Document Type : Case report
Abstract
Background: The mouth is the mirror of the body and can manifest signs of underlying health issues. The oral soft and hard tissues are physically linked to the rest of the body. Therefore, the role of dentists is much greater than the dental setup. Many physicians consider dentistry as a purely practical occupation and not scientific. In recent years, the relationship between oral and systemic disease has become a leading research issue. Interventional studies focused on the relationship between dental treatment and its effect on certain systemic condition. In this regard, the aim of this study is to introduce a case of Cowden Syndrome (CS) which was first diagnosed according to their oral manifestations by a dentist.
Case report: A 37-year-old woman was referred to the Department of Oral Medicine, Shahid Beheshti University of Medical Sciences complaining of aesthetic problems. Intra-oral examinations showed grooves and papillomatosis. Examination of the oral cavity showed a high- arched palate, hypoplasia of the maxilla and jaw. According to the patient’s oral presentation, we asked for a consultation with gastroenterologist, gynecologist and endocrinologist. Finally, based on clinical and paraclinical findings, the clinicians put the final diagnosis of CS.
Discussion: According to the review of literature, less than 500 cases have been reported worldwide, many of which have been diagnosed by dental surgeons, or oral pathology and medicine specialists by recognition of mucocutaneous lesions. There is a close association of CS with the development of several malignant neoplasms. This point emphasizes the importance of the early recognition of these lesions, which facilitates an early diagnosis of CS. Oral lesions can be the first sign of the disease, because they develop in 90 to 99% of cases. The diagnosis of CS in this case was made based on criteria proposed by the International Cowden Syndrome Consortium.
Conclusion: Since the patients can have a variety of clinical manifestations, the diagnosis can be mistaken and delayed. Therefore, it seems that there is a need for awareness of this entity in the dental community.
Keywords: Dental care, Dentists, Dentist’s role, Hamartoma Syndrome multiple, Mouth, Occupations, Physicians
Introduction
The mouth is the mirror of the body and can manifest signs of underlying health issues. Therefore, a multidisciplinary approach needs to optimize patient health and safety (1). The oral soft and hard tissues are physically linked to the rest of the body via blood, nerve and lymphatic channels (2). Therefore, the role of dentists is much greater than the dental setup (2). Dental education already includes the ability to recognize more than 100 manifestations of genetic derangement, systemic disease and lifestyle problems (3). Because of their training in oral health and its relation to systemic situations, dentists are in an ideal position in diagnosis of physical and mental disorders (3). However, many physicians consider dentistry as a purely practical occupation and not scientific, which may be due to deficit communication and consultation between doctors and dentists (4). In recent years, the relationship between oral and systemic disease has become a leading research issue. Lots of epidemiological studies investigated the association between oral diseases and systemic conditions, including diabetes, cardiovascular diseases, pneumonia, rheumatoid arthritis and pregnancy outcomes (5). Interventional studies focused on the relationship between dental treatment and its effect on certain systemic condition (5). In this regard, the aim of this study is to introduce a case of Cowden Syndrome (CS) which was first diagnosed according to their oral manifestations by a dentist and confirmed after consultation with some physicians in different specialties.
CS is a rare autosomal dominant disorder characterized by oral and skin lesions, and is associated with an enhanced risk of cancer development (6). The oral findings include: hypoplasia of the mandible and maxilla; a high-arch palate; hypoplasia of the soft palate and uvula; microstomia; papillomatosis of the lips and oral pharynx scrotal tongue (7). The diagnosis of CS is based mainly on clinical findings and oral cavity manifestations (8). Early diagnosis is crucial in patients affected by CS. Because of the oral lesions (papillomatous growths) can be seen in 99% of cases; the dentists may be the first to notice any atypical changes in the oral cavity and refer the patient for further examinations. This emphasizes the responsibility of dentist in the early diagnosis of this progressive pathological entity (6).
