Document Type : Original article
Abstract
Background: This study aimed to investigate the effectiveness of volleyball exercises on executive function and daily living skills in schizophrenia.
Methods: In this randomized study, 28 individuals with schizophrenia participated. The intervention was volleyball exercises for two months. The Functional Independence Measure, The Lawton instrumental activities of daily living scale, and Loewenstein Occupational Therapy Cognitive Assessment battery tests were used in this study. Repeated measures and effect size were utilized for analysis.
Results: Volleyball exercises improve cognitive function and Activities of Daily Living (ADLs) in the intervention group in the following: group effect, time effect, and group and time interaction. They were significant respectively (p-value1=0.041, p-value2=0.001, p-value3=0.001, Cohen’s d=1.267,1.266), (p-value1=0.001, p-value2=0.001, p-value3= 0.001, Cohen’s d=3.967,3.749). With this intervention, no significant difference was observed between the control and intervention groups in instrumental activities of daily Living.
Conclusion: Volleyball exercises improve executive function and ADLs in individuals with schizophrenia.
Keywords: Activities of daily living, Cognitive function, Instrumental activities of daily living, Schizophrenia, Volleyball
Introduction
Schizophrenia or schizophrenia spectrum disorders is one of the most damaging mental disorders that develops slowly and is debilitating (1,2). In this disorder, without treatment personality is often disrupted, reality is distorted, and one’s functioning in everyday life is impaired (3). Symptoms often appear before the age of 19 (4), which are considered as the critical years of a person’s social and educational/career development (5). Schizophrenia encompasses a wide range of cognitive, emotional, and serious social and functional impairments (6).
Individuals with schizophrenia experience executive dysfunction from the outset (7). Research suggests that executive function deficits in schizophrenia may specifically affect Activities of Daily Living (ADLs) (8). Executive function is a key term for complex cognitive processes that result in consistent and purposeful behaviors (9). The first line of treatment for this disease is antipsychotic drugs that can reduce the positive symptoms of psychosis. Antipsychotics are usually used to relieve positive symptoms such as hallucinations, delusions and thought disorders. However, the drug has little effect on negative symptoms such as lethargy, deficits in cognitive function, loss of emotion, social distancing and general lack of interest in activities (10-12).
Studies have shown that aerobic exercise is effective in improving executive function in populations such as Parkinson’s disease, the elderly, attention deficit hyperactivity disorder and stroke (13-15). A meta-analysis conducted in 2017 found that exercise improves cognitive function in people with schizophrenia, especially in the areas of social cognition, working memory, and attention (16). Another study suggested that future clinical trials should determine the appropriate method, intensity of exercise, and duration of aerobic exercise in schizophrenia (17). Beebe et al examined the effect of exercise on the mental and physical health of patients with schizophrenia. In this study, the participants took part in a 16-week walking program, which showed positive effects on physical fitness and psychological symptoms (18). Acil et al investigated the effects of physical exercise on the mental status and quality of life of 30 individuals (two groups of 15 people) with schizophrenia. Aerobic exercise was designed by sports and physical education experts so that participants could exercise in daily life. These exercises were performed for 10 weeks, 3 days a week and for 40 minutes every day. The results demonstrated that mild-to-moderate aerobic exercise is an effective program to reduce psychiatric symptoms and increase the quality of life in people with schizophrenia (19). Su et al examined the effect of aerobic exercise on cognition of people with schizophrenia, who participated in a 12-week program of running and stretching exercises; the results indicated that physical activity has beneficial effects on cognition (20). There exists scientific evidence that represents physical activity and exercise have an important role in the treatment of schizophrenia (21).
