Document Type : Original article
Abstract
Background: Patients’ complaints against hospital staff reflect dissatisfaction with care and service, indicating gaps in the healthcare delivery system. This study investigates the causes of complaints against medical staff referred to the Kerman healthcare organization before and after the COVID-19 epidemic.
Methods: This cross-sectional study examined claims filed against medical staff during two years—2018 (before COVID-19) and 2019 (after COVID-19). The data, collected from 154 forensic medical cases (120 in 2018, 34 in 2019), included the year of complaint, complaint outcome, reasons, and defendant’s education level.
Results: Indictments were issued for 31.2% (48 cases), prohibition of prosecution for 63.6% (98 cases), and suspension of prosecution for 8.2% (8 cases). Complaints due to complications were 61% (94 cases), mostly before COVID-19 (74 cases). Complaints due to patient death increased post-COVID-19 (8.4%, 13 cases). After the epidemic, most complaints were against physicians (70.5%) and dentists (20.6%) (p=0.001). Before COVID-19, complaints were highest among gynecologists and obstetricians (18.3%), surgical specialists (14.2%), and general practitioners (9.2%). Post-COVID-19, the highest complaints were against surgical specialists (20.6%), dentists (20.6%), and orthopedic specialists (17.6%).
Conclusion: Complaints against medical staff decreased post-COVID-19 compared to the previous year. The highest complaints were against gynecologists and obstetricians, surgical specialists, dentists, and orthopedic specialists. Common causes included death, complications due to lack of skill, and carelessness. Monitoring the performance of specialties with the highest complaints is necessary.
Keywords: Complaints, COVID-19, Healthcare complaints, Health personnel, Patient satisfaction, Physicians
Introduction
Medical errors harm patients when treatments fall short of approved standards, often due to lacking skills or care compared to peers in the field (1,2). Forensic medicine is essential in clarifying medical responsibilities and preventing misinterpretations of scientific evidence in healthcare-related claims (3). Despite efforts by physicians and medical staff, along with advanced facilities, patient dissatisfaction, complaints, and lawsuits against healthcare professionals and institutions are steadily increasing worldwide (4). Iranian Forensic Medicine Organization statistics indicate a rising trend in complaints regarding medical staff malpractice in recent years. Among healthcare providers, general practitioners receive the most forensic medical complaints, followed by nurses (5,6).
Patients’ complaints against medical staff are among the foremost occupational tensions in this profession, demanding resolution (7). However, these complaints only represent a fraction of the dissatisfaction within the healthcare system, with many preventable adverse events and treatment failures going unreported (8). Medical malpractice, a significant issue in medical ethics, entails the failure to fulfill duties, including conducting thorough diagnostic measures and administering appropriate treatment (9). Despite causing adverse health consequences for patients and their families, medical malpractice can also impose additional emotional and economic burdens, including job burnout, diminished quality of life, and reduced professional satisfaction among healthcare providers (10-12).
Injuries during a patient’s treatment can stem from medical malpractice or the natural progression of the disease. Not all errors in medical care constitute malpractice, as even highly skilled doctors may err due to the inherent limitations of medical science (13,14). Additionally, not all instances of medical malpractice result in harm to the patient or legal action. From a societal perspective, addressing medical malpractice aims to eliminate unsafe medical practices, provide compensation to those harmed, and ensure fair and accurate judgments (15). In Iran, investigations into medical malpractice typically occur following patient or family complaints, with the goal of holding the responsible party accountable (16).
Studies have revealed that most cases of medical malpractice result from medical staff negligence (16). Furthermore, analysis of malpractice complaints indicates that a significant portion involve non-doctors, with causes often attributed to negligence, lack of skill, and failure to adhere to established protocols (17). Certain medical specialties, including orthopedics, obstetrics, gynecology, general surgery, and otolaryngology, are more frequently associated with malpractice cases, with approximately a quarter resulting in convictions (17).
Medical malpractice, involving errors in service provision or wrongful actions in planning or execution, can lead to undesirable outcomes, complications, and even death (17).
