Document Type : Original article
Abstract
Background: The present study aimed to assess the frequency, Lingual Concavity Angle (LCA) and the different types of lingual concavity in the posterior mandible.
Methods: In this study Cone Beam Computerized Tomography (CBCT) images of 670 mandibular bodies in the molar areas were evaluated. Cross-sectional images of the mandible were reconstructed at furcation points of first molar area. The LCA was measured. The subjects with LCA smaller than 85° were considered as concave. Then, the concave subjects were classified into three groups: angle less than 40°, angle between 40-60°, and angle between 60-85° were designated as extremely deep, deep, and mild deep, respectively.
Results: The most common type of lingual concavity was mild deep, followed by deep, and extremely deep. There was a significant positive correlation between the LCA and the age of participants (p<0.001). There was also significant relationship between the age of participants and the type of lingual concavity (p<0.001). The subjects in mild deep group were significantly older than deep group (p=0.032). Also, the non-concave subjects were significantly older than deep and mild deep subjects. (p=0.001 and 0.040, respectively). The LCA was significantly higher in males than females (p=0.020). The LCA was significantly larger on the left side (p<0.001).
Conclusion: The presence of deep lingual concavity was common (95%.). Also, mandibular lingual concavity types were found to vary by age, and laterality. Moreover, the LCA was significantly different according to patient age, sex, and laterality.
Keywords: Cone-beam computed tomography, Female, Male, Mandible
Introduction
In recent decades, treatment plans for replacing missed teeth have transitioned. Indeed, implant-based treatments have replaced less favorable, removable prosthetics (1). Due to the high risk of early extraction of the first permanent mandibular molar teeth (2), the posterior of the mandible is a common site for implant placement. Besides, the important neurovascular structures in this region (3), the sigmoid-shaped lingual concavity in this area is another limiting factor for implant placement (1). Lingual concavity imposes the surgeons to choose a narrow diameter implant with a higher length or a shorter implant with a normal diameter in case of sufficient bone volume (1). Insertion of longer length with less diameter implant may have the risk of encroachment to the vascular structures and hemorrhage (4). And, in the latter choice, the normal diameter shorter implant, there is a risk of lingual cortex perforation (5,6).
Perforation of the lingual cortex of the posterior mandible leads to nervous complications. As the course of extension of the lingual nerve passes from the lingual aspect of the mandible, perforation of this cortex damages the mentioned nerve, contributing to persistent infection of the posterior mandible. The spread of the infection into the parapharyngeal and retropharyngeal spaces causes serious life concerns for the patient, including carotid artery rupture, thrombosis of the internal jugular vein with pulmonary embolism, and obstruction of the upper airway (7).
The risk of the lingual cortex perforation is dependent upon the severity of the lingual concavity (8,9). Froum et al (10) and Chan et al (11) conducted studies regarding the risk of lingual cortex perforation during implant placement and revealed that in cases with marked lingual concavity, the risk of perforation of this cortex would be higher. Moreover, in patients who are affected with systemic disorders such as β-thalassemia major, altered mandibular features, necessities higher consideration than normal population prior to surgery (12,13).
A factor that minimizes the time and discomfort of the surgical procedure and, as a result, the post-surgical complications is the surgeon’s awareness regarding the exact angulation of the lingual undercut before surgery. Considering this point would be essential in deep concavities, where drilling mistakes would grow more perilous. Based on the former classification of mandibular lingual morphology, there are three main types: concave, parallel, and convex. When the lingual cortex angulation is less than 85°, it is defined as the concave form, between 85 ° to 95 ° as parallel, and larger than 95 ° as convex type (14). In more recent classification, the concave form itself has three subtypes (15). If the angulation is between 60°-85°, it is classified as mild deep, 40°-60° as deep and less than 40° is considered as extremely deep with the highest risk of lingual cortex perforation (16). In fact, the concavities with angles larger than 60° are considered low risk for perforation during implant placement, which is compatible with Braut et al (17), who divided the lingual concavities into two groups of influential and non-influential ones.
