Document Type : Original article
Abstract
Background: Repairing the inguinal hernia with mesh using the Lichtenstein method is safe, with a high success rate and low recurrence. Still, there is a potential risk of damage and entrapment of the ilioinguinal and iliohypogastric sensory nerves. This study aimed to investigate the outcomes of the patients after modified Lichtenstein hernia repair surgery.
Methods: This cross-sectional study was conducted on 35 male patients referred to Poursina Hospital with complaints of inguinal hernia who underwent a modified Lichtenstein hernia repair procedure. The demographical data, clinical characteristics, and the outcomes of the patients were recorded. A visual Analog Scale (VAS) evaluated pain scores after surgery, and the data was analyzed using SPSS version 24.
Results: The mean age of the patients was 50.65±14.44 years. Surgery duration averaged 41.17±14.97 minutes, and most patients had indirect hernias (71.4%), with a 57.2% occurrence on the right side. No intraoperative complications occurred, and only one patient experienced postoperative complications. No hernia relapses were reported, and the mean pain score was 0.38±0.07, according to the VAS. Patients returned to work in an average of 2.90±0.98 days, with 45.7% returning after three days.
Conclusion: Findings illustrated that the modified Lichtenstein surgery procedure can treat inguinal hernia due to its fewer postoperative complications.
Keywords: Cross-Sectional Studies, Herniorrhaphy, Inguinal hernia, Return to Work, Surgical Mesh
Introduction
Inguinal hernias are common worldwide, affecting individuals of all ages. The prevalence of inguinal hernias exhibits considerable geographical and demographic variation, with higher rates observed among males and upper ages (1,2). Inguinal hernia repair is one of the most commonly performed surgical procedures globally, presenting a significant burden on healthcare systems and impacting the quality of life for affected individuals (3,4). The etiology of inguinal hernias is multifactorial, encompassing both congenital and acquired factors. Predisposing factors include increased intra-abdominal pressure, connective tissue weakness, anatomical variations, and prior surgical interventions. While the precise pathogenesis remains incompletely understood, it is widely accepted that a combination of genetic predisposition and environmental triggers contributes to developing inguinal hernia (5,6).
Various surgical techniques exist for repairing inguinal hernias, with historical emphasis placed on primary repair methods that have proven effective. However, the advent of artificial meshes has established mesh-based repair as the gold standard approach for inguinal hernia surgery due to its ability to prevent hernia recurrence (2,7). Among the available techniques for hernia repair, the modified Lichtenstein method has emerged as a cornerstone approach, renowned for its efficacy and durability. This technique, which involves tension-free mesh placement to reinforce the weakened abdominal wall, has garnered considerable attention for its favorable outcomes and low recurrence rates (8–10).
Nonetheless, this method could potentially damage and entrap the ileoinguinal and ileohypogastric sensory nerves. Failure to explore and exercise caution during mesh fixation can result in severe postoperative neuralgia, sometimes necessitating surgical nerve block interventions (11,12). Evaluating patient outcomes after inguinal hernia repair is crucial for determining surgical interventions’ effectiveness and long-term success. While the modified Lichtenstein procedure is widely recognized for its reproducibility and favorable outcomes, further investigation is required to confirm (13–15). This study aimed to address this gap by investigating the outcomes of patients with an inguinal hernia who underwent modified Lichtenstein hernia repair procedure in Poursina Hospital, Rasht, Iran.
Materials and Methods
Study design
This cross-sectional study was conducted on the data of 35 male patients referred to Poursina Hospital, Guilan University of Medical Sciences, Rasht, Iran, with the complaint of inguinal hernia. All the patients underwent inguinal hernia surgery by performing the modified Lichtenstein procedure. Patients were selected using the census method, and all the individuals gave informed consent to participate in the study. Patients aged 20 to 80 with direct or indirect inguinal hernias were included in the study. Patients with mental illness, incarcerated hernia, scrotal or previous peritoneal surgery, peritonitis symptoms, intestinal obstruction or perforation, presence of focal or diffuse infection, urethral infections, and sepsis were excluded from the study.