Case report
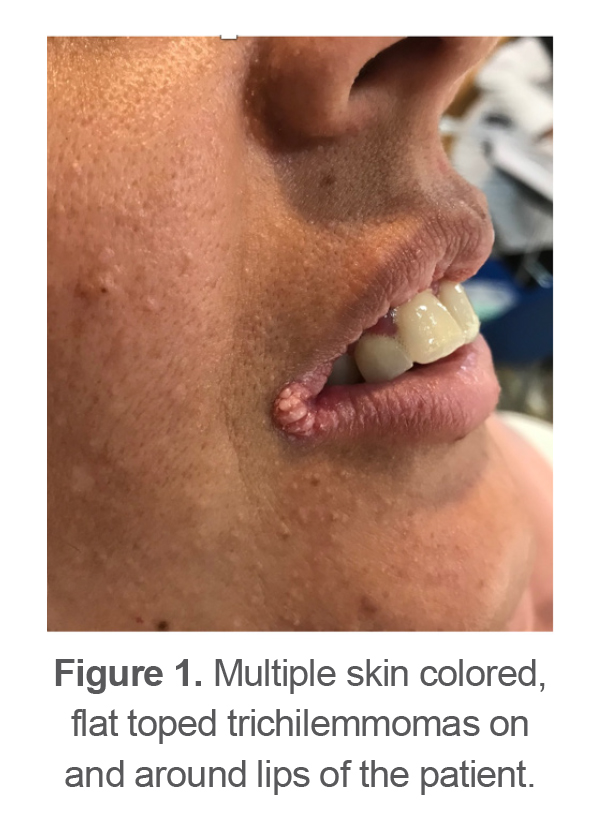
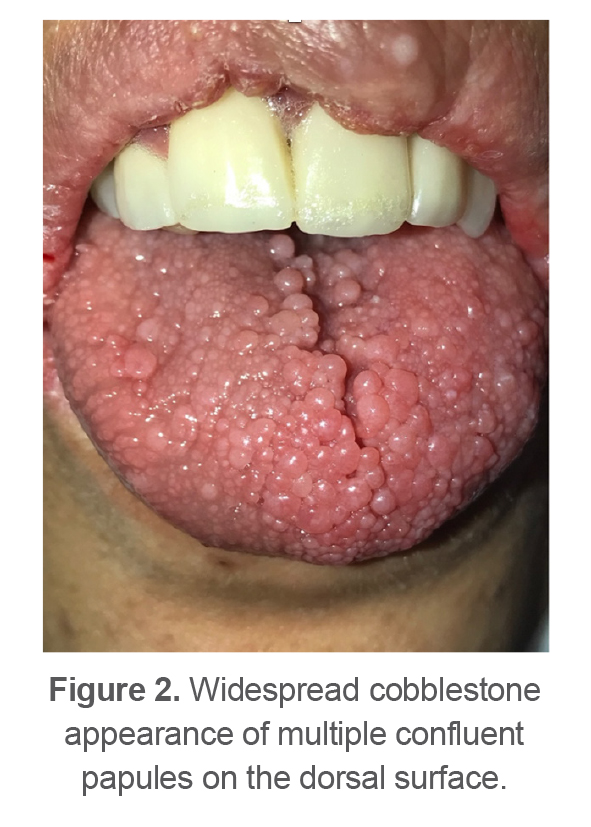
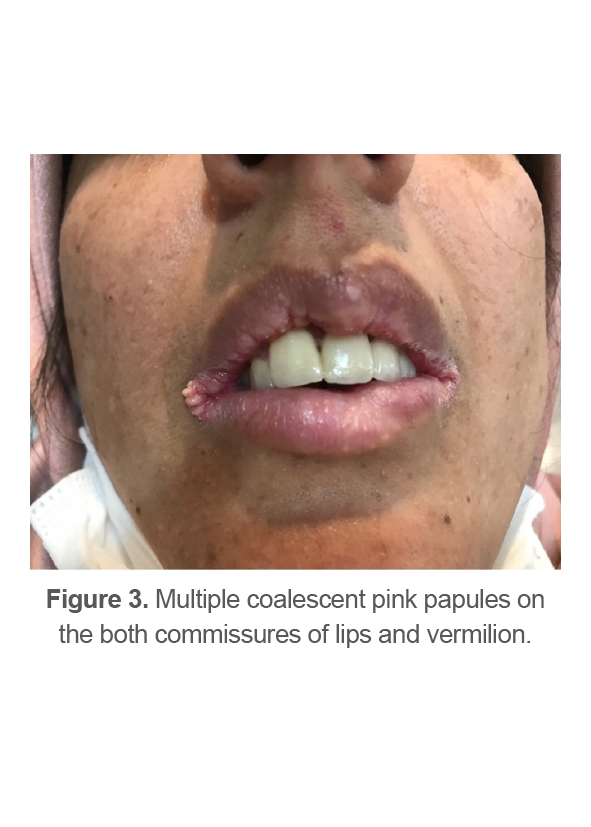
A 37-year-old woman was referred to the Department of Oral Medicine, Shahid Beheshti University of Medical Sciences complaining of aesthetic problems because of sessile lesions on the labial sides (Figure 1). Intra-oral examinations showed grooves and papillomatosis of a normal mucosal color on the tongue surface (Figure 2), oral multiple coalescent papillomatous lesions covering cervical area of teeth, gingiva and labial mucosa (Figures 3-5).