The emergence of COVID-19 in 2019 quickly became a global concern, with epidemiological findings highlighting its rapid human-to-human transmission (18). The disease has caused widespread infections and high mortality rates worldwide, including in Iran (19). Its rapid spread, severe cases, and lack of specialized treatment pose a significant threat to public health (20). The COVID-19 pandemic has impacted all areas of life, especially healthcare and medical staff. Despite medical advancements, patient dissatisfaction and complaints are rising due to factors like population growth, increased patient awareness, and medical errors. Communication gaps between doctors and patients are a primary concern. This study examines complaints against medical staff in the Kerman healthcare organization before and after the pandemic, highlighting the ongoing importance of addressing medical malpractice.
Materials and Methods
The sample size for the cross-sectional study conducted in 2022, utilizing complaints filed in the forensic medicine of Kerman during 2018-19, was determined through the examination of complete cases meeting inclusion criteria and availability for analysis. Out of the 220 existing cases, 154 complete cases were ultimately included after excluding those with incomplete or insufficient information or those not finalized for any reason. Data were collected from files in forensic medicine related to complaints from medical staff, as well as information recorded in the file system of the forensic medicine commission of Kerman city, with efforts made to remove duplicate cases. This sample size of 154 cases was utilized for analysis, aiming to ensure representativeness and reliability in assessing the study objectives. The data were collected using a researcher-made checklist containing the year of the complaint, the complaint outcome (including indictment, prohibition of prosecution and suspension of prosecution), causes of complaints filed against the medical staff (including causing complications, cost, bad behavior, moral, unlicensed practice, and death), educational degree and level of education of the defendant.
Since maintaining the confidentiality of the information of forensic medical files has its own conditions, the data were extracted from the files by the employees of the forensic medical department, and the information related to plaintiffs and defendants was recorded and coded without mentioning their names and details.
The present study was approved in the Research Ethics Committee of Kerman University of Medical Sciences and ethics system in biomedical research with IR.KMU.AH.REC.1400.131. The data were analyzed using SPSS version 22 statistical software, employing various statistical tests. Descriptive analysis was first conducted to explore the distribution of complaints against the medical staff within the Kerman medical system organization. Subsequently, comparative analysis was undertaken using Chi-square and Fisher’s exact tests to discern differences before and after the onset of COVID-19. A significance level of 0.05 was adopted for all tests.
Results
In this study, the information of 154 forensic medical cases including 120 cases in 2018 and 34 cases in 2019 were included in the study. In general, during the two years of the study, for 31.2% (48 cases) an indictment has been issued indicating that the medical staff was guilty. In 63.6% of the cases (98 cases), a prohibition of prosecution was issued due to the fact that the medical staff was not guilty, and in 2.5% (8 cases) of the cases were dismissed or postponed due to the prolongation of the investigation process for more than a year or lack of follow-up by the plaintiff. Table 1 reveals that most of the cases of indictment (39 cases), prohibition of prosecution (74 cases) and suspension of prosecution (7 cases) were before the onset of the COVID-19 epidemic.
Investigating the causes of complaints during the two years under study showed that in general, 0.61% (94 cases) of complaints occurred due to complications in patients, most of which (74 cases) occurred before the onset of the COVID-19 epidemic. Misbehavior was in 23.3% of the cases of filed complaints before the onset of the epidemic, which reached 8.8% after the onset of the epidemic. In 8.4% of cases (13 cases), the family of the deceased filed a complaint due to the death of the patient, which increased after the onset of the epidemic (8 cases). Complaints regarding ethical issues and unlicensed practice had the lowest frequency (Table 2).
In table 3, the results of the frequency of complaints filed against the medical staff in the healthcare organization of Kerman, based on evidence, show that before the epidemic, 89.1% of complaints were from doctors and 6.7% from dentists, and after the onset of the epidemic, complaints against doctors with 70.5% and dentists with 20.6% had the highest frequency (p=0.001). The results based on the educational level show that the cases of complaints against general practitioners were 81.7% before the epidemic, and after the onset of the epidemic, complaints against specialists were more frequent (70.6%) (p=0.146).
