Document Type : Original article
Abstract
Background: While numerous studies have explored sociodemo- graphic disparities in accessing maternity care in Pakistan, there remains a paucity of knowledge regarding the continuum of maternity care and the unequal access between urban and rural areas in the country. Thus, this study aimed to bridge this gap.
Methods: We performed a secondary analysis using data from the Pakistan Demographic Health Survey (2017-18), stratifying by urban and rural residents. Poisson regression was employed to discern the sociodemographic factors associated with three crucial aspects of maternity care: adequate antenatal care (ANC), skilled birth attendance (SBA), and postnatal care (PNC), as well as the completion of the continuum of care (CoC). Additionally, path analysis estimated the relationship between adequate ANC, SBA, and PNC along the pathway of ongoing maternity care.
Results: The results indicated higher education, wealth, living in ICT region, mobile phone ownership, internet use, TV viewership, and newspaper reading increased the likelihood of receiving ANC, SBA, PNC, and completing CoC. Conversely, higher parity, living in Baluchistan/FATA regions decreased the likelihood of receiving ANC, SBA, PNC, and completing CoC. Adequate ANC increased the likelihood of SBA, PNC, and completing CoC. However, SBA did not impact PNC along the care pathway.
Conclusion: Regardless of place of residence, higher levels of education and wealth, as well as access to mass media, were found to be the most significant determinants of receiving adequate ANC, SBA, PNC, and completing CoC and should be prioritized in future policy making in Pakistan to enhance the maternal and child health.
Keywords: Continuity of Patient Care, Maternal Health Services, Prenatal Care, Postnatal Care, Pakistan
Introduction
Despite the remarkable progress attained in reducing maternal mortality during the Millennium Development Goals (MDGs) era (1); yet, maternal health remains a key focus of the 3rd Sustainable Development Goal (SDG) due to its persistent burden. The UN set the target to reduce maternal mortality below 70 per 100,000 live births by 2030 (2). Globally, South Asia has the second-highest Maternal Mortality Rate (MMR) after Sub-Saharan Africa. According to the latest UN data from 2017, Afghanistan (638/100000 live births), Bangladesh (173/100000 live births), India (143/100000 live births), and Pakistan (140/100000 live births) had the highest MMR in the region (3). However, the latest statistics from Pakistan indicate a 32% increase from 2017 to 2019 (from 140 to 186 per 100,000 live births), which is of great concern and calls for more research to inform the policies and interventions (4). That said, Pakistan not only failed to achieve the MDG 5 to reduce maternal and neonatal mortality by 2015 but is also far behind achieving SDG 3 by 2030.
Continuum of Care (CoC) is defined as the linkage between essential care across the pregnancy, delivery, and postpartum stages (5). These include, but are not limited to, adequate Antenatal Care (ANC), having a Skilled Birth Attendant (SBA), and Postnatal Care (PNC) (6), and ensure early detection and management of adverse complications (7). The key to an efficient CoC is continuity of care along the three critical stages of pregnancy, delivery, and postnatal, and failure to provide appropriate care at any stage could lead to unfavorable outcomes (8,9). CoC could also foster the continuity of care in later life during childhood and adolescence, reducing the likelihood of maternal and child morbidity and mortality (10).
Despite the remarkable improvement in MMR since the year 2000, the observed increase (32%) in 2019 has alarming implications for future policy and research (11). Additionally, a recent survey in 2019 revealed an estimated 26% higher MMR in the rural population compared to the urban in Pakistan (12). This disparity has been attributed to the significant gap in access to health services between rural population and those living in remote areas (12). Nonetheless, there is also a gap in the utilization of maternity services in areas with adequate access to healthcare services and limited knowledge exists about the underlying sociodemographic drivers of such differential uptake among Pakistani women (13). That said; stratified by place of living (urban/rural), this study aimed to explore the sociodemographic factors that are associated with adequate ANC, SBA, and PNC, and more importantly, determine the proportion and characteristics of Pakistani women who have completed CoC. Although several studies have addressed the sociodemographic inequalities in accessing maternity care in Pakistan, none explored it from the perspective of a continuum of care (14-16) nor considered the disproportionate access to maternity care in urban and rural areas (17,18). Additionally, the rise in the MMR observed from 2017 to 2019 calls for more research into underlying drivers of such trends to identify the vulnerable population, address the root reasons, and formulate targeted and well-tailored interventions to reduce the MMR and strive to achieve the SDGs 3 by 2030.
