Document Type : Original article
Abstract
Background: The literature on the potential protective role of serum bilirubin levels in the development of Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD) has produced conflicting findings. This study aimed to investigate the potential relationship between serum total and direct bilirubin levels and the risk of acute exacerbation in COPD.
Methods: Over a period of 18 months, a total of 99 patients were recruited from two major hospitals in Mashhad, Iran, comprising 49 individuals with stable COPD and 50 with AECOPD. After obtaining informed consent and conducting a comprehensive medical history and physical examination, both groups underwent an assessment of various laboratory indices, such as total and direct bilirubin levels. Appropriate statistical analysis was applied to assess the potential associations between bilirubin concentrations and the risk of AECOPD.
Results: The study population had a mean age of 64.97±10.12 years, and there was no significant difference in gender distribution (p=0.546). The majority of subjects (55.6%) were male. The serum levels of AST and ALT were significantly higher in the AECOPD group (p<0.001). Additionally, although there were no significant differences in total bilirubin levels between the two groups (p=0.323), there was a significantly higher level of direct bilirubin in the AECOP group (p<0.001).
Conclusion: Serum direct bilirubin levels were higher in COPD patients with acute exacerbation. It may be an independent biomarker for screening the COPD patients with and without acute exacerbation. Further studies are required to validate the findings.
Keywords: Bilirubin, Biomarkers, Chronic obstructive pulmonary disease, Iran, Physical examination
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is a preventable lung disease characterized by consistent airflow obstruction. Currently, COPD poses a vast burden on health-related resources (1). In fact, it has been reported that 384 million individuals are affected by the disease worldwide, with at least 50% being underdiagnosed (2,3). COPD has been the third-leading cause of death over the past decade (4); in addition, the disease impacts patients’ psychological states, causing anxiety and depression (5). The main symptoms of the disease include progressive dyspnea, cough, and fatigue (6). COPD patients could often experience events of symptom worsening, referred to as Acute Exacerbation of COPD (AECOPD); the process could be so overwhelming that the term “stroke of lungs” has been occasionally used to describe it (7).
Systemic inflammation has been introduced as an underlying pathophysiology for developing COPD and AECOPD (8). Previous studies have assessed the hypothesis and reported elevated levels of C-reactive protein (CRP), fibrinogen, and white blood cell (WBC), which are inflammatory mediators (9,10). On the other hand, bilirubin is considered an antioxidant agent, one function of which is inhibiting membrane-bound Nicotinamide Adenine Dinucleotide Phosphate Oxidase (NADPH) (11). Therefore, a possible association between the serum level of bilirubin and the severity of symptoms in COPD has been hypothesized; however, the findings of previous studies have been controversial, some in favor of it (12,13) and some opposed to it (14,15).
At present, there exists no known definitive cure for the disease, and the available treatment options primarily target the relief of symptoms. Moreover, the lack of a readily available and economical means of monitoring pulmonary functionality in afflicted individuals renders the evaluation of outcomes challenging (13). Therefore, considering the recognized function of bilirubin in redox homeostasis, the present study aimed to investigate the potential relationship between serum levels of total and direct bilirubin and the risk of acute exacerbation in patients with COPD.
Materials and Methods
Study design
The present case-control study was conducted in 2022 in Imam Reza and Ghaem Hospitals of Mashhad, Iran. This study used a convenience sampling method of all patients affected with AECOPD, referred to these hospitals over eighteen months. The exclusion criteria of the present study were (i) a history of known liver disease; (ii) a history of the pancreas and gall bladder diseases; (iii) alcohol consumption; (iv) a drug history of phenobarbital and phenytoin drugs; (v) confirmed heart failure; and (vi) active malignancy. After obtaining informed written consent, the patients were subjected to a complete examination in terms of past medical history, the extent and duration of smoking, and a thorough physical examination. At the same time, the same number of COPD patients who had outpatient visits to Imam Reza and Ghaem Hospitals clinics without evidence of an AECOPD (increased cough, sputum, and shortness of breath) were studied as the control group, and the results were compared.