Two-dimensional imagings like panoramic images are not sufficient for accurate assessment of the lingual concavity. The most detailed radiographic evaluation is made by three-dimensional imaging. The Cone Beam Computerized Tomography (CBCT) cross-sections have the highest spatial resolution and lowest cost and radiation exposure for assessment of bony structures (18). So this molality was used in the present study.
Until now, most studies on lingual concavity have evaluated the ridge according to the former classification (concave, parallel, convex). This classification lacks information regarding the deep concavities, which are the major risk for perforation. To the best of our knowledge, only one study classified the concave lingual cortex into three types (16,17). Therefore, the present study aimed to broaden our knowledge regarding the deep and risky types of lingual concavity in the posterior mandible with the new classification to reduce surgical complications in this region.
Material and Methods
This study was approved by the institutional Ethical Committee (protocol number IR.SUMS.DENTAL.REC.1399.110).
In this cross-sectional study, we evaluated the archive of CBCT images of patients referring to the Radiology department, between January 2018 to May 2022, which were taken for purposes other than the present study. The study included high-quality imaging with the field of view of the entire mandible. The exclusion criteria were subjects with a previous history of surgery or pathologic lesions in their mandible, subjects with a clear radiographic clue for bone abnormality, and images with misinterpreting artifacts due to extensive restorations. Finally, we selected 335 high-quality images for further assessment. All patients signed a written consent that their anonymous data could be used in future research.
All images were prepared with a New Tom VGI Evo CBCT machine (Verona, Italy). The exposure factors were set according to the patient’s size, with a resolution of 0.3 mm. NNT viewer performed images reconstruction with a thickness and interval of 0.5 mm. Images were assessed in three orthogonal plans by a maxillofacial radiologist in standard viewing conditions. Thirty percent of images were re-observed two weeks later to determine intra-observer agreement. Twenty percent of images were randomly selected for re-assessment two weeks later by another oral and maxillofacial radiologist, separately. In order to quantitatively assess the inter-observer reliability of the outcomes, Kappa coefficient was estimated for each variable. Cross-sectional mandibular images were reconstructed at edentulous region of the molar area, adjacent to the external oblique ridge on both sides.
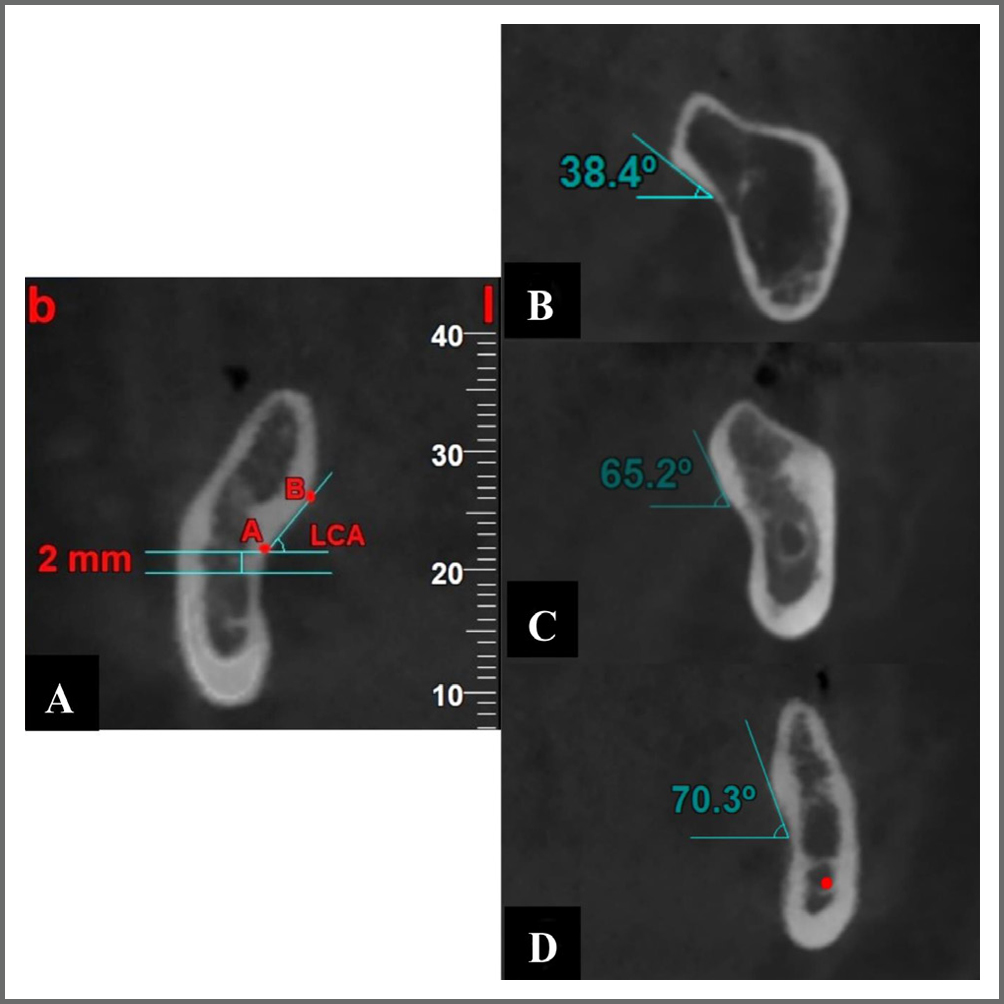