Table 4 reveals the results related to all the complaints filed against the medical staff, was separated by the type of the medical staff’s job during the study. Out of all the complaints, most complaints were filed against obstetricians and gynecologists (15.6%), surgical specialists (15.6%), and dentists (9.7%). Moreover, before the onset of the epidemic, most complaints were filed against obstetricians and gynecologists (18.3%), surgical specialists (14.2%), and general practitioners (9.2%), and after the onset of the epidemic, most complaints were filed against surgical specialists (20.6%), dentists (20.6%), and orthopedic specialists (17.6%), respectively.
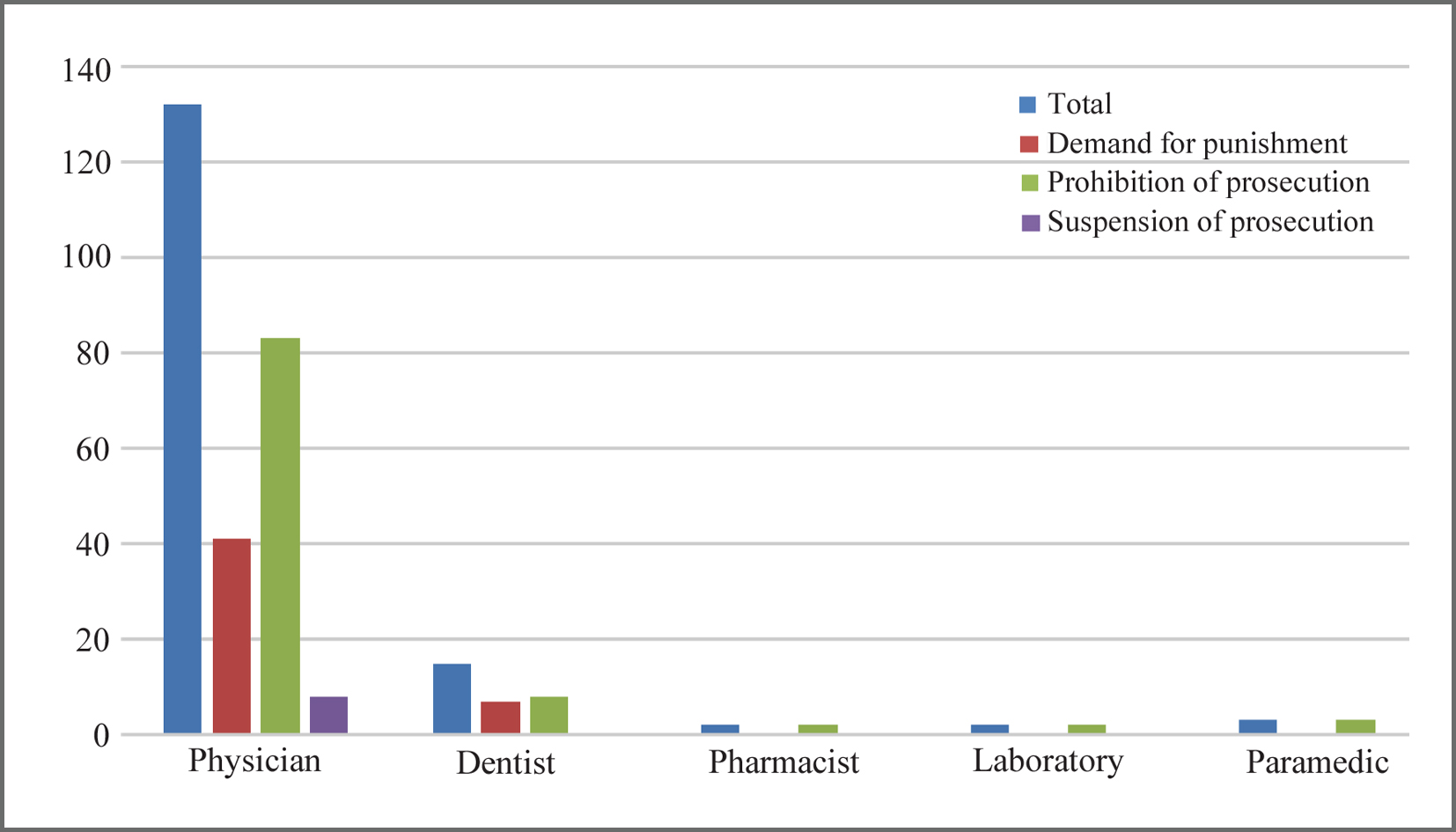
Chart 1 shows the frequency of complaints filed against the medical staff in the healthcare organization of Kerman in occupational groups of doctor, dentist, pharmacist, laboratory and paramedics. As can be seen, most of the complaints, as well as the indictments and the prohibition of prosecution cases were against doctors and dentists (Chart 1).