The patient had complained of lesions in the oral cavity for 20 years. Examination of the oral cavity showed a high- arched palate, hypoplasia of the maxilla and jaw. There was no clinical evidence of potentially malignant lesions in the oral district. Macrocephaly, dolichocephaly and adenoid faces were observed. Oral biopsy was performed from the papillomatous lesion of the tongue and the histopathologic examination showed inflammatory fibroepithelial hyperplasia. HPV associated lesions were rolled out with PCR. Several professionals in other areas of the health service including dermatologist, had already investigated these lesions without achieving a conclusive diagnosis.
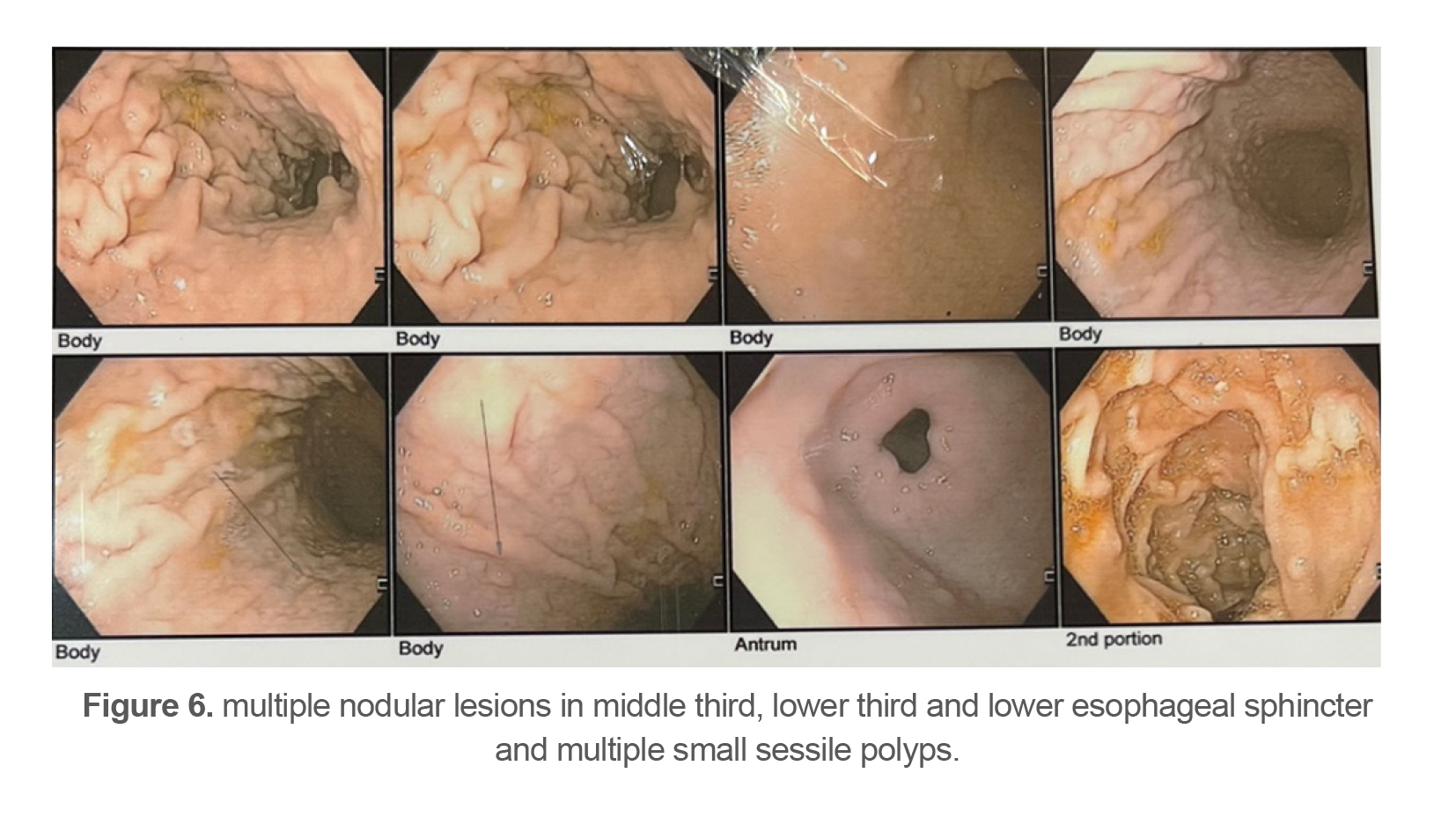
According to the patient’s oral presentation, we asked for a consultation with gastroenterologist, gynecologist and endocrinologist. In the gastrointestinal system assessment, they found multiple nodular lesions in middle third, lower third and lower esophageal sphincter and multiple small sessile polyps without active bleeding were seen in body, fundus and incisura. None of these lesions were malignant (Figure 6).