Materials and Methods
Study setting
This study used the data from the latest Pakistan Demographic Health Survey (PDHS), which was conducted in 2017-18. PDHS 2017-18 is a nationally representative survey carried out by the Pakistan National Institute of Population Studies and the ICF International funded by the United States Agency for International Development (USAID). The survey encompassed four provinces (Punjab, Sindh, Khyber Pakhtunkhwa, Baluchistan); Azad Jammu & Kashmir (AJK) and Gilgit Baltistan (GB); Islamabad Capital Territory (ICT); and the former Federally Administrated Tribal Areas (FATA) in Pakistan.
Study design and population
Through a two-stage stratified cluster sampling, PDHS 2017-18 collected data for women aged 15-49 years to estimate the key indicators at the national and regional levels across urban and rural areas. In the first stage, 580 clusters (enumeration areas from the previous national census) were selected. In the second stage, 16,240 households were selected within 580 clusters through an equal probability systematic selection process. Sampling weights were calculated and applied to obtain representative estimates at the national and regional levels. A sample of the women aged 15-49 years (n=15930) who were either permanent residents of the selected households or visitors who stayed in the households the night before the survey were enlisted, out of them 15,068 women were successfully interviewed with a response rate of 94.6%. More details could be found in the PDHS 2017-18 final report (19). For the present study, we included all the women aged 15-49 years old who were either married or formerly married, answered the questions concerning ANC, SBA, and PNC for their last pregnancy, and living in Punjab, Sindh, Baluchistan, Khyber Pakhtunkhwa (KPK), Islamabad Capital Territory (ICT), and FATA regions.
Study variables
Sociodemographic variables
The sociodemographic factors that are believed to influence access to and utilization of maternity care among women (14,20-22) were extracted from the database. This includes age (year), education (no education, primary, secondary, higher), employment (yes, no), wealth index (poorest, poorer, middle, richer, richest), parity (0, 1, 2-4, ≥5), place of living (rural, urban), region (Punjab, Sindh, KPK, ICT, FATA), husband’s education (no education, primary, secondary, higher), owning a mobile phone (yes, no), using the internet (yes, no), frequency of watching TV or reading newspaper (never, less than once a week, more than once a week).
Outcome variables
a) Adequate antenatal care
The World Health Organization (WHO) recommends a minimum of four antenatal care (ANC) visits for optimal pregnancy outcomes. Therefore, adequate ANC was defined as having at least four antenatal visits.
b) Skilled birth attendance
This variable was defined as delivery by skilled health workers including a doctor, nurse, midwife, lady health visitor, and community midwife, and was coded “yes=1” and “no=0”.
c) Postnatal care
This variable was defined and coded as “1” if the mother and newborn received a postpartum visit within two months after birth and if not, it was coded “0”.
d) Continuum of care (CoC)
This variable was defined as completion of adequate ANC, SBA, and PNC across the continuum of maternity care and was coded “yes=1” and “no=0”
