participant. The study is based on the approval of the Medical Ethics Committee of the Ahvaz Jundishapur University of Medical Sciences. In all stages of this research, the provisions of the Helsinki research ethics statement and the principles of confidentiality of patient information were observed. This research project was registered in the clinical trial center. The date of first registration for sample collection was 21/01/2022.
Study design
Before starting the trial, patients were randomly divided into two groups using computer and Excel software. A person from the hospital staff, who was not responsible for selecting and registering patients or assigning treatment, performed the randomization. A random allocation sequence was performed without knowing which treatment the patient would receive.
In the intervention group, three days before the start of EBRT and up to one month after EBRT, patients received oral metformin tablets at a dose of 1000 mg/day as a single dose.
In the control group, the patients received a placebo with the same dose of 1000 mg (glucose pill) daily from three days before EBRT to one month after. Patients consumed a placebo 2 hr prior EBRT. The appearance and packaging of the placebo were exactly similar to Metformin. A specialist who conducted the intervention and outcome measurements was unaware of the patient’s grouping. Also, the type of treatment and patient grouping were blinded for patients, researchers, and statistical analyzer.
Treatment strategy
All patients underwent EBRT. Information about surgery, Androgen Deprivation Therapy (ADT), EBRT, and risk grouping of patients was also collected. ADT treatment was performed for all patients in intermediate and high-risk groups. The risk group of patients was determined based on the National Comprehensive Cancer Network (NCCN) classification (17).
Radiotherapy plan
Based on the operation history, patients were classified into two groups. Patients without operation history were high and intermediate-risk. The EBRT was conducted in two phases; in phase I, 40 Gy was received by the pelvis, and in phase II, the total dose received by the prostate reached 72 Gy (delivered dose). This protocol was conducted for patients with surgery with the following criteria: positive for margin, extension capsular, and seminal vesicle involvement. Operated patients without the mentioned criteria (prostate bed) and low-risk patients received 66 Gy EBRT. The oncologist determined the dose and number of radiotherapy sessions. For patients who needed definitive radiotherapy, 36 sessions of external radiotherapy with a dose of 72 Gy were performed. For patients who needed postoperative radiotherapy, 33 sessions were conducted with a dose of 66 Gy. It is important to note that the surgery was performed when the life expectancy was estimated to be more than ten years.
Blood cell count
From each patient, 2.5 ml of blood was taken before the first EBRT session (baseline), during the treatment, immediately after the radiation therapy sessions, and one month after the end of EBRT. Blood samples (white blood cells, red blood cells, and platelets) were analyzed using an automatic cell counter.
Investigation of genotoxicity
Cytokinesis block micronucleus assay was used to investigate genotoxicity. The micronucleus test is an essential indicator for studying the effects of clastogenic (factors that lead to chromosomal breakage), aneugenic (elements that have a destructive impact on the division spindle or centromere), and cytotoxicity of physical and chemical factors, which can be done in both in vitro and in vivo conditions (18). To perform this test, 0.5 ml of blood sample was added to a cell plate containing 4.5 ml of RPMI-1640 culture medium. Then, FBS serum (15%), 1% penicillin-streptomycin mixture, and M. phytohemagglutinin mitogen substance were added. The culture plates were kept in an incubator at 37°C, and cytochalasin B was added after 44 hr. 72 hr after the cultivation of lymphocytes, the culture containers were transferred to a centrifuge tube with a Pasteur pipette and centrifuged for 8 min at 800 rpm. Finally, the upper liquid was removed slowly, and 1 ml of the tube bottom has remained intact.