Table 1. The frequency of complaints against medical staff in Kerman medical system organization before and after the onset of COVID-19 (2018-19)
|
Variables |
Demand for punishment |
Prohibition of prosecution |
Suspension of prosecution |
|
Frequency (%) |
Frequency (%) |
Frequency (%) |
|
|
Before COVID-19 |
39(32.5) |
74(61.7) |
7(58) |
|
After COVID-19 |
9(26.5) |
24(70.6) |
1(2.9) |
|
Total |
48(31.2) |
98(63.6) |
8(5.2) |
Table 2. The frequency of complaint causes against medical staff in Kerman medical system organization before and after the onset of COVID-19 (2018-19)
|
Variables |
Causing complications N(%) |
Cost N(%) |
Misbehavior N(%) |
Moral N(%) |
Unauthorized activity N(%) |
Death N(%) |
|
Before COVID-19 |
74(61.6) |
9(7.5) |
28(23.3) |
2(1.7) |
2(1.7) |
5(4.2) |
|
After COVID-19 |
20(58.8) |
2(5.9) |
3(8.8) |
1(2.9) |
0 |
8(23.5) |
|
Total |
94(61.0) |
11(7.1) |
31(20.1) |
3(1.9) |
2(1.3) |
13(8.4) |
Table 3. The frequency of complaint causes against medical staff in Kerman medical system organization by degree and education level, before and after the onset of COVID-19 (2018-19)
|
Variables |
Total N(%) |
Before COVID-19 N(%) |
After COVID-19 N(%) |
p-value |
|
|
Degree of education |
Physician |
132(85.7) |
107(89.1) |
24(70.5) |
0.001 |
|
Dentist |
15(9.7) |
8(6.7) |
7(20.6) |
||
|
Pharmacist |
2(1.3) |
0 |
2(5.9) |
||
|
Laboratory |
2(1.3) |
2(1.7) |
0 |
||
|
Paramedic |
3(2.0) |
3(2.5) |
0 |
||
|
Grade |
Basic/Master |
3(2.0) |
3(15.8) |
0 |
0.146 |
|
Professional doctor |
29(18.8) |
19(81.7) |
10(29.4) |
||
|
PhD |
122(79.2) |
98(32.5) |
24(70.6) |
||
Table 4. The frequency of raised complaints against the medical staff in the medical system organization of Kerman by job type
|
Variables |
Total N(%) |
Before COVID-19 N(%) |
After COVID-19 N(%) |
|
General practitioner |
12(7.8) |
11(9.2) |
1(2.9) |
|
Dentist |
15(9.7) |
8(6.7) |
7(20.6) |
|
Orthopedics |
16(1.4) |
10(8.3) |
6(17.6) |
|
Obstetrics and gynecology |
24(15.6) |
22(18.3) |
2(5.9) |
|
Surgery |
24(15.6) |
17(14.2) |
7(20.6) |
|
Restorative |
5(3.2) |
4(3.3) |
1(2.9) |
|
Internal |
10(6.5) |
9(7.5) |
1(2.9) |
|
Eye |
7(4.5) |
5(4.2) |
2(5.9) |
|
Neurosurgery |
1(0.6) |
0(0) |
1(2.9) |
|
Cardiology |
4(2.6) |
4(3.3) |
0(0) |
|
ENT |
2(1.3) |
0(0) |
2(5.9) |
|
Urology |
4(2.6) |
3(2.5) |
1(2.9) |
|
Pediatrics |
6(3.9) |
6(5.0) |
0(0) |
|
Anesthesia |
6(3.9) |
6(5.0) |
0(0) |
|
Radiology |
5(3.2) |
5(4.5) |
0(0) |
|
Laboratory |
2(1.3) |
2(1.7) |
0(0) |
|
Psychiatry |
1(0.6) |
0(0) |
1(2.9) |
|
Pharmacology |
2(1.3) |
0(0) |
2(5.9) |
|
Heart surgery |
1(0.6) |
1(0.8) |
0(0) |
|
Neurology |
1(0.6) |
1(0.8) |
0(0) |
|
Emergency medicine |
3(1.9) |
3(2.5) |
0(0) |
|
Nursing |
1(0.6) |
1(0.8) |
0(0) |
|
Surgery room |
1(0.6) |
1(0.8) |
0(0) |
|
Other |
1(0.6) |
1(0.8) |
0(0) |
Discussion
The study analyzed 154 forensic medical cases spanning 2018 and 2019, showing that 31.2% resulted in indictments against medical staff, mostly before COVID-19. Complaint causes included patient complications (74 cases before COVID-19), misbehavior, and patient death (increasing post-pandemic). Complaints were more frequent against doctors than dentists, with a shift towards specialists after the pandemic. Obstetricians, gynecologists, surgical specialists, and dentists were the most complained-about specialties, particularly post-pandemic. Physicians and dentists received the highest number of complaints and legal actions.