Data analysis
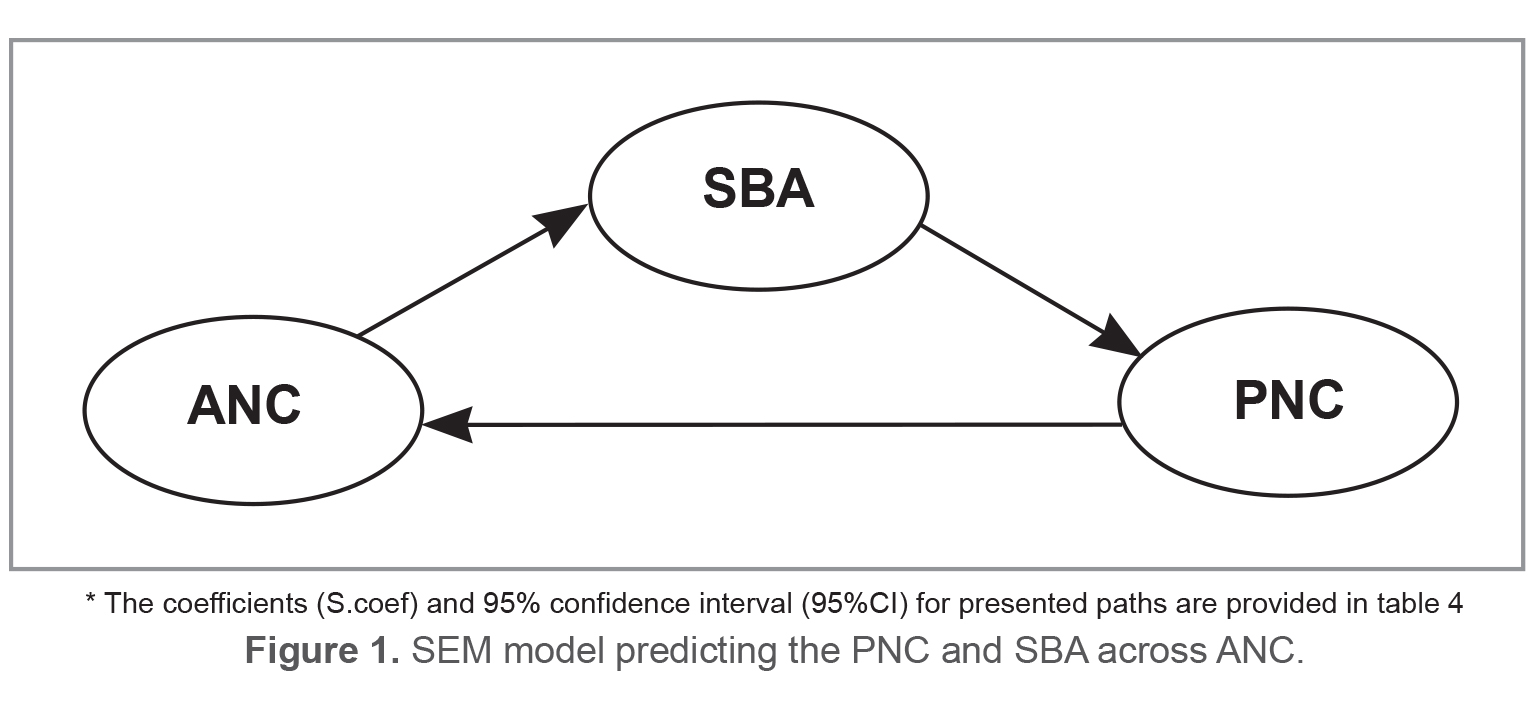
Descriptive statistics were utilized to characterize the sociodemographic profile of Pakistani women aged 15-49 years (Table 1). The chi-square test was employed to compare the prevalence rates of adequate ANC, SBA, PNC, and completed CoC between rural and urban areas (Table 2), stratified by place of living (rural/urban). Given the high prevalence of outcomes observed in our study, Poisson regression with robust variance was deemed more suitable for analyzing cross-sectional studies with binary outcomes compared to logistic regression. Poisson regression offers more accurate estimates and facilitates easier interpretation and communication of results, particularly with non-specialist audiences, using the prevalence ratio instead of the odds ratio (23). Hence, Poisson regression was employed to investigate the association between sociodemographic characteristics with adequate ANC, SBA, PNC, and completed CoC (Table 3). Results were presented in terms of prevalence Rate Ratio (PRR) and 95% confidence interval (95%CI). Path analysis, reporting the standardized path coefficients, was used to examine the association between adequate ANC, SBA, and PNC across the continuum of maternity care (Figure 1). All analyses were performed using STATA 16, with the statistically significance set at p-value <0.05.
Ethics considerations
DHS conforms to the U.S. Department of Health and Human Services regulations for the protection of human subjects (45 CFR 46). In addition, this survey was approved by the Institutional Review Board (IRB) of the Pakistan Ministry of Health (MoH) all methods were performed in accordance with the relevant guidelines and regulations. Informed verbal and written consent were obtained from all the participants/guardians/parents before the interview. We also sought permission from the DHS website and filled out a request to access and download the data. Therefore, further ethical approval to use the data is not necessary.
Results
Sociodemographic characteristics of Pakistani women aged 15-49 years
The majority of participants fell within the middle age groups, between 25 to 39 years old. Nearly half of the women and less than a third of their husbands had no education. Less than a fifth of women were employed at the time of the interview. There were more or less equal numbers of women in each wealth index class, accounting for 20% of the total population. Only 13.44% of women had no pregnancy experience. Approximately two-thirds of the participants resided in rural areas. The majority of women were living in Punjab, Sindh, and KPK regions. Nearly 40% of them owned a mobile phone; while internet access was reported by only 12.61%. Almost half of them were watching TV at least once a week and only a small proportion read the newspaper (14.22%).
Prevalence of adequate ANC, SBA, PNC, and completion of CoC across urban and rural areas
As table 2 indicates; having adequate ANC, SBA, and PNC were significantly higher in urban areas; respectively 85.90, 85.24, and 36.90%, as compared to rural areas; respectively 66.87, 65.34, and 27.65%, in Pakistan. The rate of CoC in urban areas (25.31%) almost doubled the rate in rural areas (11.40%).