First, two horizontal lines were drawn. The first line was tangent to the superior boundary of the inferior alveolar nerve canal, and the second line was drawn parallel and 2 mm superior to the first line. The intersection of this second line with the lingual aspect of the mandible was designated as point A. The outermost point of the mandible’s lingual aspect was named point B. Then a line was drawn connecting point A to point B. The angle formed between this connecting line and the horizontal line was determined as the Lingual Concavity Angle (LCA) (Figure 1A). Based on the magnitude of this angle, the subjects were divided into two main groups. The subjects with LCA greater than 85° were the non-concave group, and the ones with LCA smaller than 85° were the concave group. The concave group was classified into three subgroups: Group 1: the angle less than 40° (Figure 1B), Group 2: the angle between 40-60° (Figure 1C), Group 3: and angle between 60-85° (Figure 1D) were designated as extremely deep, deep, and mild deep, respectively.
We compared the LCA between the two genders and between the two sides. Also, we compared the frequency of different types of lingual concavity between the two genders and between the two sides. Additionally, the relationship between the age of the participants and LCA and also the relationship between the age and different groups of lingual concavity were evaluated.
SPSS software version 22 (SPSS, Chicago, IL, USA) was used for statistical analysis. The Pearson Chi-square test was used to compare the frequency of different types of lingual concavity between the two genders and between the two sides. For comparison of the LCA between the two genders and between the two sides, the independent t-test and paired t-test were used, respectively. The spearman’s rank correlation coefficient was applied to assess the relationship between the LCA and age of participants, and the Kruskal-Wallis and Dunn’s posthoc for comparison of the age of participants in different groups of lingual concavity. p-values <0.05 were considered statistically significant.
Results
No statistically meaningful difference was found between the data gathered by the two measurements. Thus, the double measurements mean was used for analysis. The significant reliability of the double measurements was proved because the Intra Class Correlation Coefficient (ICC) of the two assessments was >0.9. Furthermore, ICC indicated essential concurrence between the two spectators.
In this descriptive-analytic study, 335 participants, 222 females (mean age 35.32±3.34 years) and 113 males (mean age of 36.31±2.63 years), participated in the study. The frequency of different types of lingual concavity is depicted in table 1. The most common type of lingual concavity was mild deep (58.5%), followed by deep (34.62%), and the least common type was extremely deep (2.38%).