Laboratory measurements
After the hospitalization of patients diagnosed with an AECOPD, 5cc of blood samples were sent to the laboratory for routine tests, including complete blood cell count, quantitative C-reactive protein (CRP), Creatinine (Cr), Blood Urea Nitrogen (BUN), blood electrolytes (Na,K), Aspartate aminotransferase (AST), Alanine aminotransferase (ALT), alkaline phosphatase (ALP), and Erythrocyte Sedimentation Rate (ESR). In patients diagnosed with COPD, Arterial Blood Gases (ABG) and pulse oximetry were performed to measure oxygen saturation. Also, to measure total and direct bilirubin, 2 ml of blood was taken from the patient and sent to the hospital laboratory. To avoid the laboratory errors, all the samples were sent to the laboratory of Imam Reza and Ghaem Hospital.
Statistical Analysis
Statistical analysis was conducted using SPSS 22 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean±standard deviation (SD). Categorical variables presented as n (%). Independent sample t-test, Chi-square, and/or Fisher’s exact test were used to assess the possible correlation between serum total/direct/indirect bilirubin levels and clinical parameters in COPD patients. A Receiver Operating Characteristics (ROC) analysis was also applied to identify the cutoff point of serum total and direct bilirubin levels as well as the related sensitivity, specificity, and area under the ROC curve (AUC) with 95%CI to evaluate their screening value. p<0.05 (two-sided) was considered to indicate the statistical significance.
Table 1. Baseline characteristics of the patients categorized based on the acute exacerbation
|
|
COPD N=49 |
AECOPD N=50 |
p-value |
|
|
Demographic |
||||
|
Gender (%) |
Male |
29(59.2) |
26(52) |
0.546 |
|
Female |
20(40.8) |
24(48) |
||
|
Age (years; mean±SD) |
62.27±8.70 |
67.62±10.79 |
0.008 |
|
|
Hematological |
||||
|
Hb (g/dL) |
14.06±1.79 |
13.57±1.62 |
0.161 |
|
|
PLT (109/L) |
257±113 |
253±75 |
0.827 |
|
|
WBC (109/L) |
7.47±2.01 |
7.33±2.03 |
0.721 |
|
|
VBG |
||||
|
pH |
7.38±0.03 |
7.34±0.07 |
0.002 |
|
|
HCO3 |
27.33±3.61 |
29.24±4.42 |
0.021 |
|
|
PCO2 |
45.77±5.51 |
57.96±12.03 |
<0.001 |
|
COPD: chronic obstructive pulmonary disease; AECOPD: acute exacerbation of chronic obstructive pulmonary disease; Hb: hemoglobin; PLT: platelet; WBC: white blood cell; VBG: venous blood gas
Table 2. The association between liver enzyme and bilirubin with COPD and COPD exacerbation
|
|
COPD |
AECOPD |
p-value |
|
AST (u/L) |
19.04±6.04 |
30.70±9.97 |
<0.001 |
|
ALT (u/L) |
16.89±7.18 |
29.74±14.10 |
<0.001 |
|
ALP (u/L) |
223.14±77.17 |
217.12±46.68 |
0.643 |
|
Alb (g/dL) |
3.86±0.42 |
3.75±0.18 |
0.087 |
|
Bilirubin T (mg/dL) |
0.88 |
0.8 |
0.323 |
|
Bilirubin D (mg/dL) |
0.21 |
0.39 |
<0.001 |
COPD: chronic obstructive pulmonary disease; AECOPD: acute exacerbation of chronic obstructive pulmonary disease; AST: aspartate aminotransferase; ALT: alanine aminotransferase; Alb: Albumin
Results
Ninety-nine patients with an average age of 64.97 ± 10.12 years were included in the study, of which 49 were in the stable COPD group, and 50 were in the AECOPD group. Of the patients included in the study, 55 (55.6%) were male, and the rest were female. Table 1 compares the demographic characteristics of the two groups. The gender of the patients in the two groups was not significantly different (p=0.546), but the age of the patients in the AECOPD group was significantly higher than the patients in the COPD group (p=0.008). Furthermore, the pH of AECOPD patients was significantly lower than COPD patients (p=0.002), but their PCO2 (p<0.001) and HCO3 (p=0.021) were significantly higher than the stable patients. Regarding the CBC findings of the two groups, there was no difference between the two groups (p>0.05).