Modified Lichtenstein method
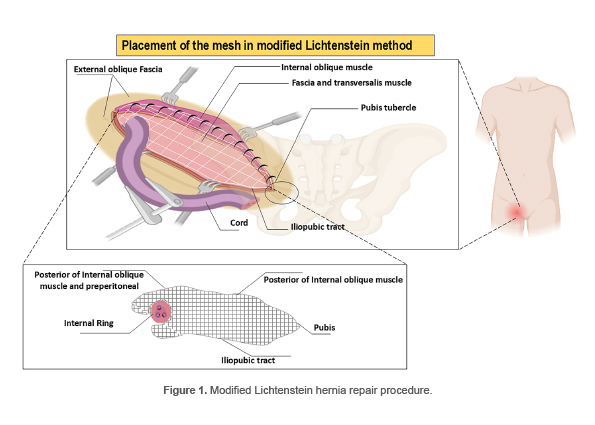
The patients underwent general anesthesia, and the modified Lichtenstein procedure was applied. Considering the anatomy of the inguinal canal and the fixed position of the indirect hernia sac in the anteromedial part of the cord, the operation involved exploring the parietal defects and ligating the hernia sac at the proximal internal ring. The internal ring was then repaired using a mesh, which was extended to the bottom of the canal and anchored to the pubis in a preperitoneal manner. The mesh was placed over the internal muscle after removing the peritoneal covering. Postoperatively, patients were administered intravenous analgesics (pethidine, 25 mg) as needed for pain relief. Figure 1 describes the schematic picture of the procedure.
Data collection
According to the anatomy of the inguinal canal and the fixed position of the indirect hernia sac in the anteromedial part of the cord, after exploring the parietal defects and ligature of the hernia sac in the proximal internal ring, the repair of the internal ring with mesh was performed as a plate mesh by extending to the bottom of the canal to the pubis in a pre-perineal manner and the meshing stage on the internal muscle was removed. Data of the patients, including age, gender, Body Mass Index (BMI), hernia type and side, hospitalization period, anesthesia type, surgery duration, intraoperative and postoperative complications, postoperative pain score, duration of return-to-work, and hernia relapse, was recorded. Postoperative pain was evaluated using a Visual Analog Scale (VAS) score ranging from zero (no pain) to 10 (worst possible pain) (16).
Statistical analysis
Data were reported as number (percentage) and mean±standard deviation (SD). All the data was analyzed using SPSS version 24.
Results
The mean age of the patients was 50.65±14.44 (24-80) years, and the mean Body Mass Index (BMI) was 23.48±1.64 (19.9-26.3) kg/m2. The mean duration of surgery in the operating room was 41.17±14.97 (27-92) minutes. Most patients had an indirect hernia (71.4%), and the frequency of right-sided inguinal hernia was 57.2%. About 91.4% of the patients underwent spinal anesthesia. None of the patients experienced complications during surgery, and only one had postoperative complications (Seroma). Also, no relapse of inguinal hernia was reported. The mean score of pain according to the VAS score was 0.38±0.07 The average duration to return to work was 2.90±0.98 days, and most patients (45.7%) returned after three days (Table 1).
Table 1. The frequency of clinical data of the patients with inguinal hernia who underwent modified Lichtenstein
|
Variables |
Frequency n(%) |
|
|
Type of inguinal hernia |
Direct |
3(8.6) |
|
Indirect |
25(71.4) |
|
|
Both |
7(20.0) |
|
|
Side of inguinal hernia |
Right |
20(57.2) |
|
Left |
11(31.4) |
|
|
Both sided |
4(11.4) |
|
|
Duration of hospitalization |
2 days |
34(97.1) |
|
2<days |
1(2.9) |
|
|
Types of anesthesia |
Spinal |
32(91.4) |
|
General |
3(8.6) |
|
|
Postoperative complications |
No |
34(97.1) |
|
Yes |
1(2.9) |
|
|
Pain score according to VAS |
0.30 |
13(37.1) |
|
0.40 |
16(45.7) |
|
|
0.50 |
6(17.1) |
|
|
Duration of return-to-work |
2 days |
13(37.1) |
|
3 days |
16(45.7) |
|
|
4 days |
3(8.6%) |
|
|
5 days |
2(5.7) |
|
|
6 days |
1(2.9) |
|
VAS: Visual Analog Scale
Discussion
Inguinal hernias often occur due to congenital or acquired factors that lead to a loss of integrity in the abdominal wall musculature (17,18). The modified Lichtenstein procedure provides a durable repair with low recurrence rates and allows for customization based on patient-specific factors (8,10). In the current study, only one patient experienced postoperative complications after Lichtenstein modified hernia repair procedure. Lohsiriwat et al reported that the Lichtenstein method proved to be a secure and efficient procedure for non-strangulated incarcerated inguinal hernias, boasting a recurrence rate of merely 10% within a follow-up duration of six years. They also mentioned that no patients experienced inguinal paresthesia one month after surgery (19).