Sociodemographic determinants of adequate ANC, SBA, PNC, and completion of CoC
Table 3 illustrated the association between different sociodemographic characteristics and adequate ANC, SBA, PNC, and completion of CoC among Pakistani women aged 15-49. Generally, women in older age groups (>35 years) were more likely to have adequate ANC compared to the youngest age group (15-24 years) in both urban and rural areas. Conversely, older age groups (>35 years) had significantly lower rates of SBA compared to the youngest in rural areas. However, age was not a significant predictor for SBA in urban areas.
Consistently across urban and rural areas, higher education for both women and husbands were associated with a higher likelihood of adequate ANC, SBA, PNC, and completion of CoC except for husbands’ education for PNC. Respectively in urban and rural areas, the likelihood of completion of CoC was 2.65 and 3.94 times higher among women with higher education compared to those with no education (Table 3). A similar trend was observed for husband education, with the odds of completion of CoC being 2.42 and 3.10 times higher among the wives of higher-educated husbands in urban and rural areas, respectively.
Except for SBA (PRR= 0.87, 95%CI: 0.78-0.96) and PNC (PRR= 1.41, 95%CI: 1.21-1.64) in rural areas, employment was not associated with any outcome. However, except for PNC, in both urban and rural areas, the likelihood of other outcomes‒adequate ANC and SBA‒was significantly higher among the women from wealthier classes as compared to the poorest class. Urban and rural women from the richest class, respectively, were 3.46 and 4 times more likely to complete CoC compared to those from the poorest class.
In both rural and urban areas, women with higher parity were less likely to have adequate ANC, SBA, and PNC. Likewise, the likelihood of completing CoC in urban and rural areas, respectively, was 49% and 64% lower among women with ≥4 pregnancy experiences compared to those with a history of one pregnancy (PRR=0.51, 95%CI: 0.35-0.74 for urban and PRR=0.36, 95%CI: 0.24-0.56 for rural).
Overall, in both urban and rural areas, women residing in Baluchistan and FATA regions had the lowest likelihood, while those living in the ICT region had the highest likelihood of adequate ANC, SBA, PNC, and completion of CoC compared to the reference group (those living in Punjab). Except for PNC in rural areas, all women owning a mobile phone were more likely to have adequate ANC, SBA, PNC, and completed CoC (Table 3). Similarly, all women with access to the internet, regardless of the place of residence, were more likely to have adequate ANC, SBA, PNC, and completion of CoC (Table 3).
Table 1. Sociodemographic characteristics of women aged 15-49 in Pakistan, PDHS 2017-18
|
Age groups(yr) |
N(weighted%) |
|
15-24 |
2522(20.13) |
|
25-29 |
2591(20.61) |
|
30-34 |
2310(19.52) |
|
35-39 |
2213(17.49) |
|
40-44 |
1468(11.62) |
|
45-49 |
1260(10.64) |
|
Education |
|
|
No education |
6682(49.18) |
|
Primary |
1693(16.47) |
|
Secondary |
2307(21.21) |
|
Higher |
1682(13.14) |
|
Employment |
|
|
Yes |
1765(17.28) |
|
No |
10597(82.72) |
|
Wealth index |
|
|
Poorest |
2406(18.26) |
|
Poorer |
2451(19.65) |
|
Middle |
2310(20.25) |
|
Richer |
2441(20.98) |
|
Richest |
2756(20.86) |
|
Parity |
|
|
Nullipara |
1595(13.44) |
|
1-3 |
5496(43.98) |
|
>=4 |
5273(42.59) |
|
Husband’s Education |
|
|
No education |
3584(29.50) |
|
Primary |
1596(15.60) |
|
Secondary |
3908(35.31) |
|
Higher |
2783(19.59) |
|
Place of living |
|
|
Urban |
6098(36.80) |
|
Rural |
6266(63.20) |
|
Region |
|
|
Punjab |
3400(53.62) |
|
Sindh |
2739(23.05) |
|
KPK |
2378(15.37) |
|
Baluchistan |
1724(5.19) |
|
ICT |
1111(0.87) |
|
FATA |
1012(1.89) |
|
Own a mobile phone |
4831(39.18) |
|
Use internet |
1563(12.61) |
|
Frequency of watching TV |
|
|
Not at all |
5229(37.68) |
|
Less than once a week |
1284(11.74) |
|
At least once a week |
5850(50.58) |
|
Frequency of reading newspaper |
|
|
Not at all |
12481(85.78) |
|
Less than once a week |
1655(9.13) |
|
At least once a week |
922(5.09) |
Table 2. The prevalence of adequate ANC, SBA, PNC, and completed CoC, stratified by place of living
|
|
Urban |
Rural |
p-value |
|
ANC≥4 |
4916(85.90) |
3998(66.87) |
0.001 |
|
SBA |
2539(85.24) |
2225(65.34) |
0.001 |
|
PNC |
948(36.90) |
868(27.65) |
0.001 |
|
CoC |
617(25.31) |
366(11.40) |
0.001 |
Adequate antenatal Care (ANC), Skilled Birth Attendance (SBA), Post Natal Care (PNC), Continuum of Care (CoC).
