Document Type : Original article
Abstract
Background: A significant gap exists between patient-centered health policies and medical graduates’ practice. Medical education is not restricted to the formal curriculum. The hidden curriculum has a powerful effect on students’ learning and behavior. This study measured the patient-centeredness of the hidden curriculum in Mashhad Medical School.
Methods: The participants were medical students at Mashhad Medical School who were about to graduate. The sample size was determined 100 students based on the Morgan table and selected in a convenient method. The validated Persian version of the Haidet instrument with three content areas of “role modeling, student’s experiences and support for students’ patient-centered actions” was used to evaluate the patient-centeredness of the hidden curriculum. Descriptive indexes and Independent samples T-Test were used for analysis.
Results: The mean±SD score of patient-centeredness of the hidden curriculum was 54.9±9.4, slightly more than half of the total questionnaire score. The area of "support for students' patient-centered actions" received a higher mean±SD score (62.1±16.5) compared to role modeling (53.9±12.3) and student experiences (53.6±9.4). Additionally, medical students emphasized the professor's role in acquiring patient-centered care.
Conclusion: Despite the formal education for patient-centeredness, students learn mainly from the practical environment and their educators’ behaviors. There was a relative dissonance between the formal and implicit curriculum regarding patient-centeredness associated with the medical student. The medical students’ experiences regarding patient-centered manners and giving encouraging feedback are two chief points for improving patient-centeredness.
Keywords: Curriculum, Education, Medical, Patient-centered care, Physicians, Schools, Medical, Universities
Introduction
Patient-centered care is crucial in providing healthcare, since it emphasizes treating individuals with dignity and involving them in decision-making regarding their health. It is considered a fundamental aspect of a quality healthcare system and plays a vital role in fostering a strong doctor-patient relationship (1). The concept of “hidden curricula” pertains to the implicit, subtle, and sometimes unintentional teachings regarding the true expectations of students, which may deviate from the official school guidelines (2). These teachings can be communicated through informal discussions among faculty members or through observed dynamics in student-faculty relationships. In experiential learning settings or internships, students might come across hidden curricula that prioritize goals other than holistic, biopsychosocial care or the monetary value of healthcare services (3-5).
In contrast to traditional apprenticeship which involves learners training and gaining proficiency through observation and assistance, cognitive apprenticeships focus on developing skills that require internal thought processes. This approach emphasizes learning through cues from role models, coaching, and scaffolding that builds on prior knowledge, often utilizing metacognitive tools for articulating thought processes and reflecting on problem-solving strategies. Apprenticeship in clinical settings encompasses a more unpredictable environment, where learners encounter interpersonal interactions, ambiguity, and risks, ultimately shaping a professional identity influenced by both the explicit teachings and the hidden curriculum (5).
The hidden curriculum, which has garnered increased attention in recent years, plays a significant role in bridging the gap between formal education and students’ behaviors, beliefs, and attitudes (4,5).
The hidden curriculum comprises implicit and unspoken standards, habits, and values (3). The hidden curricula can have varying effects, either positive, negative, or neutral. However, it is believed to have a negative impact on student learning and their acceptance of patient-centeredness in health professional education (4). Some surveys have indicated that medical students’ patient-centered attitudes tend to decline with each passing year of their training, despite the formal curricula’s focus on patient-centered communication, values, and behaviors (4,6).
It is imperative to identify and manage the key factors contributing to the development of the hidden curriculum. Educational planners at universities must acknowledge both the positive and negative aspects of their hidden curriculum and pinpoint areas that require intervention (6,7). Numerous studies have demonstrated that a substantial portion of a medical student’s learning occurs through the school’s hidden curricula (8,9).
A physician’s clinical competence relies on four primary skills: Medical Knowledge, Communication Skills, Problem-Solving Skills, and Physical Examination (6,10). Current directives in medical universities underscore the significance of fostering patient-centered care in both practice and medical education, as patient-centeredness stands as a crucial component of medical professionalism (11,12). Assessments of patient satisfaction and medical errors underscore the need for physicians to enhance their patient-centered care approach (4,5).
Despite the recognition of the importance of patient-centeredness, there is limited understanding regarding how the hidden curriculum influences medical students’ perspectives on patient care. Prior research has primarily focused on explicit educational strategies, neglecting the implicit lessons derived from role models, institutional culture, and peer interactions during clinical rotations. The need for research in this domain is underscored by the potential ramifications of inadequate patient-centered training. Graduates who are not fully attuned to the principles of patient-centeredness may inadvertently contribute to poorer patient experiences and increased medical errors. Mashhad University of Medical Sciences (MUMS) is recognized as one of the top medical sciences universities and a leading educational institution in Iran, boasting 51 research centers, and 30 educational hospitals in the region. By focusing on the perspectives of graduated students from MUMS, this study aims to illuminate the factors influencing the hidden curriculum and its implications for practice. Elucidating the dynamics of patient-centeredness within the hidden curriculum of medical education is pivotal. Addressing this gap not only enhances educational strategies at institutions like MUMS, but also ultimately contributes to the overarching goal of improving patient care and safety in the healthcare system. The purpose of this study was to evaluate the patient-centeredness of the hidden curriculum in medical education based on the perspectives of graduated students from Mashhad University of Medical Sciences and its related factors.