According to the findings, majority of the patients were in middle age with normal BMI and complained of indirect and right-sided hernia. Similar to our findings, the frequency of unilateral inguinal hernia was reported to be commonly compared to bilateral hernia (8). Goede et al demonstrated that inguinal hernias commonly afflict middle-aged and elderly males, with incidence rising as individuals age. Contrary to the common belief, overweight or obese individuals have a reduced risk of developing inguinal hernias (20). Melwani et al observed that a normal BMI in males exhibited a higher incidence of inguinal hernia chances than a low BMI (21). On the other hand, studies have illustrated that a higher incidence of inguinal hernia among males was significantly associated with age (22,23).
In the current study, the mean duration of Lichtenstein surgery was 41 minutes, and most patients were discharged after two days. A study by Zuvela observed that the mean stay at the surgery unit was 2.5 hours, and the average hospitalization was 1.6 days. They reported that some patients represented postoperative complications during the follow-up (8). Another study demonstrated shorter operation time in the extraperitoneal herniorrhaphy group (49 minutes) compared to open Lichtenstein herniorrhaphy group (54 minutes) and more extended hospital stay in the Lichtenstein herniorrhaphy group (24). Similar to our findings, Vasu and Sagar reported that none of their patients represented postoperative complications after performing the Lichtenstein procedure to repair an inguinal hernia (25).
According to the findings of the present study, the pain score of majority of the patients was less than 5 using VAS scoring, and most returned to work after two or three days. Pedroso et al reported that transabdominal pre-peritoneal laparoscopy patients experienced lower postoperative and chronic pain than those who underwent the Lichtenstein procedure, and no patients experienced recurrent (26). It should be considered that transabdominal pre-peritoneal laparoscopy is a way more expensive method than the Lichtenstein procedure (27). A study by Campanelli et al demonstrated that the Lichtenstein procedure yielded comparable outcomes to expert-led procedures, requiring minimal specialized equipment and offering the flexibility of local anesthesia (28). The results of a meta-analysis illustrated that the laparoscopic approach demonstrated decreased chronic inguinal pain and quicker resumption of regular activities, albeit with notably extended operative durations. However, the decision between laparoscopy and alternative methods remains contingent upon the accessibility of local expertise (29).
This study reported the advantages of applying the modified Lichtenstein hernia repair procedure due to the cost of operation and the economic cost of inguinal hernia, especially in the setting of a developing country, although there are some limitations. Firstly, the study design was cross-sectional, which limited the ability to establish causal relationships or evaluate long-term outcomes. Furthermore, the sample size was small, which may impact the generalizability of the findings. Lastly, the study did not compare different groups or evaluate the performance of the modified Lichtenstein method against alternative surgical approaches, limiting the ability to assess its superiority or inferiority, which has been suggested to be considered in future studies.
Conclusion
The modified Lichtenstein hernia repair procedure is an effective and safe technique with low recurrence rates and minimal postoperative complications. Patients experience minimal pain, quick recovery, and early return to work.
Ethics approval and consent to participate
All the subjects gave their informed consent to participate in the study. This study has been confirmed by the Ethics Committee of the Guilan University of the Medical Sciences, Rasht, Iran (IR.GUMS.REC.1399.561). All the methods followed relevant guidelines and regulations, such as the Declaration of Helsinki.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Acknowledgement
This study was driven from Mohammad Ramezani’s general surgery thesis with registration code 1235.
Conflict of Interest
There was no conflict of interest in this manuscript.