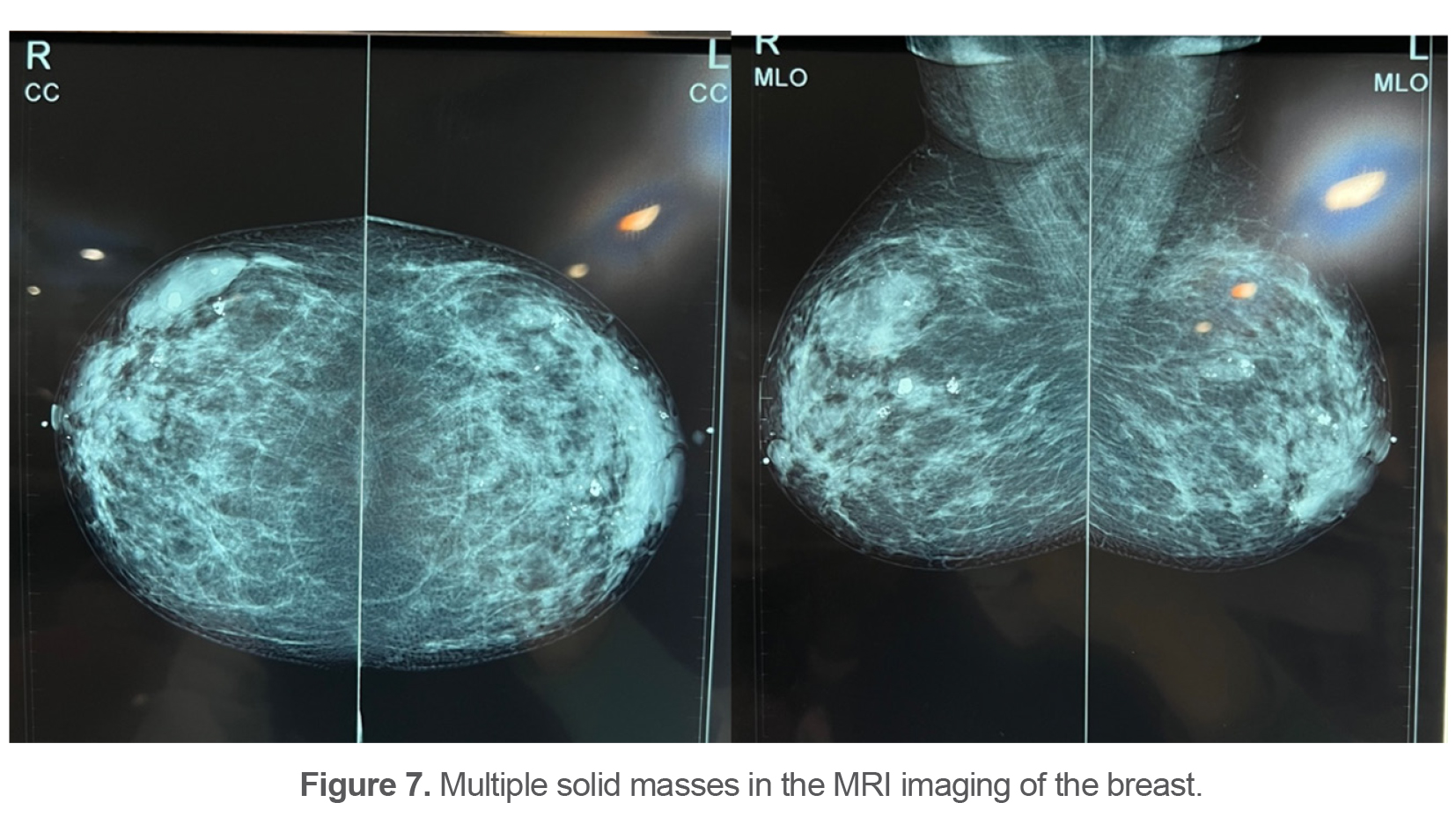
In the examination of breast and auxiliary ultrasound on both sides, the fibrous tissue in the breasts was prominent and thick with hypoechoic areas scattered among them in the context of moderate fibrocystic changes. The image of multiple solid masses was mainly seen with a benign appearance containing calcification and rarely with a suspicious appearance (Figure 7). Biopsy of suspicious breast lesions was performed under ultrasound guidance. There were no invasive cells as confirmed by PanCK immuno-staining seen. In sonography of thyroid, some nodules were found. The histological assessment showed multiple follicular adenomas without malignancy.