6 ml of hypotonic potassium chloride (KCL) solution was added to the tubes and mixed 2-3 times using a plastic Pasteur pipette. Immediately after adding KCL, the samples were centrifuged at 1000 rpm for 5 min. The upper liquid was removed slowly so that about 1 ml remained. Then, to separate all the lymphocytes, the sample was moved for 1 min using a manual shaker. 2 ml of cold fixing solution (1:6 ratio of acetic acid and methanol) was added to cell fixation; the final volume of the sample was brought to 9 ml using this solution. The samples were centrifuged at 800 m for 8 min, and the upper solution was removed. This process continued until the solution on the cells became clear and colorless (at least three times). In the last step, when the remaining is only 0.5 ml, we shake it until it is ensured that the cells are entirely separated from each other, and a uniform suspension solution is obtained. All the samples were kept in the refrigerator for 24 hr to better cell fixation. From a distance of 10 cm, 3 drops of cell suspension were poured on each slide, and the slides were slightly turned upside down so that the maximum number of cells remained on the slides, then placed at room temperature to dry completely. The slides were stored in the freezer to spread the cells better (19). To better stain cells, 2-3 days after preparing the slides, Giemsa staining was done. Finally, the slides were examined with 40×magnification, and at least 1000 binucleate cells and the number of micronuclei in them were counted for each sample.
Investigating urinary and lower gastrointes-tinal complications
All patients were evaluated for developing urinary and lower gastrointestinal complications during RT. The patients were ranked by Radiation Therapy Oncology Group (RTOG) acute complication criteria (Tables 1 and 2) (20).
Statistical analysis
The normality of data was assessed by Kolmogorov–Smirnov. Mean, and Standard Deviation (SD) were used for quantitative variables to describe data dispersion. Frequency and percentage were used for qualitative variables. An Independent t-test was used to compare quantitative variables between the two groups, and a Chi-square test was used to compare qualitative variables between the two groups. The mean comparison of the variables before and after the treatment was evaluated by paired t-test, and the analysis of variance of repeated measures assessed the changes in the comparison of the variables at different times. The pairwise comparison of the two groups was investigated with Bonferroni’s post hoc test. The significant level was considered as 0.05. All studies were conducted using SPSS 25 (IBM Corp., Armonk, NY, USA).
Results
Patients with prostate cancer who are candidates for EBRT were included. Based on the inclusion criteria, 40 patients were randomly selected and divided into two groups: the placebo group (n=20) and the intervention or case group (n=20). The mean age of participants was 72.43±8.32 years (51-83). There were no significant differences between groups when adjusted for age, weight, Body Mass Index (BMI), HbA1c level, risk group, EBRT treatment, surgery, and ADT (p-value <0.05) (Table 1). The results of the Kolmogorov–Smirnov test showed that all numeric data have a normal distribution.
Evaluating Intervention Efficacy
Cell blood counts: All patients were evaluated for differences in CBC before and after treatment; a significant difference was not found (p-value <0.5). Next, the analysis was done between placebo and intervention groups; as shown in table 2, a significant difference was not observed (p-value >0.05) (Table 2).
Table 1. The demographic information of included patients
|
Variables |
Subgroup |
Intervention group (n=20) |
Placebo group (n=20) |
p-value |
|
Age (year) * |
- |
73.61±8.47 |
71.23±8.18 |
0.391 |
|
Weight (kg) * |
- |
82.40±8.92 |
81.21±7.46 |
0.607 |
|
BMI (kg/m2) * |
- |
28.18±4.18 |
27.61±3.72 |
0.631 |
|
HbA1c (%) * |
- |
5.87±1.23 |
5.71±1.08 |
0.914 |
|
NCCN risk group (%) ** |
Low |
0 |
1(5) |
0.473 |
|
Intermediate |
4(20) |
2(10) |
||
|
High |
16(80) |
17(85) |
||
|
EBRT (%) ** |
Definitive |
16(80) |
17(85) |
0.606 |
|
Postoperative |
4(20) |
3(15) |
||
|
ADT** |
Before EBRT |
20(100) |
19(95) |
0.33 |
|
Concurrent EBRT |
20(100) |
19(95) |
||
|
After EBRT |
20(100) |
19(95) |
BMI: Body Mass Index, HbA1c: HemoglobinA1C, NCCN: National Comprehensive Cancer Network, EBRT: External Beam Radiotherapy, ADT: Androgen Deprivation Therapy.
*p-value, **Chi-square, *Independent t-test, **Paired t-test, CBC: Cell blood count; RBC: Red blood cells; WBC: White blood cell; ALC: Absolute Lymphocyte; PLT: Platelet.