Table 2 shows the level of liver enzymes and albumin in two groups of the patients. The level of AST (p<0.001) and ALT (p<0.001) in the AECOPD group was significantly higher than those in the COPD group. Furthermore, no significant difference was found for the total bilirubin (p=0.323) between the two groups. However, the direct bilirubin levels were significantly higher in the AECOPD group compared to the COPD group (p<0.001).
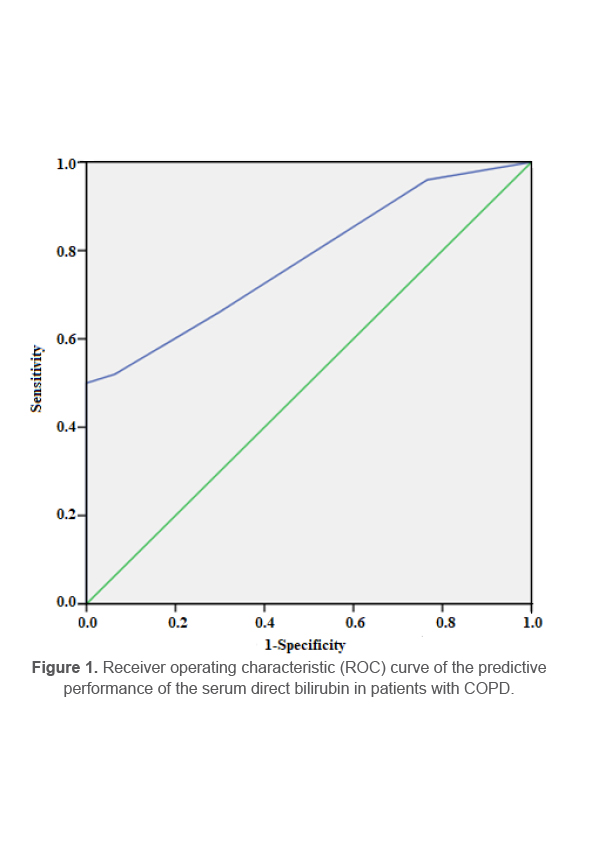
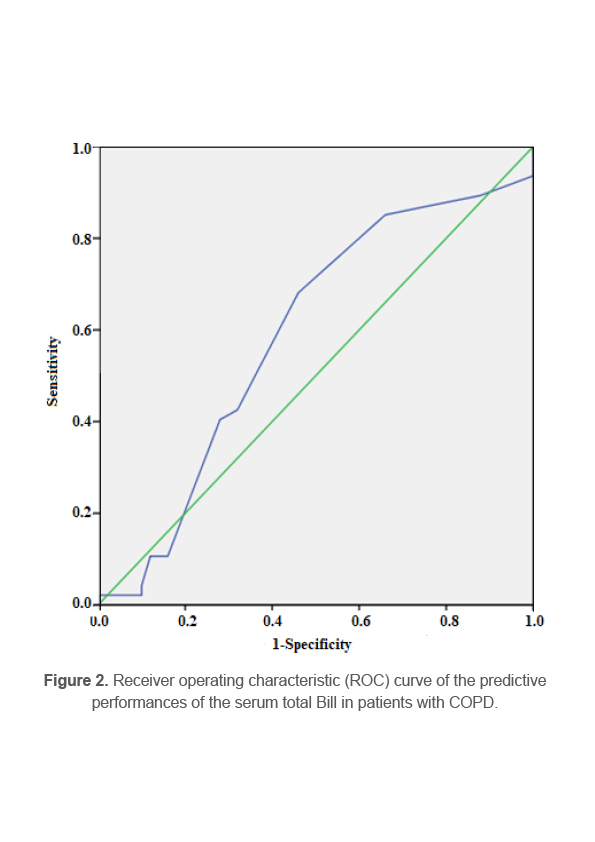
In order to assess the screening utility of level, the ROC curve was plotted and an optimal cut-off point of 0.25 mg/dL, with a corresponding sensitivity of 70% and specificity of 70% was calculated (95%CI, 0.69-0.87) (Figure 1). The AUC for serum direct bilirubin was 0.78 (95%CI, 0.69–0.87) which can be considered as an independent predictor of AECOPD. Furthermore, the ROC plot for total bilirubin showed a cut-off of 0.75 mg/dl with a sensitivity of 70% and a specificity of 55% and the AUC of 0.59 (95%CI, 0.47-0.70) (Figure 2).