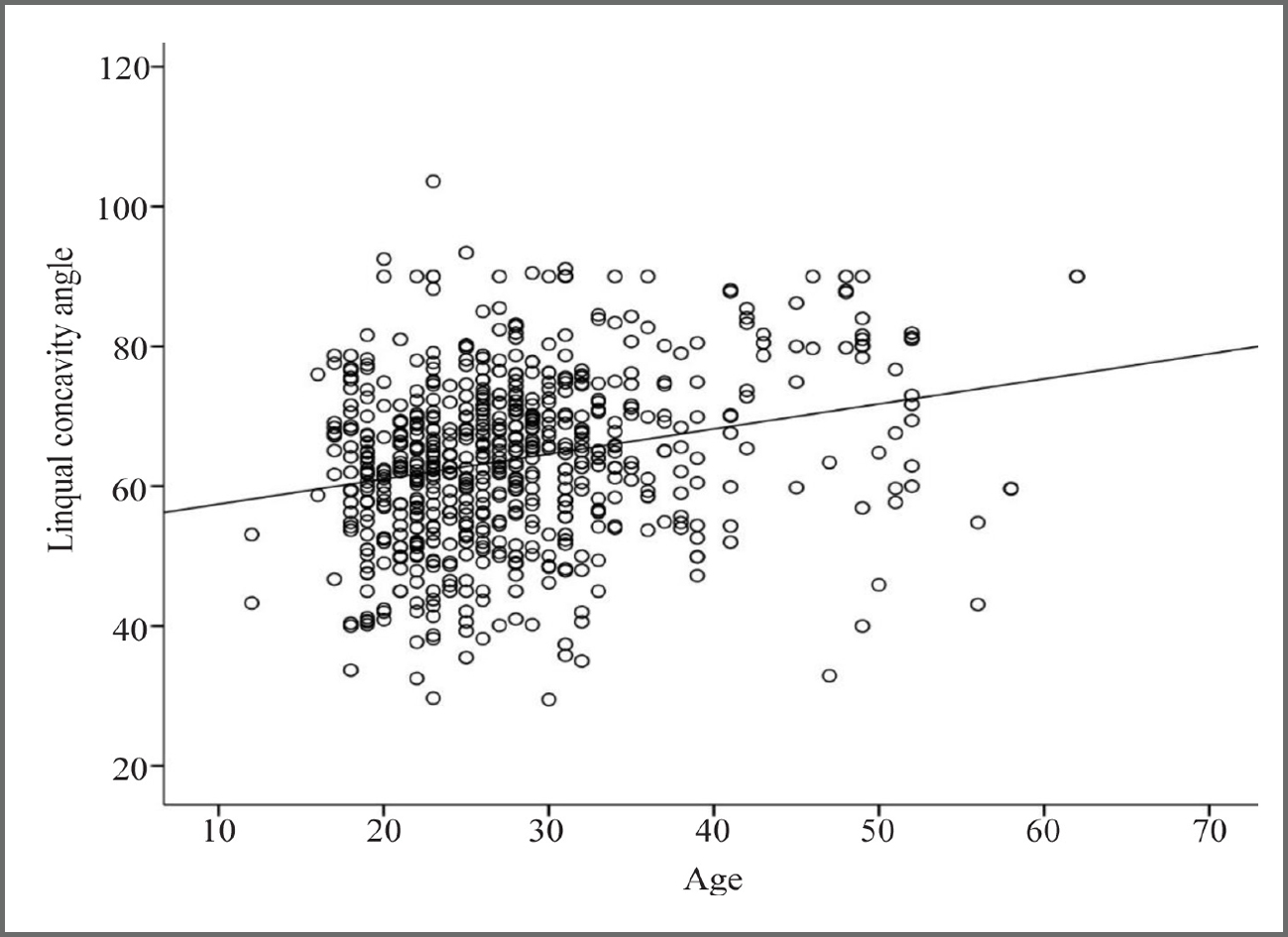
There was a significant positive correlation between the LCA and the age of participants (p-value <0.001, Correlation coefficient=0.50). The LCA increased 0.226 degree per year (Figure 2). There was also significant relationship between the age of participants and the type of lingual concavity (p-value <0.001). The subjects in mild deep group were significantly older than deep group (p-value=0.032). Also, the non-concave subjects were significantly older than deep and mild deep subjects (p-value=0.001 and 0.040, respectively) (Table 2).