Table 3. Sociodemographic determinants of adequate ANC, SBA, PNC, and Completed CoC; PDHS 2017-18
|
|
Adequate ANC |
SBA |
||
|
|
Urban |
Rural |
Urban |
Rural |
|
|
PRR (95%CI) |
PRR (95%CI) |
PRR (95%CI) |
PRR (95%CI) |
|
Age groups |
|
|
|
|
|
15-24 |
Ref |
Ref |
Ref |
Ref |
|
25-29 |
1.03(0.97-1.09) |
0.86(0.79-0.93)* |
1.09(1.02-1.15)* |
0.92(0.85-0.99)* |
|
30-34 |
1.05(0.99-1.12) |
0.92(0.85-1.00)) |
1.05(0.98-1.13) |
0.92(0.85-1.01) |
|
35-39 |
1.11(1.04-1.18)* |
1.06(0.98-1.14) |
1.06(0.99-1.13) |
0.84(0.76-0.92)* |
|
40-44 |
1.22(1.15-1.29)* |
1.30(1.21-1.40)* |
1.01(0.91-1.12) |
0.80(0.68-0.94)* |
|
45-49 |
1.25(1.18-1.32)* |
1.41(1.32-1.52)* |
0.96(0.74-1.25) |
0.62(0.43-0.89)* |
|
Education |
|
|
|
|
|
No education |
Ref |
Ref |
Ref |
Ref |
|
Primary |
1.12(1.07-1.18)* |
1.13(1.05-1.21)* |
1.27(1.16-1.39)* |
1.22(1.11-1.34)* |
|
Secondary |
1.16(1.11-1.22)* |
1.29(1.21-1.38)* |
1.30(1.20-1.42)* |
1.42(1.30-1.56)* |
|
Higher |
1.26(1.21-1.31)* |
1.43(1.34-1.52)* |
1.43(1.32-1.54)* |
1.65(1.51-1.80)* |
|
Employment |
|
|
|
|
|
Yes |
1.00(0.96-1.04) |
1.04(0.98-1.10) |
0.96(0.88-1.05) |
0.87(0.78-0.96)* |
|
No |
Ref |
Ref |
Ref |
Ref |
|
Wealth index |
|
|
|
|
|
Poorest |
Ref |
Ref |
Ref |
Ref |
|
Poorer |
1.17(0.99-1.39) |
1.29(1.17-1.42)* |
1.19(0.82-1.73) |
1.15(1.01-1.30)* |
|
Middle |
1.32(1.11-1.57)* |
1.42(1.30-1.55)* |
1.45(0.99-2.13) |
1.43(1.26-1.63)* |
|
Richer |
1.51(1.26-1.81)* |
1.60(1.47-1.74)* |
1.62(1.11-2.38)* |
1.64(1.43-1.88)* |
|
Richest |
1.64(1.37-1.96)* |
1.84(1.69-1.99)* |
1.74(1.19-2.55)* |
1.88(1.66-2.12)* |
|
Parity |
|
|
|
|
|
Nullipara |
Ref |
Ref |
Excluded |
Excluded |
|
1 |
0.87(0.83-0.91)* |
0.62(0.57-0.68)* |
Ref |
Ref |
|
1-3 |
0.84(0.81-0.86)* |
0.60(0.56-0.64)* |
0.97(0.93-1.01) |
0.84(0.79-0.90)* |
|
>=4 |
0.83(0.79-0.86)* |
0.63(0.60-0.66)* |
0.81(0.74-0.89)* |
0.68(0.63-0.75)* |
|
Husband’s Education |
|
|
|
|
|
No education |
Ref |
Ref |
Ref |
Ref |
|
Primary |
0.99(0.92-1.06) |
1.07(0.99-1.15) |
0.99(0.90-1.10) |
1.14(1.03-1.26)* |
|
Secondary |
1.15(1.09-1.21)* |
1.21(1.14-1.29)* |
1.20(1.11-1.29)* |
1.31(1.21-1.43)* |
|
Higher |
1.22(1.16-1.28)* |
1.32(1.24-1.40)* |
1.28(1.18-1.38)* |
1.53(1.40-1.67)* |
|
Region |
|
|
|
|
|
Punjab |
Ref |
Ref |
Ref |
Ref |
|
Sindh |
1.02(0.98-1.07) |
0.81(0.74-0.89)* |
1.07(1.00-1.14) |
0.96(0.85-1.10) |
|
KPK |
0.90(0.84-0.96)* |
0.92(0.83-1.01) |
0.95(0.86-1.04) |
0.94(0.82-1.08) |
|
Baluchistan |
0.73(0.66-0.81)* |
0.72(0.61-0.84)* |
0.73(0.61-0.86)* |
0.41(0.29-0.57)* |
|
ICT |
1.03(0.98-1.09) |
1.26(1.18-1.35)* |
1.01(0.92-1.10) |
1.30(1.16-1.45)* |
|