In Occupational Therapy (OT), it is believed that sport as a recreational occupation has positive effects (22). In general, physical activity plays a very important role in the participation of people with mental health problems, and occupational therapists use it as a valuable tool for promotion of mental health (23-26). Studies have demonstrated that group sports are more exciting (27) and will be more enjoyable if done competitively (28). Therefore, in this study, volleyball was chosen, due to its popularity, accessibility, physical demands, and competitiveness (29). Volleyball is considered an aerobic exercise since it requires continuous movement, which can increase the heart rate and improve cardiovascular endurance. Although volleyball has been described as an “interval” sport with both anaerobic and aerobic components, the large aerobic component of elite volleyball play is supported by the high VO2 max value recorded for national team players. Volleyball is aerobic in nature that uses both aerobic and anaerobic energy systems, with a large aerobic component at higher skill levels (30). Interventions that involve physical, mental, and social indicators, such as group exercise, may have a major impact on ADLs due to their effects on cognitive function, physical ability, and psychological aspects (31).
Daily living skills include ADLs and Instrumental Activities of Daily Living (IADLs) (32). Both ADLs and IADLs are primary concerns of occupational therapists working in psychiatric settings where their goals are to improve both occupational performance areas (33). Studies have revealed that although occupational therapy services can be effective in addressing positive and negative symptoms of schizophrenia, there are very few studies about occupational therapy interventions for people with chronic schizophrenia (18). On the other hand, studies are needed that document the effect of aerobic exercises on ADLs and IADLs of people with chronic schizophrenia (34).
Observing symptoms such as inappropriate appearance, failure in personal hygiene and inability to perform self-care activities and as a result, rejection by the society in people with schizophrenia, the question arises as to whether group sports such as volleyball can change cognitive function and ADLs/IADLs. So far, it was found that no study has been conducted with the aim of improving the daily life activities of schizophrenic patients through aerobic exercise. Therefore, the purpose of this study was to investigate the effect of volleyball exercises on cognitive function and daily living skills in schizophrenia.
Materials and Methods
Design
This randomized clinical trial study was conducted for 10 weeks and approved by the Ethics Committee of Tehran University of Medical Sciences (IR.TUMS.FNM.REC.1398.157) and the Iranian Registry of Clinical Trials (IRCT20191102045312N1).
Participants
The participants were selected from an outpatient comprehensive rehabilitation center of chronic psychiatric patients from Nowshahr. The inclusion criteria were as follows: participants with the age range of 20 to 40 years, diagnosed with schizophrenia based on Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria; permission from psychiatric specialist to participate; absence of static/dynamic balance issues, cardiovascular disease, pulmonary illness, or other systemic pathologies contraindicating exercise without monitoring physiological variables; an intelligence score above 70 based on the adult version of the Wechsler scale listed in the patients’ medical record; and not having any medication changes three months before the intervention. The exclusion criteria included lack of cooperation of the participants in the study. Ethical consent was obtained from all the participants. Prior to the intervention, the psychiatrist assured the researcher that volleyball was safe for individuals and there were no side effects for them.
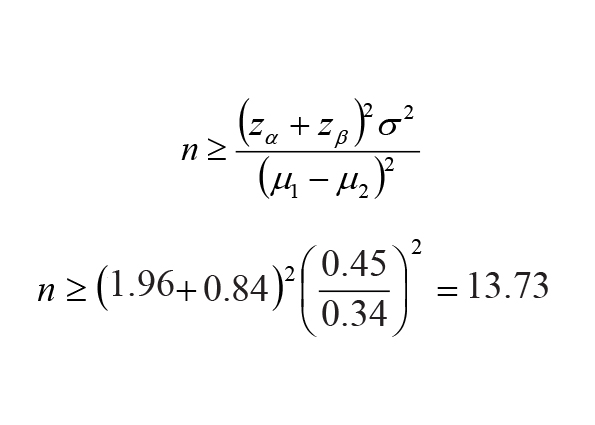
The sample size was considered using the following formula (35) and values and for each group (18), and 14 individuals were considered for the control and intervention groups.