Table 2. Evaluating efficacy of treatment and therapy before and after treatment and between two groups.
|
CBC parameters |
Intervention group (n=20) |
Placebo group (n=20) |
p-value * |
||
|
RBC (10*12/L) after treatment |
Before treatment |
5.12±2.45 |
5.25±2.18 |
0.325 |
|
|
5.14±1.92 |
5.22±1.34 |
0.394 |
|
||
|
p-value** |
0.3 |
0.2 |
|||
|
WBC (×109/L) |
Before treatment |
6774.28±2023.23 |
6581.66±2256.57 |
0.316 |
|
|
After treatment |
6527.54±2163.63 |
6371.13±2400.60 |
0.671 |
||
|
p-value** |
0.6 |
0.5 |
|||
|
ALC (×10³/μL) |
Before treatment |
1714.12±517.68 |
1765.85±597.43 |
0.809 |
|
|
After treatment |
1695.22±474.58 |
1685.47±427.61 |
0.503 |
||
|
p-value** |
0.1 |
0.09 |
|||
|
PLT (×10³/μL) |
Before treatment |
275.37±64.21 |
264.48±62.47 |
0.534 |
|
|
After treatment |
272.05±61.75 |
263.60±51.85 |
0.691 |
||
|
p-value** |
0.9 |
0.1 |
|||
*Independent t-test, **Paired t-test, CBC: Cell blood count; RBC: Red blood cells; WBC: White blood cell; ALC: Absolute Lymphocyte; PLT: Platelet
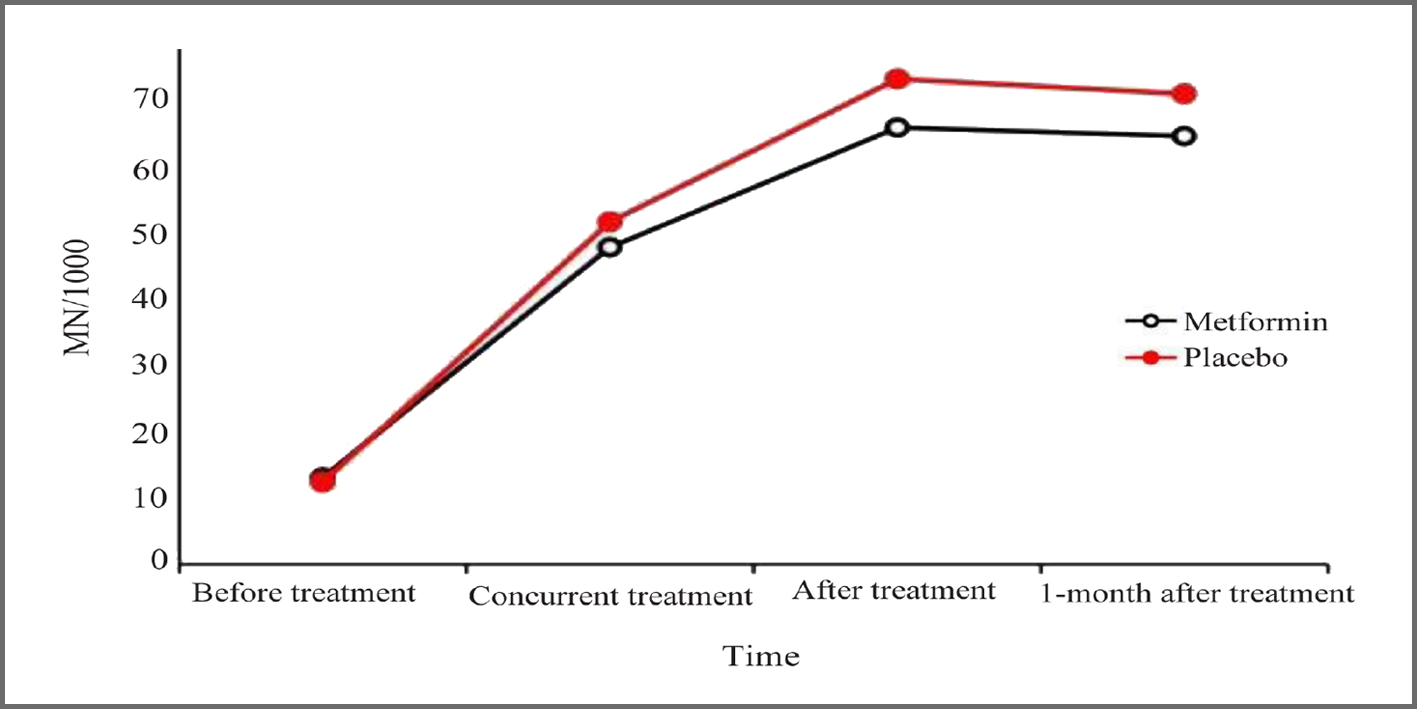
Table 3. Evaluating the association between increasing micronuclei count and therapy progression.