FATA |
0.72(0.59-0.89)* |
0.69(0.61-0.78)* |
1.11(1.04-1.18)* |
0.77(0.63-0.93)* |
|
Own a mobile phone |
|
|
|
|
|
No |
Ref |
Ref |
Ref |
Ref |
|
Yes |
1.15(1.12-1.19)* |
1.24(1.18-1.32)* |
1.14(1.08-1.20)* |
1.31(1.22-1.41)* |
|
Use internet |
|
|
|
|
|
No |
Ref |
Ref |
Ref |
Ref |
|
Yes |
1.14(1.11-1.17)* |
1.40(1.31-1.48)* |
1.17(1.12-1.22)* |
1.46(1.35-1.57)* |
|
% of watching TV |
|
|
|
|
|
Not at all |
Ref |
Ref |
Ref |
Ref |
|
Less than once a week |
1.06(1.00-1.13)* |
1.25(1.17-1.34)* |
1.10(1.00-1.21) |
1.30(1.15-1.47)* |
|
At least once a week |
1.13(1.08-1.18)* |
1.28(1.21-1.36)* |
1.18(1.10-1.26)* |
1.33(1.22-1.45)* |
|
% of reading newspaper |
|
|
|
|
|
Not at all |
Ref |
Ref |
Ref |
Ref |
|
Less than once a week |
1.07(1.03-1.11)* |
1.26(1.18-1.36)* |
1.10(1.04-1.16)* |
1.32(1.20-1.44)* |
|
At least once a week |
1.07(1.02-1.12)* |
1.29(1.18-1.40)* |
1.16(1.11-1.22)* |
1.38(1.24-1.53)* |
Adequate antenatal Care (ANC), Skilled Birth Attendance (SBA), Post Natal Care (PNC), Continuum of Care (CoC), Prevalence Rate Ratio (PRR).
Table 4. Standardized path coefficients (S.coef) and 95% confidence interval (95%CI) for relationships between adequate ANC, SBA, and PNC along the continuum of maternity care, by place of living
|
|
Urban |
Rural |
||
|
|
S.coef(95%CI) |
p-value |
S.coef(95%CI) |
p-value |
|
ANC>SBA |
0.29(0.27-0.33) |
0.001 |
0.36(0.33-0.39) |
0.001 |
|
ANC>PNC* |
0.15(0.12-0.19) |
0.001 |
0.12(0.10-0.15) |
0.001 |
|
SBA>PNC |
0.02(-0.07-0.01) |
0.138 |
0.02(-0.01-0.16) |
0.273 |
* In SEM analysis, only 7 % and 5% of the total effect of ANC on PNC is mediated by SBA in urban and rural areas, respectively.
Consistently across urban and rural areas, watching TV at least once a week or more was strongly associated with adequate ANC, SBA, PNC, and completion of CoC compared to those who never watch TV. Moreover, aside from PNC; in both urban and rural areas, the likelihood of having adequate ANC, SBA, PNC, and completing CoC was significantly higher among the women who read newspapers‒regardless of the frequency of reading‒ compared to those who do not read.
Relationship between adequate ANC, SBA, and PNC along the pathway of continuum maternity care
As is presented in table 4, consistently across urban and rural areas, having adequate ANC was significantly associated with having SBA (s.coef: 0.29, p-value=0.001 for urban and s.coef: 0.36, p-value=0.001 for rural) and PNC (s.coef: 0.15, p-value=0.001 for urban and s.coef: 0.12, p-value=0.001 for rural). however, having SBA was not a significant predictor of having PNC (p-value>0.05).