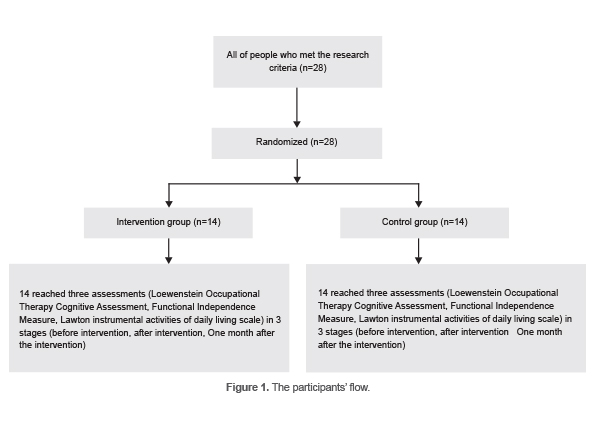
The participants (n=28) with an age range of 20 to 40 years were selected conveniently and according to the inclusion criteria (Figure 1). Their names were placed separately in 28 envelopes and were coded. These coded envelopes were used for randomization into intervention and control groups. Participant registration and randomization were performed by an occupational therapist that performed the evaluations.
Intervention
The control group received standard OT, including purposeful, creative, and recreational activities (gardening, making handicrafts with used items and, artistic activities) that were performed by the trained occupational therapist. The participants were blind to the therapies they received (36). Blinding of the participants meant that they were unaware of allocation. To achieve this goal, the participants were told in advance that they would be assigned to one of the two groups of volleyball or routine treatment, but they did not know in which of these two groups they would be assigned.
The intervention group performed volleyball exercises in addition to their standard OT interventions. In this study, we did not mean the volleyball game or sport, but the exercises/movements related to volleyball that was performed in two groups with a ball to associate as closely as possible with actual occupational engagement.
Volleyball exercises were held for 60 minutes, three days a week, for 2 months (24 sessions for each subject). Each volleyball session consisted of three parts (total 60 minutes): 5 minutes of warm-up (stretching), 45 minutes of playing volleyball exercises (1 set of 20 minutes doing volleyball movements individually, 5 minutes break, and again 1 set of 20 minutes doing volleyball but in two separate and competitive groups as a sport), and 10 minutes of cool-down (slow walking and stretching) (Table 1).
Table 1. Detailed interventions
|
Group |
Interventions |
||
|
Control group |
Standard OT |
||
|
Intervention group |
Standard OT + |
5’ warm-up |
|
|
45’ playing volleyball exercises |
20’ volleyball movements individually (5’ forearm pass, 5’ overhead pass, 5’ spike, 5’ serve |
||
|
5’ rest |
|||
|
20’ the same movement as above but competitively in two groups as a sport |
|||
|
10’ cool-down |
|||
Warm-up and cool-down exercises were suggested to reduce injury, increase athletic performance, and increase joint range of motion (37).
Before starting the intervention, the participants were trained by an experienced volleyball coach and learned the simple rules and the movements (forearm pass, overhead pass, spike, serve) used in volleyball. The active engagement of the participants in each part of the intervention was also carefully monitored by the occupational therapist throughout the intervention.
For the competitive part, the participants were told that the occupational therapist would calculate each team’s score, in case the ball hit the ground in any group, points were given to the opposite group and finally, the winning group would be encouraged. The participants were encouraged to do the best efforts.
It is necessary to mention the duration of the standard OT and rehabilitation services that the participants had received was the same in both intervention and control groups before the intervention.
Outcome measures
The evaluation was performed by an occupational therapist that monitored the participants and evaluated them three times. The evaluations were carried out in two groups, before the intervention, immediately after the intervention, and one month after the intervention as follow up. The outcome measures are as follows:
Functional Independence Measure
The test has 18 items that measure physical, psychological, and social performance. Items assessed using the FIM comprise bowel and bladder control, transfers, locomotion, social cognition, communication, cognition and six self-care activities including eating, grooming, bathing, dressing - upper body, dressing - lower body, and toileting. A score of 1 to 7 applies to each item. A score of 1 means complete dependency and 7 means complete independence. Internal consistency and inter rater reliability of the Persian version has been reported as excellent (38). The total score for the FIM instrument (the sum of the motor and cognition subscale scores) ranges from 18 to 126. The total score for the motor subscale ranges from 13 to 91, while the total score for the cognition subscale ranges from 5 to 35 (39). There is no specific cut-off point for the two sections of the FIM. This test was printed separately for each participant and was completed by the examiner according to the abilities of the participants.