Table 3 depicts the comparison of LCA between the two genders. As shown, the LCA was significantly higher in males than females (p-value=0.020). However, there was no significant difference between the two genders in different groups of lingual concavity (p-value=0.242).
The LCA was significantly larger on the left side (p-value<0.001). Also, the deep and mild deep groups were significantly different between the two sides (p-value=0.000 and 0.012, respectively) (Table 4).
Table 1. Distribution of different types of lingual concavity
|
|
Number |
Percentage |
|
1 |
8 |
2.38% |
|
2 |
116 |
34.62% |
|
3 |
196 |
58.50% |
|
Non-concave |
15 |
4.47% |
Table 2. Comparison of age between different groups of lingual concavity
|
|
Age |
||
|
Mean±SD |
p-value |
||
|
Groups of lingual concavity |
1 |
27.81±8.98 |
p total <0.001 |
|
2 |
26.77±7.92 |
P2-3 =0.032 |
|
|
3 |
28.24±7.83 |
P2-4 =0.001 |
|
|
4* |
34.70±12.03 |
P3-4 =0.044 |
|
Kruskal-Wallis and Dunn’s posthoc, *4 is determined as the non-concave group.
Table 3. Comparison of lingual concavity angle and frequency of different groups between the two genders
|
|
Sex |
p-value |
||
|
|
Females Mean ± SD |
Males Mean ± SD |
||
|
Lingual concavity angle |
63.11±11.79 |
65.43±12.75 |
0.020 a* |
|
|
Frequency of lingual concavity types |
1 |
2.70% |
1.8% |
0.242 b** |
|
2 |
34.90% |
34.1% |
||
|
3 |
59.0% |
57.5% |
||
|
Non-concave |
3.40% |
6.6% |
||
*a independent t test, **b pearson chi square test.
Table 4. Comparison of lingual concavity angle and frequency of different groups between the two sides
|
|
Side |
p-value |
||
|
Right Mean ± SD |
Left Mean ± SD |
|||
|
Lingual concavity angle |
61.57±12.26 |
66.21±11.62 |
<0.001 |
|
|
Frequency of lingual concavity types |
1 |
1.3% |
1% |
0.617 |
|
2 |
21.3% |
13.3% |
0.000 * |
|
|
3 |
25.5% |
33% |
0.012 * |
|
|
Non-concave |
1.8% |
2.7% |
0.273 |
|
Discussion
With an increase in the use of implants for the replacement of missed teeth, surgical anatomic limitations have been disclosed more. In the posterior region of the mandible, which is at high risk for tooth loss due to the early eruption of the first molar tooth, a significant anatomic limitation is lingual concavity. The deeper the lingual concavity, the higher the risk of lingual cortex perforation. As perforation of this cortex during surgery leads to severe complications for the patient, it is essential to increase our knowledge regarding the different types of lingual concavity with a standard assessment protocol.