Discussion
Continuum of care plays a critical role in enhancing maternal and child health outcomes. It necessitates a well-connected delivery of service across three main components of maternal care‒antenatal, delivery, and postnatal services‒of standard quality (24). Therefore, understanding the underlying factors contributing to disparities in accessing or utilizing maternity care services along the continuum of care is of paramount importance. To the best of our knowledge, this is one the first studies that explored and determined the associated sociodemographic factors of accessing and completing maternity care‒adequate ANC, SBA, PNC, and completed CoC‒ among Pakistani women aged 15-49 years across urban and rural areas. Additionally, the study explores the interrelationship between the three key components of maternity care—adequate ANC, SBA, and PNC—along the continuum of care, postulating that receiving adequate ANC is linked with having SBA and PNC as part of the ongoing maternity care pathway.
The results showed that higher education and wealth, residence in the ICT region, ownership of a mobile phone, internet usage, TV watching, and newspapers reading are positively associated with adequate ANC, SBA, PNC, and completion of CoC among Pakistani women. On the other hand, factors such as higher parity, and residing in Baluchistan and FATA regions are associated with decrease likelihood of having adequate ANC, SBA, PNC, and completing the CoC. Additionally, women with adequate ANC are more likely to have SBA and PNC in later stages and complete the CoC. However, having SBA was not associated with having PNC along the pathway of ongoing maternity care.
Several studies have suggested that higher women’s education correlates with improved maternal health-seeking behavior (25,26). This has been attributed to enhanced information processing abilities through improved cognition skills‒literacy and numeracy‒acquiring during schooling (27). Moreover, the acquisition of health knowledge continues throughout life, facilitated by ongoing improvements in literacy and numeracy skills (28). Education also has the potential to shift women’s roles within the family, granting them greater autonomy and bargaining power in matters related to reproduction and maternity rights (29). Besides, higher levels of education offer more job opportunities and income, further empowering women and improving their access to maternity and reproductive health services (30). We observed higher rates of adequate ANC, SBA, PNC, and completed CoC among the women of higher education, regardless of living place, in this study. Importantly, the impact of education on maternity care access and utilization appears to be more pronounced in rural areas, underscoring the critical role of schooling in enhancing these aspects of maternal health. This effect is attributed to improved health literacy, risk perception, awareness, and increased bargaining power in reproductive rights negotiations within partnerships (30). Besides, efforts to retain young girls in school have been shown to delay the age of marriage, particularly in rural areas of Pakistan where child marriage is prevalent. By preventing early marriage, education can mitigate the risk of life-threatening pregnancy complications among child brides (31). Despite strides made by the Pakistan government in expanding education access in rural areas, women’s education still lags behind target levels due to social pressures and outdated cultural norms discouraging women’s education (13). Additionally, poverty, pervasive in rural Pakistan, is associated with lower education levels and may limit access to and utilization of maternity care (30,32). Given the limited access to healthcare facilities in rural areas of Pakistan, it is imperative to develop policies and interventions aimed at improving access to quality education for women, particularly young girls, in underprivileged areas such as Baluchistan and the Federally Administered Tribal Areas (FATA). This approach can help increase health literacy, awareness, and delay marriage by keeping girls in school, thereby improving maternal health outcomes.
Findings also indicated a lower rate of adequate ANC, SBA, PNC, and completed CoC among women with higher parity across rural and urban areas. Several studies reported higher parity is associated with improved health literacy and navigation skills and encourages health-seeking behaviors among multipara women that lead to higher access and utilization of maternity care services (20,33,34). However, the results of the present study contradict this notion. This may, in part, be due to difficulties in accessing maternal health services experienced by multipara women, often attributed to childcare duties (35). Additionally, documented suboptimal quality of maternal healthcare in Pakistan could discourage pregnant women from visiting the health facilities, resulting in discontinuity of maternity care (21). In Pakistan, the majority of health interventions mainly focus on the supply-demand chain rather than on the quality of delivered care and are often ignorant of client satisfaction and subsequent service utilization (36) which may disrupt the continuity of maternity care across prenatal, birth and postnatal periods. The dearth of evidence concerning the successful implementation of quality improvement measures in maternity care is worrisome and of great concern in a country with a high MMR (37). In light of the identified challenges, there is an urgent need for further research to identify ways to improve the quality and continuity of maternity care in Pakistan. Future research could focus on exploring potential interventions and policies that could address the barriers to accessing and utilizing maternity care services, particularly in rural areas.