Loewenstein Occupational Therapy Cognitive Assessment
The LOTCA test is used to evaluate cognitive function (40,41). LOTCA consists of 27 sections that examine seven areas of time and space perception (orientation), visual perception, spatial perception, motor praxis, visuomotor organization, mental operations and attention. The subtests refer to the areas, and there are a total of seven areas in the LOTCA assessment that are scored from 1 to 8 in orientation items and from 1 to 4 in other items. A higher score indicates better performance. In this test, the minimum score is 27 and the maximum score is 119, and it takes about 30 to 45 minutes. For all the subtests, inter-rater reliability is from 0.82 to 0.97 (42). The Persian version of the LOTCA test is a valid and useful tool for assessing cognitive dysfunction in adults with schizophrenia (43).
Lawton test
The Lawton test is useful for evaluating IADL. It takes 10 to 15 minutes to complete and consists of 8 items, including phone use, shopping, food preparation, housekeeping, laundry, public transportation, medication management and money management, with scores ranging from 0 to 8. A higher number indicates better performance (44). This paper and pen test was completed for each participant by the examiner. The Persian version of this test shows high validity and reliability (45).
Statistical Analysis
In this study, SPSS software version 26 was used for the statistical analysis. Repeated measurements Analysis of Variance (ANOVA) were utilized to evaluate the long-term effects of the experiment. To use this method, FIM, LOTCA, and Lawton were performed on the subjects three times. In the repeated measurements ANOVA, the means of multiple tests are compared to evaluate the effectiveness of the test and its persistence over time. p-value 1: Comparison between the groups by repeated measures method, p-value 2: Comparison between the times with repeated measurement method. p-value 3: Comparing the group and time interaction with repeated measures method (46,47). The size of the interventional effect was obtained by calculating Cohen’s d effect size. Cohen’s d indicating a small (0.2), medium (0.5), or large (0.8) difference.
Results
Twenty-eight people with schizophrenia participated in the study. Fourteen were female, and 14 were male. The mean age did not differ significantly between the two groups (Table 2). None of the subjects had university degrees, and their highest level of education was high school. All of them were unemployed. Descriptive data related to research variables are shown in table 3.
Table 2. Age characteristics in two groups of intervention and control
|
Variable |
Group |
Number |
Mean |
SD |
p-value |
|
Age (year) |
Intervention |
14 |
31.8571 |
3.63439 |
0.763 |
|
Control |
14 |
32.2857 |
3.81149 |
Table 3. Descriptive indicators related to research variables
|
Variables |
Mean±SD |
|
|
Intervention Group |
LOTCA score before intervention |
93±5.129 |
|
LOTCA score after intervention |
106±4.608 |
|
|
LOTCA follow up |
107±4.899 |
|
|
FIM score before intervention |
106.57±2.593 (motor:87.642, cognitive:18.714) |
|
|
FIM score after intervention |
117.71±2.163 (motor:89.928, cognitive:27.857) |
|
|
FIM score follow up |
119.28±2.223 (motor:89.928, cognitive:29.500) |
|
|
Lawton score before intervention |
5.43±0.756 |
|
|
Lawton score after intervention |
6.71±0.469 |
|
|
Lawton score follow up |
6.71±0.469 |
|
|
Control group |
LOTCA score before intervention |
93.43±7.562 |
|
LOTCA score after intervention |
98.43±7.079 |
|
|
LOTCA follow up |
99.14±7.284 |
|
|
FIM score before intervention |
106.5±2.409 (motor:87.428, cognitive:18.071) |
|
|
FIM score after intervention |
108.07±2.673 (motor:87.428, cognitive:20.071) |
|
|
FIM score follow up |
108.21±2.636 (motor:87.428, cognitive:20.428) |
|
|
Lawton score before intervention |
6.21±0.579 |
|
|
Lawton score after intervention |
6.43±0.646 |
|
|
Lawton score follow up |
6.50±0.650 |
|
LOTCA: Loewenstein Occupational Therapy Cognitive Assessment, FIM: Functional Independence Measure
The information in this table represents the mean and standard deviation of the scores of each variable in the two intervention and control groups. The scores increased in both groups.