Materials and Methods
Participants
The participants in this study were medical students at Mashhad University’s medical school who were graduating in 2020. The sample size comprised 100 students based on the Morgan Table with regard to the total number of Medical students. The inclusion criteria were the medical students of Mashhad Faculty of Medicine at the end of their internship (in the last semester of schooling), and agreeing to participate in the study. Foreign students and guest students from other medical schools were excluded. After extracting the names of the eligible students, the researcher referred to educational hospital wards for inviting the students and completing the questionnaires.
Type of investigation
This research was a descriptive-analytical cross-sectional study conducted regarding the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline.
Data collection
The data collection tool used in this study was the Haidet instrument, which consists of 29 items and assesses the patient-centeredness of hidden curricula in medical schools (7). This instrument can be used by students with minimal clinical experience. It evaluates three areas: role modeling, student’s experiences, and support for students’ patient-centered actions. The first area measures the frequency of patient-centered behaviors students observe during their clinical education. The second area assesses activities with varying levels of patient-centeredness and instances of non-patient-centered behaviors. The third area measures the amount of encouragement students receive for their patient-centered actions. As the patient-centeredness increases in each area, the overall patient-centeredness also increases (7).
The Haidet questionnaire includes 1 to 7 items for role modeling, 8 to 18 items for student’s experiences, and 19 to 21 items for support for students’ patient-centered actions. The responses are rated on a scale ranging from never to always for the first area, from never to very high for the second area, and from 1 for disagreement to 5 for agreement for the third area.
The questionnaire scores for the first area ranged from 5 to 35, for the second area ranged from 11 to 55, and for the third area ranged from 3 to 15. To compare the different areas, the scores from each area were converted to a scale of 0-100. The mean score, standard deviation, and relative score (obtained by dividing the mean score by the lowest score in the same section) were then reported. A higher score indicates a higher level of patient-centeredness. In addition to assessing patient-centered care and communication skills in the clinical course, demographic characteristics of the students and other factors that may affect learning were also examined.
There were some questions in the final section of the questionnaire regarding the most effective learning source of patient-centered care and communication for medical students. It was categorized in five learning sources as “Observation of the professor’s behaviors, Observation of the resident physicians’ behaviors, Observation of the senior interns’ behaviors, Formal practical education, and Self-learning”.
Reliability and validity of the questionnaire
The validity and reliability of the Persian version of the patient-centeredness of the hidden curricula questionnaire were evaluated by Jalalvandi et al (6). The reliability of the questionnaire was assessed in this study, with a total Cronbach’s alpha of 0.85. The Cronbach’s alpha values for the three areas were 0.68, 0.82, and 0.85, respectively.
Statistical analysis
Statistical analysis was performed using IBM SPSS27 (IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp.). In addition to the descriptive analysis, the data were analyzed using the independent samples T-test to compare the scores according to the participants’ characteristics. A p-value lower than 0.05 was considered a significant level.