|
Time |
Intervention group (n=20) |
Placebo group (n=20) |
p-value * |
|
Before treatment |
13.18±3.27 |
12.43±4.18 |
0.602 |
|
Concurrent treatment |
48.05±10.18 |
51.91±10.93 |
0.401 |
|
After treatment |
66.21±9.46 |
73.53±10.12 |
0.091 |
|
1-month after treatment |
64.92±9.22 |
71.31±9.87 |
0.123 |
*Independent t-test.
Table 4. Compression nuclei count through different stages of treatment.
|
Time |
Differences of Levels |
Mean differences ± SD |
95% Confidence interval (CI) |
p-value * |
|
Intervention group |
||||
|
Before treatment |
Concurrent treatment |
34.87±6.91 |
0.1-2.7 |
0.002 |
|
After treatment |
53.03±6.19 |
0.9-2.6 |
<0.001 |
|
|
1-month after treatment |
51.74±5.95 |
0.6-2.9 |
<0.001 |
|
|
Time |
Differences of Levels |
Mean differences±SD |
95% Confidence interval (CI) |
pvalue |
|
Placebo group |
||||
|
Before treatment |
Concurrent treatment |
39.48±6.75 |
-0.24 -0.9 |
0.023 |
|
After treatment |
61.1±5.94 |
-0.1-1.7 |
0.003 |
|
|
1-month after treatment |
58.88±5.69 |
1.34-7.2 |
<0.001 |
|
*LCD, One way ANOVA analysis.
Table 5. Frequency of acute gastrointestinal AEs due to radiotherapy in two groups
|
Gastrointestinal AEs |
Intervention group (n=20) |
Placebo group (n=20) |
p-value* |
|
No AEs (%) |
1(5) |
2(10) |
0.523 |
|
Grade 1 (%) |
16(80) |
17(85) |
|
|
Grade 2 (%) |
3(15) |
1(5) |
*Chi-square.
Table 6. Frequency of acute urinary AEs due to radiotherapy in two groups
|
Acute urinary AEs |
Intervention group (n=20) |
Placebo group (n=20) |
p-value* |
|
Grade 1 (%) |
17(85) |
7(35) |
0.005 |
|
Grade 2 (%) |
3(15) |
12(60) |
|
|
Grade 3 (%) |
0 |
1(5) |
*Chi-square.
Evaluating the safety of intervention
The results of the present study have shown there are no significant differences between placebo and intervention groups for micronuclei count (p-value >0.05) (Table 3) (Figure 1). There was a significant difference between placebo intervention groups for micronuclei counts following treatment (F=11.359 vs. F=13.353) (p<0.001). Post-hoc analysis showed the highest differences between before treatment and one month after treatment for nuclei count (p-value <0.05) (Table 4).
Adverse events of radiotherapy
Adverse Events (AEs) were evaluated based on the RTOG criteria. The incidence of gastrointestinal AEs between the two groups was not significantly different (p-value =0.5) (Table 5). Meanwhile, the frequency of acute urinary AEs≥grade 2 was significantly higher in the placebo group (p-value =0.005) (Table 6).
Discussion
EBRT is one of the primary prostate cancer therapies. EBRT can destroy cancer cells through direct and indirect effects. Radiation produces free radicals and toxic substances, which lead to DNA damage and cell death. Many studies have shown the suppressive effect of Metformin on cell signaling involved in proliferation, oxidative phosphorylation, and inflammation in cancer cells (21,22). In this study, we also investigated the radiation protection effect of Metformin against urinary and gastrointestinal complications and genotoxicity caused by radiation therapy in patients suffering from prostate cancer.