Finally, based on clinical and paraclinical findings, the clinicians put the final diagnosis of CS. A Diode laser with a power of 2 W was used to treat lesions on the corners of the patient’s lips. In addition, the patient was examined by an internist to investigate and follow up the problems related to CS and to survey other family members.
Table 1. Pathognomonic lesions and major and minor criteria
|
Pathognomonic lesions |
Major Criteria |
Minor Criteria |
|
Mucocutaneous lesions Facial trichilemmomas Acral keratoses Papillomatous lesions Mucosal lesions |
Breast carcinoma Thyroid carcinoma Macrocephaly (occipital frontal circumference≥97th percentile or ≥60 cm) Lhermitte-Duclos disease (cerebellar dysplastic) Endometrial carcinoma |
Other thyroid lesions Mental retardation (IQ≤75) Gastrointestinal hamartomas Fibrocystic disease of the breast Lipomas and fibromas Genitourinary tumors (uterine fibroids, renal cell carcinoma) or malformations |
Discussion
CS or multiple hamartomas syndrome is a rare autosomal dominant Geno dermatosis with variable expressiveness that was first described by Lloyd and Dennis in 1963 (7). The prevalence of this entity is 1 in 200000 persons, and women are more affected (60%) than men (8). The age of onset usually ranges between 4 and 75 years with a mean age of diagnosis of 39 years (8). Often, the symptoms appear in the third and fourth decade of life (9). It is determined that 10-15% of the cases have a family member also affected by this phenomenon (10). According to the review of literature, less than 500 cases have been reported worldwide, many of which have been diagnosed by dental surgeons, or oral pathology and medicine specialists by recognition of mucocutaneous lesions (8). The diagnosis of CS is mainly based on clinical findings (8). There is a close association of CS with the development of several malignant neoplasms such as thyroid, breast, endometrial, colorectal, and renal carcinomas (6,8,9). This point emphasizes the importance of the early recognition of these lesions, which facilitates an early diagnosis of CS (8). The main differential diagnosis of CS is listed as multiple pointed condyloma acuminatum, multiple irritation fibromas, multiple neuromas, acanthosis nigricans, Darier disease, Heck’s disease, tuberous sclerosis and lymphangioma (9). According to the International Cowden Syndrome Consortium, clinical presentations can be divided into three subgroups as pathognomonic lesions, major and minor clinical criteria (Table 1) (10). CS is diagnosed when the patient shows one of the following criteria (9):
Presence of pathognomonic lesions such as
- Six or more facial papules, of which three or more are trichilemmomas.
- Facial papules and papillomatosis in oral mucosa.
- Papillomatosis in oral mucous and acral keratosis.
- Six or more palmoplantar keratosis lesions
Presence of two major criteria, one of which must be macrocephaly or Lhermitte-Duclos disease
Presence of one major criterion and three minor criteria
Presence of four minor criteria
Oral lesions (fibrotic lesions with cobblestone or pebbly pattern) can be the first sign of the disease as they develop in 90-99% of cases and are as a part of pathognomonic criteria for the diagnosis and the age of onset of these lesions ranges from birth to 46 years, with an average 22 years (8,9). In addition to fibro papillomatosis lesions, scrotal tongue, high-arched palate and a tendency to contract periodontal disease may be seen in these patients (6,9).
Liked other previous reports, the diagnosis of CS in this case was made based on criteria proposed by the International Cowden Syndrome Consortium. She fulfilled adequate items in almost all diagnostic subgroups which have been classified as pathognomonic lesions, major and minor clinical criteria (9). However, there was no evidence of malignant changes after evaluation of high-risk organs. In addition, the other characteristics of this case were in accordance to the previous reports in terms of the age of onset of the disease, sex, the age of onset of the oral lesions, patterns of oral lesions, shape of palatal arch and clinical presentation of tongue surface (6,8,9). In this case, the dentist had the key role in tentative diagnosis and further evaluations.
Conclusion
In conclusion, as patients can have a variety of clinical manifestations, its diagnosis is commonly mistaken and delayed. Therefore, it seems that there is a need for awareness of this entity in the dental community. This would improve early diagnosis of CS and timely treatment of related malignancies.
Conflict of Interest
Informed consent was obtained from the patient.