In the present study, the frequency of the different types of lingual concavity was approximately 95%. Based on the standard protocol of assessment, the presence of deep lingual concavity was common. This justifies great caution during surgical operations in this region. Also, the most and the least common types were mild deep and extremely deep, respectively. Although the extremely deep lingual concavity was the least frequent type (2.38%) due to the life-threatening danger of lingual cortex perforation in this type, the presurgical prescription of 3D examination of this region is highly recommended. Therefore, it is suggested that oral and maxillofacial radiologists report the angle and type of lingual concavity in the posterior region of the mandible. This will increasingly reduce the time spent by the surgeon for determining the angulation and position of implant insertion. These results were in accordance with the findings of Bodart L et al (16). They reported the frequency of lingual concavity as about 93%, and the frequency of different types was as follows: mild deep>deep> extremely deep, which is the same as the current study. Other studies on this issue were conducted with different protocols and could not be compared with the present study.
The results of the present study revealed a significant positive correlation between the LCA and the age of the subjects. With each year of aging, the LCA increased by 0.226 degrees. Also, we found that the subjects with the mild deep type of lingual concavity were older than those with the deep type. Additionally, the non-concave form of lingual concavity was significantly more frequent in older participants. The possible explanation for this finding would be the widely accepted notion that the concavity of the lingual aspect of the alveolar ridge decreases during life as the height of the ridge reduces and atrophic alterations occur with aging (7,15,19,20). This finding coincides with study of Kamburoğlu K et al (15) which revealed a correlation between the lingual concavity indicators and age of the participants. Although, Bodart L et al (16) found no significant relationship between the concavity angle and the age of the participants.
In the present study, the LCA was significantly larger in males than in females. Comparing the frequency of the different types of lingual concavity between the two genders, all types were more frequent in females than males. Also, the non-concave lingual cortex was more prevalent in males. The results in groups were not statistically significant. Generally, it can be concluded that women are more prone to concave lingual cortex and its possible surgical complications. This is in line with Bayrak S et al (21), Zhang W et al (22) and Braut V et al (17) studies who believed that women are more susceptible to surgical complications due to their smaller jaws. Although, Bodart L et al (16), Quirynen M et al (23). Parnia F et al (8), and Rajput BS et al (24) reported no significant correlation between gender and LCA. This can be attributed to the different measurement protocols of different studies, ethnic diversities and differences in sample sizes.
The LCA was significantly higher on the left than on the right. Also, comparing the frequency of different types of lingual concavity between the two sides, it was found that the frequency of the types of mild deep and deep lingual concavity was significantly different between the two sides. Insignificancy of this result in the extremely deep type of lingual concavity may be related to the low frequency of this group.
This result aligns with the study of Tan WY et al (19), who reported a significant difference in lingual concavity depth between the two sides. They interpreted that this is due to the submandibular gland size difference between the two sides. Regarding the diversity in the anatomic features of jaws of different ethnicities, further studies in other ethnicities regarding the lingual concavity of the posterior of the mandible with this standard assessment protocol is recommended.
Conclusion
Based on the standard assessment protocol, different types of deep lingual concavity were highly frequent. Therefore, a detailed CBCT image analysis of concavity morphology should be included as part of pre-operative implant planning in order to avoid complications such as lingual plate perforation, hemorrhage and nerve injury. Mandibular lingual concavity types were found to vary by age, and laterality. LCA was also significantly different according to patient age, sex, and laterality.
Funding
The authors would like to thank the Vice Chancellor for Research, Shiraz University of Medical Science for supporting this investigation.
Ethics approval and consent to participate
The protocol of current study was approved by the Ethical committee of Shiraz University of Medical sciences (protocol number IR.SUMS.DENTAL.REC.1399.110).
Acknowledgement
The authors thank the Vice-Chancellery Research of Shiraz University of Medical Sciences for supporting this research. The protocol of current study was approved by the Ethical committee of Shiraz University of Medical sciences (protocol number IR.SUMS.DENTAL.REC.1399.110).
Conflict of Interest
The authors declare that they have no conflict of interest.
J Prosthet Dent 2021 May;125(5):766.e1-766.e8. https://pubmed.ncbi.nlm.nih.gov/33752904/