Table 1. Scores of three content areas of patient-centeredness of medical school’s hidden curricula questionnaire from the student’s point of view in Mashhad University of Medical Sciences
|
Areas of the questionnaire |
Score [out of 100] Mean±SD** |
Relative Score* |
|
Total patient-centeredness |
54.9±9.4 |
1.92 |
|
Role modeling |
53.9±12.3 |
2.69 |
|
Student’s experiences |
53.6±9.4 |
2.11 |
|
Support for students’ own patient-centered actions |
62.1±16.5 |
3.11 |
*Relative Score = mean score/minimum score in each area
**SD:Standard Deviation
Table 2. Scores of patient-centeredness of schools’ hidden curricula questionnaire from the students’ point of view in Mashhad University of Medical Sciences based on student characteristics
|
Areas of the questionnaire |
Score [out of 100] Mean±SD** |
p-value* |
|
Total Patient-centeredness |
|
|
|
gender |
|
|
|
Male |
56.8±8.8 |
0.445 |
|
Female |
52.3±9.9 |
|
|
Residence |
|
|
|
Native |
56.1±8.7 |
0.273 |
|
Non-native |
53.4±10.7 |
|
|
Role modeling |
|
|
|
gender |
|
|
|
Male |
56.5±11.5 |
0.271 |
|
Female |
50.2±12.3 |
|
|
Residence |
|
|
|
Native |
53.3±10.8 |
0.913 |
|
Non-native |
53.6±14.6 |
|
|
Student’s experiences |
|
|
|
gender |
|
|
|
Male |
55.4±9.4 |
0.451 |
|
Female |
51.1±9.1 |
|
|
Residence |
|
|
|
Native |
55.9±8.6 |
0.015* |
|
Non-native |
50.3±10.1 |
|
|
Support for students’ own patient-centered actions |
|
|
|
gender |
|
|
|
Male |
62.5±16.3 |
0.893 |
|
Female |
62.1±17.1 |
|
|
Residence |
|
|
|
Native |
61.8±169 |
0.531 |
|
Non-native |
64.3±15.9 |
*Independent sample T-Test
** SD: Standard Deviation
Table 3. The most effective learning source of patient-centered care and communication in medical students’ view
|
Learning source |
Frequency(%) |
|
Observation of the professor’s behaviors |
46(57.5) |
|
Observation of the resident physicians’ behaviors |
5(6.3) |
|
Observation of the senior interns’ behaviors |
10(12.5) |
|
Formal practical education |
13(16.2) |
|
Self-learning |
6(7.5) |
Results
In this study, after data collection, 82 students agreed to participate in the study and totally completed the questionnaire for evaluating the patient-centeredness of the hidden curriculum. The mean age of the participants was 25.2±1.8 years old, 53.7% were male and 53.4% were native students. The scores for assessing the patient-centeredness of the hidden curriculum at Mashhad Medical School are presented in table 1. This includes the total patient-centeredness score and its components such as role modeling, student experiences, and support for students’ patient-centered actions. The patient-centeredness score of the hidden curriculum was found to be approximately half of the total questionnaire score. Interestingly, the results indicated that the area of “support for students’ patient-centered actions” received a higher score compared to role modeling and student experiences.
Table 2 displays the scores of patient-centeredness from the hidden curriculum questionnaire based on the student characteristics. While male students scored slightly higher than female students across all areas of the questionnaire, there were no significant differences between the two genders in various aspects. Moreover, the scores based on students’ residency were mostly similar, except for the student experiences area where non-native students scored lower than native students (p-value=0.015).
Table 3 illustrates the most effective learning source of patient-centered care and communication according to medical students expressions. Over half of the medical students emphasized the significance of the professor’s role in acquiring patient-centered care. The roles of resident physicians and senior interns were also deemed important. Observing the professors’ behaviors was identified as the most effective factor in learning patient-centered care and communication by majority of the medical students. Formal practical education by the professor and observing the behaviors of senior interns were identified as the next most effective sources.
Discussion
The patient-centeredness score of the hidden curriculum in the medical school of Mashhad University, as evaluated by medical students, was approximately half of the total questionnaire score. The results demonstrated that the area of “support for students’ patient-centered actions” received a higher score compared to the other two areas of role modeling and student experiences. One possible reason for this difference could be that providing positive feedback on students’ communication skills in unpredictable medical center situations is more feasible than monitoring and influencing students’ experiences and role modeling.
The findings of research conducted by Jalalvandi et al regarding the correlation between the utilization of communication skills by medical interns and the patient-centeredness of the hidden curriculum in the three medical universities in Iran (Tehran, Yazd, and Mashhad University in 2014) revealed that, among various aspects, “support for students’ patient-centered actions” received the highest score, while “student’s experiences” received the lowest score. In contrast, the patient-centeredness score of the hidden curriculum at Mashhad Medical School was similar to that of the previous study in 2014 (6).
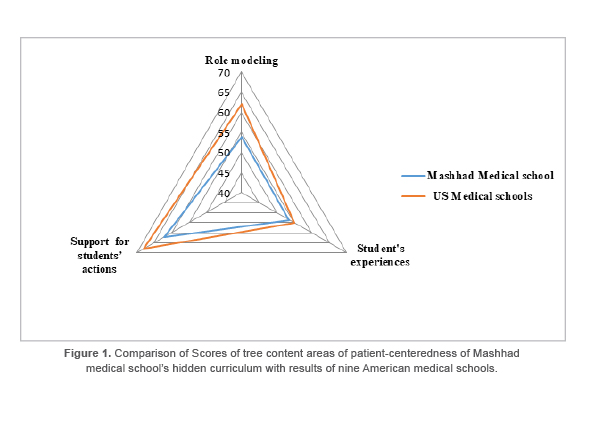
A study by Haidet et al focusing on the assessment of patient-centeredness in hidden curricula across nine medical schools in the United States of America underscored that acquiring patient-centered practice skills heavily relied on hidden curricula and the role modeling of educators (7). The results of two additional studies that evaluated the patient-centeredness of hidden curricula using a similar instrument in American and Saudi Arabian medical schools across three questionnaire areas (role modeling, student’s experiences, and support for students’ actions) were 62, 55, and 68 in the nine American medical schools, and 60, 47, and 54 in Saudi Arabian medical schools, respectively (13,14). In the current study at Mashhad Medical School, the mean scores for the three areas were 54, 53, and 62, respectively, all of which were lower than those of the American schools. However, the scores were higher in the areas of student’s experiences and support for students’ actions compared to the Saudi Arabian medical school.