In this study, we sought to answer the question of whether volleyball exercises affect cognitive function, ADLs and IADLs. For this purpose, repeated measures analysis was used to analyze the results of the LOTCA test, FIM test, and Lawton test, and the magnitude of the effect was calculated using Cohen’s deffect size.
The results of repeated measures test showed that the p-values in all three comparisons, the effect between groups, the effect of time, and the interaction of time and group were less than 0.05. The contrast test was conducted to compare the results between the two time points, with the “before vs. after intervention” set as the reference. The results revealed that the difference in means between “before vs. follow-up” (F value=74.58, p-value<0.001) and “after vs. follow-up” (F value=21.51, p-value<0.001) was significantly different compared to the reference.
In the pre-intervention stage, the Cohen index has become negative and very low value, which indicates very similar means between the two groups. However, in the post-intervention stages and one month after the intervention, the Cohen index is positive and greater than 0.8, which indicates the positive effect of volleyball on participants’ cognitive function (Table 4).
In table 5, the p-values in all the three comparisons, the effect between groups, the effect of time, and the interaction of time and group are less than 0.05. As in the previous analysis, the contrast test was done. The results indicate that there was a significant difference in the means of “before vs. follow-up” and “after vs. follow-up” in comparison with the reference of before vs. after intervention in the intervention group (F value= 187.18, p-value<0.001 and F value=36.83, p-value<0.001, respectively). It can be concluded that all the three comparisons are meaningful. In other words, volleyball exercises are effective in improving the ADLs of people with schizophrenia. In the pre-intervention stage, the Cohen index is less than 0.8, which demonstrates that there is a weak difference between the means of the two groups, but in the stages after the intervention and one month after the intervention, the Cohen index is positive and greater than 0.8, which indicates the positive effect of volleyball exercises on the ADLs of the participants (Table 5).
Based on the results of repeated measures test, the effect of group is not significant, but the effect of time and the interaction of time and group are significant. The results of contrast test showed that the means’ difference of before vs. follow-up in comparison of the means’ difference of before vs. after intervention was statistically different (F value=38.36, p-value<0.001); however, the comparisons of the means’ differences of after vs. follow-up and the means’ difference of before vs. after intervention was not significantly different (F value=1.00, p-value=0.327).
This means that the exercises could not make a significant difference between the intervention and control groups in terms of IADLs, but over time (i.e., before, after the intervention and one month after the intervention) there was a significant change in IADLs in the entire sample. The results suggest that the interaction between time and group was significant, and the effect size of the Lawton test was positively impacted by the intervention. However, the magnitude of the effect was considered weak (Cohen’s d <0.8) one month after the intervention (Table 6).
Table 4. Result of repeated measures test of LOTCA
|
Cohen Index(d) |
F value p-value3 |
F value p-value2 |
F value p-value1 |
Min |
Max |
SD |
Mean |
Group |
LOTCA test |
|
- 0.067 |
672.31 <0.001 |
124.70 <0.001 |
4.62 0.041 |
79.00 |
103.00 |
7.56 |
93.43 |
Control |
Before intervention |
|
85.00 |
100.00 |
5.13 |
93.00 |
Intervention |
|||||
|
1.267 |
85.00 |
107.00 |
7.08 |
98.43 |
Control |
After intervention |
|||
|
98.00 |
112.00 |
4.61 |
106.00 |
Intervention |
|||||
|
1.266 |
85.00 |
109.00 |
7.28 |
99.14 |
Control |
Follow up |
|||
|
98.00 |
113.00 |
4.90 |
107.00 |
Intervention |
p-value1: Comparison between groups with repeated measures method, p-value2: Comparison between time with repeated measurement method, p-value3: Comparison of group-time interaction with repeated measures
Table 5. Result of repeated measures test of FIM