Patients’ complaints against medical staff reflect dissatisfaction with care and highlight gaps in the healthcare system. A systematic approach to addressing these complaints in hospitals enhances organizational performance and improves care quality. Comparing and sharing such issues can pinpoint common problem areas, facilitating strategic planning and deficiency elimination (21). Studies have shown that for every written complaint there are 400 dissatisfied patients, which despite the significant advances in science and the existence of new technologies in diagnosis and treatment, the number of complaints has had an ascending trend (22).
With the onset of the COVID-19 disease, many activities communities underwent significant changes. In order to prevent the spread of the disease, people had to stay at home most of the time, and social isolation and reduced mobility along with preventive policies inevitably increased stress levels and reduced access to social support services (23). The results of a study in England showed that the number of complaints registered by the National Health Service (NHS) in the first quarter of 2020, which coincided with the first peak of the COVID-19 epidemic, was significantly lower than the previous year. It was still lower than previous years, although it gradually increased in the next three seasons (24). The initial decline in complaints during the COVID-19 pandemic may be due to increased waiting times, delayed access to services, hospital infections, inadequate care, staff shortages, and decreased empathy. However, these challenges are likely to result in a subsequent increase in complaints. Many doctors struggle to provide adequate care due to heavy workloads and burnout, with a significant proportion fearing litigation and experiencing complaints related to the epidemic (25). Limited research exists on the impact of COVID-19 on complaints against medical staff. However, possible reasons for the reduction in complaints may include initial gratitude and empathy towards healthcare workers during the epidemic’s onset, along with increased community cooperation. Yet, there’s a possibility of a continued upward trend in complaints. Addressing this requires identifying factors contributing to dissatisfaction and adopting strategies to enhance behavioral, communication, and professional skills through training, along with vigilant monitoring and reporting to rectify deficiencies (21).
The study found that the majority of complaints were lodged against gynecologists, obstetricians, surgical specialists, and dentists. Before COVID-19, gynecologists, obstetricians, surgical specialists, and general practitioners faced the most complaints, while after the pandemic’s onset, surgical specialists, dentists, and orthopedic specialists were the most frequently complained-about. Review studies corroborate these findings, indicating that general surgeons, gynecologists, general practitioners, and orthopedic specialists received the highest number of complaints among doctors (26). The results of studies in the healthcare organization of Kermanshah showed that 19% of the complaints were filed against gynecologists and obstetricians, 14% against orthopedic specialists, and 13% against dentists (27). In another study in the Mashhad healthcare organization, 56% of all complaints were against the surgical team and 13% were against dentists and paramedical staff (28). Similar results were obtained in the study investigating the causes of complaints filed against Khorramabad healthcare organization during 2006-11 (29) indicating medical errors play a significant role in adverse outcomes like death and complications.