Another important finding of the present study was higher rates of adequate ANC, SBA, PNC, and completed CoC among those who own a mobile phone, use internet, watch TV, and read newspapers‒collectively are considered as having access to mass media (38). Mass media serves as an important source of information and health knowledge for women, with higher health literacy and navigation skills observed among those exposed to it (27,38). Nowadays, massive health-related information is communicated through mass media. Broadcasted information related to family planning through the internet, radio, television, or newspaper is the main source of health knowledge among women living in remote areas in Pakistan and could shape women’s health-seeking behavior during pregnancy (39). Similar to our study, studies from India (40), Cambodia (24), Zambia (41), and Ethiopia (22) have shown higher rates of adequate ANC, SBA, PNC, and completed CoC among women exposed to such mass media, particularly in rural areas. Therefore, health authorities are encouraged to take advantage of this opportunity to disseminate information related to maternity care, which could promote the utilization and continuity of these services, especially in rural areas. By utilizing various channels of communication, such as mass media or community outreach programs, health authorities can improve awareness of the importance of maternal healthcare services and encourage women to seek and continue to receive such care. This, in turn, can lead to better maternal health outcomes and reduce disparities in maternal healthcare access and utilization.
Although each element of CoC‒ANC, SBA, and PNC‒provide essential and potentially life-saving benefits, a successful CoC entails the attendance of all necessary maternity services during the prenatal, birth, and postnatal periods. This study found that those who received adequate ANC are more likely to have SBA and PNC; however, having SBA was not associated with having PNC. Similar findings have been documented in other developing countries (42,43). It has been shown that frequent contact with healthcare providers during the antenatal period could enhance the client’s health literacy and perception of the potential benefits that continuous maternity care could bring about (43). Additionally, clients could discuss the birth plans and options for delivery with their healthcare providers during ANC visits (44). Therefore, given the critical role of adequate ANC in the continuity of maternity care in Pakistan, authorities should promote interventions and policies that facilitate access to such care, particularly among young women with suboptimal access and utilization of ANC, and those living in rural areas with limited access to such care. Expectant mothers should be guided along the continuum of care and encouraged to attend maternity care through appropriate strategies such as cash transfers to reduce costs for underprivileged individuals or sending reminders and educational messages to clients with mobile phones to maintain continuity of care (45).
Limitations
While this study provides valuable insights into the prevalence, determinants, and continuity of three critical maternity care services - ANC, SBA, and PNC - across rural and urban areas in Pakistan, some limitations should be considered in the interpretation of the results. Firstly, the cross-sectional design of the study precludes any causal inferences. However, as there is a logical chronological order to the continuum of maternity care, one could infer causal relationships between adequate ANC and subsequent SBA and PNC, as well as between SBA and PNC. Another potential limitation is the possibility of recall and social desirability biases, which may lead to over- or underestimation of the results. Besides, there are some factors that can influence the access to maternity care that were not collected in DHS such as the distance from the facility, transportation, and cultural and religious norms that might confound the findings and should be considered in future DHS endeavors. Despite these limitations, the findings of this study provide a valuable foundation for further research into maternal healthcare utilization and access in Pakistan, particularly in the context of rural and urban disparities.
Conclusion
It was evident that women with higher education and wealth are more likely to have adequate ANC, SBA, PNC, and completed CoC. Additionally, the likelihood was significantly higher among those who have access to mass media. The results indicated no significant differences in the sociodemographic determinants of utilization and access to maternity care and completed CoC between urban and rural areas in Pakistan. Given the persistent disparities in healthcare access between urban and rural areas, which are challenging to address due to limited resources in countries like Pakistan, it is imperative for the government to prioritize empowering women rather than solely investing in new infrastructure, which is often costly and time-consuming. Moreover, as women’s education can profoundly impact social determinants of health and healthcare access, facilitating Pakistani women’s access to quality education is essential, especially in more traditional societies where cultural norms may discourage women from seeking education. Moreover, policymakers and healthcare providers should recognize the crucial role of mass media in enhancing health literacy, awareness, and continuity of care, and should integrate it into future policies and interventions.
Conflict of Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Availability of data and material
The DHS questionnaire that collected the data in Pakistan’s demographic and health survey in 2017-18 could be downloaded from DHS’s official website (https://dhsprogram.com/data/available-datasets.cfm). The dataset (PDHS 2017-18) that was used in this study could be available upon a reasonable request and with permission from the DHS website.