The resulted scores of tree content areas of patient-centeredness in the present study was compared with those reported in a reference study that introduced an evaluation instrument for patient-centeredness in schools’ hidden curricula. The results of applying this questionnaire in nine American medical schools are also discussed (4,7). Figure 1 presents a comparison of the scores in three content areas of patient-centeredness in the hidden curriculum of Mashhad Medical School with the results from nine American medical schools. The radar chart indicates that scores in the area of student experiences were similar, but differences were observed in the other two areas, particularly in role modeling.
The impact of the hidden curriculum on the patient-centered perceptions of medical students in Saudi Arabia was examined in a recent study, revealing a notable decrease in various questionnaire areas for clinical training. Instances of non-patient-centered behaviors also increased among the students (14). This trend sheds light on the origins of certain non-patient-centered practices in postgraduate medical education. Egnew et al’s research highlighted the crucial role of role modeling in teaching patient-centered care, specefically by medical educators who openly share their personal experiences (15).
Similarly, Mokhtari et al and Karimi et al emphasized the significant influence of professors as behavioral models in shaping students’ practices (16,17). Teachers play a vital role as role models, with learning taking place as students observe and compare their behavior to that of their instructors (16-19). Additionally, implementing innovative educational approaches is essential to instill patient-centered attitudes in medical students as they transition into hospital-based clinical practice (1).
A systematic review revealed that factors such as increasing patient complexity, the effects of a demanding “hidden curriculum,” and the presence of inadequate role models negatively influence medical students’ empathy levels, leading to pessimism and desensitization (18). Unprofessional behaviors from educators can create an environment of humiliation and shame, undermining students’ psychological safety and stifling productive discourse (5). To address these challenges, educators can enhance engagement by inviting participation, which fosters a shared vision and aligns team thinking. By employing active inquiring or open-ended questions and showing respect for learners’ contributions, educators can empower students and promote a more positive educational experience (5).
The incorporation of an empathic hidden curriculum in medical education involves early exposure to real patients, real-life scenarios, empathy assessments, attention to social determinants of health, and improved community health education (19). Moreover, experienced peers can assist students in transitioning to clinical education, as the result of systematic reviews highlighting the benefits of peer mentors in providing both academic and social support (19).
Although the role models of teachers play a crucial role in shaping professional development, particularly in the medical field, where students assess numerous doctor-patient interactions during their training. These evaluations are influenced by the behaviors they observe in senior clinicians and their earlier education, ultimately teaching them the importance of empathy through these examples (16,17,19).
The benefits of providing empathetic care to patients and healthcare providers highlight the importance of implementing interventions in medical education that focus on creating a “hidden empathetic curriculum.” This curriculum should aim to tackle the decline in empathy among medical students, with the goal of halting or even reversing this trend (18,20).
Conclusion
The findings of this study underscore the current inadequacy of patient-centeredness within the hidden curriculum of the medical school at Mashhad Medical School, particularly in terms of role modeling and student experiences. Encouraging feedback and engaging in patient-centered activities are crucial for enhancing the attitudes and behaviors of medical graduates toward patient-centered care. It is imperative to emphasize the professor’s role and shift from a physician-centered to a patient-centered approach in medical education.
Study Strengths and Limitations
Evaluating the perspective of medical students upon completion of their internship, after acquiring hands-on experience throughout the 3.5-year clinical program, and utilizing reliable questionnaires are the key strengths of this research. However, the student self-reporting and the inability to observe student behavior in the real fields were significant limitations of this study. The observational data in the field could provide richer context and a more nuanced understanding of how practical experiences shape students’ professional identities and competencies. Future surveys should strive to incorporate these elements to foster a more holistic view of medical students’ experiences and perspectives. In addition, assessment of HC from the multiple sources such as educators, patients, peer educators, and other health care team members can give the researchers comprehensive views.
Acknowledgement
We would like to express our gratitude to the personnel at the medical school of Mashhad University for their support. This study protocol was approved by the Research Ethics Committee of the Mashhad University of Medical Sciences: (Ref: IR.MUMS.fm.REC.97.0072).
Conflict of Interest
There was no conflict of interest in this manuscript.
16 Karimi Moonaghi H, Yazdi Moghaddam H. [Role modeling and mentor in nursing education.] Res Med Educ 2014 Mar 10;6(1):59-71. Persian. URL: http://rme.gums.ac.ir/article-1-201-en.html