In 2006, the Director of the Ministry of Health stated that 60% of all maternal deaths resulted from errors in medical, midwifery, and nursing care (30). Due to the invasive nature of their medical procedures, complaints are always filed against the surgical team. In a study in Mashhad, the surgical team was sued about four times more than the non-surgical specialists (28). In another study in Saudi Arabia, the number of complaints filed against surgeons and anesthesiologists was three times higher than that of non-surgeons (31). Also, in another study in Spain, most cases of medical complaints were against obstetricians and gynecologists and the surgical team (32).
The investigation found that most complaints stemmed from patient complications, misbehavior, and patient death; while issues related to ethics and unlicensed practice were less common. Complaints regarding complications, costs, misbehavior, and unlicensed practice were more prevalent before COVID-19, whereas those regarding death and ethics increased afterward. Kalani et al’s systematic review identified carelessness, lack of skill, and non-compliance with government systems as common causes of medical malpractice in Iran (26). In the study by Siabani et al, the most common causes of complaints were treatment complications, death, wrong treatment, and organ defects (27). In another study in Tehran, the most common cause of complaints was the death of the patient (33). In a study in England, most complaints were related to patients’ attitude, wrong diagnosis, long waiting time, short appointment time, and poor communication with the patient (34). In another study in Tehran, the most common reasons for filing a complaint were related to treatment method and the lowest percentage of complaints were due to diagnosis and treatment (22). In 2020, complaints were related to various issues including care and treatment services, tariffs, health and infection control, lack of skill, equipment defects, handling, unlicensed practice, forgery and abuse, and illegal advertising (21). Medical malpractice cases encompass errors in diagnosis, treatment, or disease management, often leading to complaints referred to judicial courts, healthcare organizations, and forensic medicine organizations. While causes of medical complaints vary, common issues include death, complications, lack of skill, and carelessness. Physicians bear legal responsibility for their mistakes, and negligence or lack of skill resulting in patient losses require compensation (35).
This research emphasizes the impact of COVID-19 on patient complaints against medical staff and highlights a decrease in complaints post-pandemic onset compared to the previous year. It identifies specialties like gynecologists, obstetricians, surgical specialists, dentists, and orthopedic specialists as frequent subjects of complaints. Common causes include death, lack of skill, and carelessness. Strategies for addressing these issues involve enhancing training, monitoring, and reporting mechanisms to correct deficiencies. It underscores the need for increased oversight on specialties with high complaint rates. This research can inform future efforts to improve healthcare delivery and reduce medical malpractice.
Conclusion
In the current study, the investigation of complaints filed against the medical staff indicates a decrease in complaints after the onset of the COVID-19 pandemic compared to the year before the onset of the epidemic. Moreover, the cases of complaints filed against gynecologists and obstetricians, surgical specialists, dentists, and orthopedic specialists were more than other specialties, and issues such as death, lack of skill, and carelessness were among the common causes in most studies. It is required to carry out more supervisions on the performance of the specialties that are the subject of most complaints.
Strength and limitation
The study presents a comprehensive comparative analysis of patient complaints against medical staff before and after the onset of the COVID-19 pandemic within the Kerman healthcare organization. Strengths of the study lie in its ability to identify specialty-specific trends and common causes of complaints, providing targeted insights for improving healthcare delivery. However, limitations include its narrow focus on a single healthcare organization, potential biases in complaint reporting, and the lack of qualitative analysis to explore patient perspectives. Additionally, the potential impact of external factors, such as changes in healthcare service utilization patterns during the COVID-19 pandemic, on the frequency and nature of complaints filed against medical staff, further adds to the study’s limitations.
Specifically, it highlights the limitation of not examining the correlation between surgical procedures and complaints, which could provide valuable insights but would also introduce complexities to the study design. Therefore, it points out a potential avenue for further research or improvement in the study’s methodology to address this limitation. Nonetheless, the study offers valuable data for strategic planning and quality improvement initiatives within the healthcare system, emphasizing the importance of addressing systemic issues to enhance patient satisfaction and reduce medical malpractice.
Conflict of Interest
Authors declare no conflict of interest.