The results of the present study showed that the number of blood cells (RBC, WBC, absolute lymphocyte count, and platelets) was insignificant between intervention and control groups in pre- and post-treatment. The same surveys have shown no significant difference in blood cells following RT (23,24). However, Pinkawa’s et al reported that prostate RT has a small but significant effect on the number of blood cells, which can be observed even after a few weeks (25). The results of EBRT on blood cells and immune function depend on the factors, including the radiotherapy total dose, irradiated volume, primary tumor location, the levels of blood cells pre-treatment, simultaneous therapies, the number of surviving cells, and their capacity to migrate into the microenvironment (26-28).
The present investigation was done specifically for each patient. As mentioned earlier, patients were evaluated based on the NCCN criteria. In this line, high-risk patients were treated for pelvic lymph nodes. In the same with this study, the effect of Metformin on the blood cell count was investigated in patients with differentiated thyroid cancer who were treated with radioactive iodine-131. The results showed that the WBC reduction in patients treated with Metformin was significantly lower than the control group. Their results indicate that Metformin with inhibition effects of iodine-131 reduces the CBC parameters compared to the control group (29).
There is not much evidence about the effect of Metformin on the number of blood cells in prostate cancer patients undergoing radiotherapy, so it is recommended that more studies be conducted to investigate the effect of Metformin on the number of blood cells in this group of patients. However, it seems that Metformin, by affecting the cell repair signaling and preventing genomic instability, can prevent the severe destruction of cells against radiation.
Micronucleus is a biomarker of chromosomal fragmentation that is produced following radiation exposure. Lymphocytes are sensitive cells to radiation and prone to chromosomal damage; hence, they are widely used to evaluate genotoxicity in EBRT (30).In the present study, the number of micronuclei in peripheral blood lymphocytes increased 3-8 times post-treatment compared to pre-treatment. In the Metformin group, immediately after treatment, the number of micronuclei increased less compared to the placebo, which may indicate the radiation protection effect of Metformin. It agrees with Cheki et al’s findings; they demonstrated that using Metformin two hours before radiation could reduce DNA damage and cell apoptosis caused by ionizing radiation. Also, they found that the micronuclei count was significantly lower in EBRT and Metformin than in the EBRT without Metformin (31). The present study’s lack of significant differences could be due to the lower sample size. Further studies are needed to optimize the efficacy of Metformin in RT of patients with prostate cancer, such as optimal dose, administration time, and molecular mechanisms.
Radiation causes the generation of free radicals and toxic substances and leads to DNA damage and genotoxic effects in cells (32,33). Studies have shown that Metformin has antioxidant activity (34,35), and its therapeutic effects have been reported in patients undergoing EBRT (36). Metformin suppresses Human Epidermal growth factor Receptor-2 (HER2) onco-protein, inhibiting oxidative phosphorylation and fatty acid oxidation, causing selective toxicity for p53-deficient cells (37,38). In an H2O2-inducible oxidative stress model, Metformin attenuated H2O2 p-ERK activation, enhanced H2O2 p-AMPK expression, attenuating pro-survival signals and potentiating the Adenosine Monophosphate-activated Protein Kinase (AMPK) activation under oxidative stress (39,40). AMPK is activated by cellular stress, such as hypoxia and oxidative stress, induced by an increase in the ratio of Adenosine Monophosphate (AMP) to Adenosine Triphosphate (ATP) (41).
The direct anticancer mechanism of Metformin is associated with AMPK activation and inhibition of rapamycin (mTOR) activity in mammals (42,43).Metformin enters complex 1 of the electron transport chain and blocks its activity, reducing oxygen consumption and ATP production (44). When AMPK is activated, it leads to downstream inhibition of the rapamycin signaling complex-1 (mTORC1) mammalian target and activation of the tumor suppressor Tuberous Sclerosis Complex 2 (TSC2, tuberin). Inhibition of mTOR leads to attenuation of protein synthesis and growth and proliferation of tumor cells through downstream targets (45). In addition, inhibition of the Krebs cycle may directly affect other metabolic pathways, such as lipid synthesis and beta-oxidation, which are critical in prostate cancer metabolism (46).