|
Cohen Index(d) |
F-value p-value3 |
F-value p-value2 |
F value p-value1 |
Min |
Max |
SD |
Mean |
Group |
FIM test |
|
0.027 |
150.71 <0.001 |
192.24 <0.001 |
92.65 <0.001 |
101.00 |
110.00 |
2.47 |
105.50 |
Control |
Before intervention |
|
102.00 |
110.00 |
2.64 |
106.07 |
Intervention |
|||||
|
3.967 |
104.00 |
113.00 |
2.68 |
107.86 |
Control |
After intervention |
|||
|
114.00 |
120.00 |
1.99 |
117.57 |
Intervention |
|||||
|
3.749 |
105.00 |
113.00 |
2.79 |
108.43 |
Control |
Follow up |
|||
|
115.00 |
123.00 |
2.34 |
119.00 |
Intervention |
p-value1: Comparison between groups with repeated measures method, p-value2: Comparison between time with repeated measurement method, p-value3: Comparison of group-time interaction with repeated measures
Table 6. Result of repeated measures test of Lawton
|
Cohen Index(d) |
F-value p-value3 |
F-value p-value2 |
F-value p-value1 |
Min |
Max |
SD |
Mean |
Group |
Lawton test |
|
1.087 |
16.42 <0.001 |
36.04 <0.001 |
0.24 0.627 |
5.00 |
7.00 |
0.58 |
6.21 |
Control |
Before intervention |
|
4.00 |
7.00 |
0.76 |
5.43 |
Intervention |
|||||
|
0.408 |
5.00 |
7.00 |
0.65 |
6.43 |
Control |
After intervention |
|||
|
6.00 |
7.00 |
0.47 |
6.71 |
Intervention |
|||||
|
0.281 |
5.00 |
7.00 |
0.65 |
6.50 |
Control |
Follow up |
|||
|
6.00 |
7.00 |
0.47 |
6.71 |
Intervention |
p-value1: Comparison between groups with repeated measures method, p-value2: Comparison between time with repeated measurement method, p-value3: Comparison of group-time interaction with repeated measures
Discussion
In this study, the effect of volleyball on cognitive function, ADLs, and IADLs in people with schizophrenia was evaluated. There have been some studies on the effect of aerobic exercise on cognitive function in people with schizophrenia (16,17,20). but so far, no study has been conducted on the effect of volleyball exercises on cognitive function, ADLs, and IADLs of this population.
The results of this study revealed that volleyball exercises for 2 months have a large effect on cognitive function and ADLs and a small effect on IADLs of people with schizophrenia.
In this study, it was found that volleyball exercises could affect the cognitive function measured by LOTCA, which was consistent with a number of previous studies that examined aerobic exercise on the cognitive functions (18,19,20).
Exercise, especially aerobic exercise, is thought to have a positive effect on cognitive and brain function, including learning, processing, executive function, and storage. Cognitive function is the process of thinking to conceptualize, recognize, and process stimuli, one of the most important aspects that must be maintained and strengthened for a healthy, disease-free lifestyle (48). Cardiovascular stimulation during exercise is associated with changes in the temporal lobes, forehead, hippocampus, and amygdala, as well as the cerebellum and brainstem, indicating increased parasympathetic activity. Therefore, exercise may facilitate the cognitive function by stimulating the autonomic nervous system (49) and can also increase the concentration of hemoglobin in oxygen in the frontal cortex, activate the nerves in the brain, and thus improve the cognitive function (50). Exercise improves mood and psychological well-being, reduces psychological stress, anxiety and depression (51). Exercise can also affect mood through the release of noradrenaline in the central nervous system, which indirectly improves cognitive function (52).
According to the results of the FIM test and the interpretations made in the present study, improvements in memory, social perception and communication have improved ADLs. In this regard, Kongart et al reached a similar conclusion to the results of the current study (31).
Exercise is associated with an increase in hippocampal neurons, strengthening cognition, memory and reducing anxiety, thus having a positive effect on the brain (49,53). Studies show that the ADLs and IADLs of people who exercise are sometimes better than those who do not (30). Likewise it has been proven that volleyball exercises can be effective in improving motor function in patients who have had a stroke (54). Using gross motor activities can help break the adduction/internally rotated/flexion motor patterns of those with chronic schizophrenia (55) .