Discussion
In the present study, the association between the liver function enzymes, total bilirubin, and direct bilirubin with COPD and AECOPD was assessed. The study results demonstrated that AST and ALT serum levels were significantly different between the two groups. Moreover, while total bilirubin levels showed no significant difference, serum direct bilirubin level was significantly higher in AECOPD patients and represented greater potential in screening utility for differentiating the COPD patients with and without acute exacerbation.
COPD is a chronic lung disease associated with endogenous and exogenous oxidative stress (16). Heme oxygenase-1 (HO-1) is an enzyme that contributes to the inflammation process in multiple disorders, including COPD (17). The enzyme is produced within the pulmonary cells and the resident alveolar macrophages (18). The resulting oxidative stress lays certain damage on lipids in the lungs, further deteriorating the process leading to damaged cell structure and permeability (19). It has been shown that more severe airflow obstruction in COPD is associated with higher lipid peroxidation in the lungs (20,21).
On the other hand, studies have demonstrated antioxidant and anti-inflammatory properties for bilirubin in animal models (22,23). Furthermore, it has been shown that smoking, as an exogenous oxidant, leads to decreased bilirubin levels, which reverts to the baseline shortly after smoking terminates (24). Also, polymorphisms in UDP-glucuronosyl transferase-1A1 (UGT1A1), an enzyme responsible for the excretion of bilirubin into the bile, have been shown to be associated with possible improved respiratory outcomes (25). Bilirubin has also shown antioxidant effects in organs other than lungs as studies have reported bilirubin improved vascular endothelial activation (26).
Several studies have assessed the association between serum bilirubin levels and disease outcomes in COPD. In a large study in the UK, 504,206 individuals were followed up for eight years, and the results revealed that higher serum levels of bilirubin had a significant association with developing COPD. Furthermore, they indicated that lower bilirubin levels were associated with a lower risk of lung cancer and all-cause mortality (27). Dai et al claimed a 6% decrease risk of COPD for each 0.1 mg/dL increase in bilirubin level (28). Also, some studies showed that higher bilirubin levels were associated with fewer COPD exacerbations (29), which is in line with our findings.
Nevertheless, higher than normal bilirubin levels have also been associated with adverse outcomes in COPD patients; in fact, a study reported a cut-off of 1 mg/dl for bilirubin above, which was associated with a slight increase in mortality (27). However, there were contradicting results in the literature as well. Leem et al reported that higher serum levels of bilirubin were associated with a higher risk of COPD exacerbation, particularly among GOLD III-IV patients (30). Nevertheless, they explained their contradicting results by pointing out the relationship between right-sided heart failure and higher bilirubin levels and that COPD patients with cor pulmonale are at higher risk for COPD exacerbations (30,31). A more recent systematic review also demonstrated an association between higher bilirubin levels and COPD exacerbations; however, the authors reported this finding as having low strength of evidence (25). All these studies have been observational studies, and no clinical trial has been conducted so far, leaving no room for judgment on the causality relationship between the two factors. As a minor finding in this study, significantly different AST and ALT between the two groups were represented, while previous studies have shown otherwise (32,33).
The current study had some limitations. First, the study was observational, which is naturally associated with some biases. Second, relying solely on self-reported medical history may lead to inaccurate inclusion of individuals with undiagnosed liver disease. Finally, due to the small sample size, the results should be interpreted with regard to the study content.
Conclusion
In conclusion, serum direct bilirubin levels were higher in COPD patients with acute exacerbation. It may be an independent biomarker for screening the COPD patients with and without acute exacerbation. However, the findings were obtained in a cross-sectional study, and additional larger prospective studies are required to confirm these findings.
Acknowledgement
The authors would like to thank all individuals who participated in this study. We also appreciate the Clinical Research Development Unit, Ghaem Hospital, Mashhad University of Medical Sciences to facilitate the data analysis. This work was approved by the Ethics Committee of Mashhad University of Medical Sciences (IR.MUMS.MEDICAL.REC.1400.173), and conducted as Research Project No.991935, as an Internal Medicine Residency thesis.
Conflict of Interest
The authors declare that they have no conflict of interest.