Indirect activation of AMPK by Metformin inhibits the transcription of glycogenesis-related genes in hepatocytes. Decreased glycogenesis increases glucose absorption in muscle cells and thus reduces serum glucose and insulin levels (47,48). Insulin receptors in cancer cells with high insulin levels promote mitogenic effects, tumor growth, and proliferation (49). Many studies have associated hyperinsulinemia with prostate cancer’s development, progression, and aggressiveness (50,51). In summary, metformin exerts its protective effect on cells by increasing free oxygen and decreasing fasting blood glucose and insulin.
The present study showed that Metformin significantly reduces grade 2 and higher urinary complications. However, the severity of digestive complications did not differ substantially between the two groups. As an AMPK activating agent, Metformin reduces acute and chronic intestinal toxicity caused by radiation by optimizing mitophagy dependent on AMPK (52). In a meta-analysis, the incidence of long-term genitourinary complications (60 months) grades 2≤RTOG in prostate cancer patients treated with RT has been reported to be 17% (53). Late side effects of RT in prostate cancer were also investigated in a randomized trial using the RTOG scale, and 22% of patients experienced grade 2 or higher gastrointestinal or urinary adverse events (54,55).Metformin leads to subsequent downregulation of the Phosphoinositide-3-Kinase (PI3K) axis by decreasing circulating insulin. The PI3K pathway is involved in growth, proliferation, differentiation, and motility, and following the androgen receptor pathway, it is the second major factor in prostate cancer growth (45). The results of a recent clinical trial by Kim et al showed that Metformin could significantly decrease grade 2 urinary complications and is generally safe and well tolerated by patients (16). Their further analysis revealed that the urinary urgency frequency was significantly lower following metformin use. However, the meaning of decreasing urinary urgency was borderline, which can be due to sample size.
On the other hand, it was found that urinary complications were influenced by race and ethnicity, such as urinary urgency, which is most prevalent in non-Hispanic black men. Hence, these irrupting factors in interpreting treatment outcomes should be considered.
In general, the effect of Metformin is multi-signal and has many molecular effects on cancer and non-cancer cells. The predominant mechanism of Metformin in prostate cancer is unknown, but both direct and indirect pathways are likely to have anticancer benefits. However, it was found that Metformin can activate the immune system and eliminate the cancer stem cells (56). Also, whether AMPK activation is essential for metformin activity remains unclear, as its ability to inhibit mTORC1 has also been shown through AMPK-independent pathways. Further research is ongoing to explain better the mechanisms of Metformin in prostate cancer treatment.
Conclusion
The present study showed that using Metformin in prostate cancer alongside EBRT effectively reduces acute urinary complications and is not accompanied by life-threatening gastrointestinal complications. However, the micronuclei count was not significantly reduced compared to the control group, but features such as cost-effectiveness, desirable safety, and availability are some of the benefits of Metformin usage in EBRT treatment of patients who suffer prostate cancer.
Ethical approval
The study was conducted in accordance with the Declaration of Helsinki the Research Ethics Board approved our study (IR.AJUMS.HGOLESTAN.REC.1400.111). In all stages of this research, the provisions of the Helsinki research ethics statement and the principles of confidentiality of patient information were observed. This research project was registered in the clinical trial center of Iran (IRCT: IRCT20211213053377N1) study participants to publish their identifiable data in an online, open-access journal.
Consent for publication
Consent to publish was obtained before study from each patient.
Acknowledgement
We thank all our colleagues at Allied Health Sciences School, Ahvaz Jundishapur University of Medical Sciences.
Conflict of Interest
The authors declare no conflict of interest. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or compared ethical strands.
12.van Oorschot B, Hovingh SE, Moerland PD, Medema JP, Stalpers LJ, Vrieling H, et al. Reduced activity of double-strand break repair genes in prostate cancer patients with late normal tissue radiation toxicity. Int J Radiat Oncol Biol Phys 2014;88(3):664-70. https://pubmed.ncbi.nlm.nih.gov/24411188/