According to the results of repeated measures test, the effect of the group is not significant for IADLs. That is, there is no significant difference between the control and intervention groups in terms of the rate of changes in IADLs scores. IADLs requires more sophisticated cognitive skills than ADLs (56), thus making appropriate changes in IADLs skills that can lead a person to independence and improve their quality of life is more difficult and time-consuming than ADLs. Managing the life needs a variety of skills, including money and medicine management, household chores, and food preparation planning. These skills require training and cognitive abilities to master (57). On the other hand, the families of individuals with schizophrenia often do not provide their family member with schizophrenia with tools such as knives, scissors, etc. hence these people are not able to carry out IADLs within their everyday lives. According to the results, the p-value2 became significant. That is, it is true that there were no significant changes between the groups, but over time in the entire sample, regardless of the type of group, there were significant changes.
It can be stated that occupational therapists can use volleyball exercises in their rehabilitation interventions in the field of psychiatric disorders to improve the cognitive function and the ADLs of people with schizophrenia. Hopefully, these findings can suggest that these kinds of exercises may assist people with schizophrenia to be more independent, to increase their participation in their social life and therefore, and be more accepted by the community. Families may be encouraged to enable their family members with schizophrenia to go to the club a few days a week to play volleyball so that exercise becomes a daily routine and can have lasting positive effects on this population.
Limitations and Suggestions
The limitations of this study included the sampling which was a convenience sampling, and the sample was not randomly selected. Measures used may not have been sensitive to changes e.g. the Lawton test is not sensitive to small changes (44). Other measures may have provided more specific information such as the Assessment of Motor and Process Skills (AMPS) or the Independent Living Scales. Also, it was not possible to make this study double blind. On the other hand, if the intervention had been longer, more changes would have made and stronger results could be obtained. Besides, other characteristics of the participants were not collected. Other characteristics, to be considered, include length of illness, length of treatment, symptom severity, physical fitness, physical activity history, interest in sports, previous exposure to volleyball, etc.
Suggestions would be for a larger study carried out at multiple sites, and alternative measures which may be more sensitive to changes. In this study, volleyball was considered as an intervention. It is suggested that in future research, a comparison of resistance exercise (such as upper/lower extremity muscle strengthening) and aerobic exercise (such as volleyball) in improving cognitive function and ADLs/IADLs of people with schizophrenia be done (31). With this research in the future, it might be revealed that resistance training alone or in combination with aerobic exercise can make significant positive changes in the daily living activities of people with schizophrenia. Further studies are required to monitor oxygen consumption or heart rate during volleyball in this population. Also, research can be conducted on the role of motivation and interest in volleyball to explore the specific mechanisms behind these effects.
Conclusion
This study was conducted to evaluate the effectiveness of volleyball exercises on cognitive function and ADLs/IADLs of people with schizophrenia. According to the findings, likely, volleyball exercises can be considered to have a positive impact on cognitive function and ADLs of people with schizophrenia.
This study is a part of the thesis at the master’s degree in Occupational Therapy, supported by the Tehran University of Medical Sciences with code of ethics Committee (IR.TUMS.FNM.REC.1398.157). We would like to thank people with schizophrenia who participated in this study for their kind cooperation.
Practice implications
- Volleyball exercises are a fun and engaging sport which can improve cognitive function in people with schizophrenia.
- Volleyball exercises can make significant changes in ADLs, but it does not appear to affect IADLs.
Acknowledgement
This article is a part of the thesis at the master’s degree in Occupational Therapy, supported by the Tehran University of Medical Sciences. We would like to thank people with schizophrenia who participated in this study for their kind cooperation.
Ethical Approval
This clinical trial study conducted for ten weeks (eight weeks of intervention and two weeks of evaluations) and approved by the Ethics Committee of Tehran University of Medical Sciences (IR.TUMS.FNM.REC.1398.157) and the Iranian Registry of Clinical Trials (IRCT20191102045312N1).
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of Interest
There was no conflict of interest in this manuscript.