Document Type : Case report
Abstract
Background: Non-ossifying fibroma is a benign fibrohistiocytic bone tumor and occurs mostly in the metaphysis of long bones. Non-ossifying fibroma of the rib is extremely rare.
Case presentation: Herein, a case of a 32-year-old man who was referred for a prolonged cough after an accident was presented. CT scan revealed a well-defined expansile lesion in the right 11th rib. Due to the uncertainty of the diagnosis, a core needle biopsy was taken from
the lesion. The biopsy showed proliferated bland fibroblasts admixed with multinucleated giant cells and hemosiderin deposition. Based on the imaging findings and H&E studies, non-ossifying fibroma of the rib was confirmed.
Conclusion: Although the most common sites of non-ossifying fibroma are metaphysis of long bones, they can occur in any bone. The diagnosis of non-ossifying fibroma is based on radiological findings, and the correct diagnosis in imaging studies reduces invasive procedures.
Keywords: Fibroma, Ribs, Radiology
Introduction
Non-ossifying fibroma was first stated by Jaffe and Lichtenstein in 1942 (1-4). Non-ossifying fibroma is a benign and self-limiting bone tumor. The exact occurrence is unknown due to its asymptomatic and benign nature. Non-ossifying fibroma occurs in 30-40% of children and its peak is in the second decade of life. The most common sites are the metaphysis of long bones and extremely rare in ribs (1-14). Non-ossifying fibroma is twice as much in boys as in girls (1,3-5). The etiology of sporadic non-ossifying fibroma is unclear (1,3). To the best of our knowledge, there are only a few studies on non-ossifying fibroma of rib (1-15). Here, the case of a 32-year-old man with non-ossifying fibroma of rib which was identified incidentally in imaging following an accident, as well as reviewing the literature was reported.
Case report
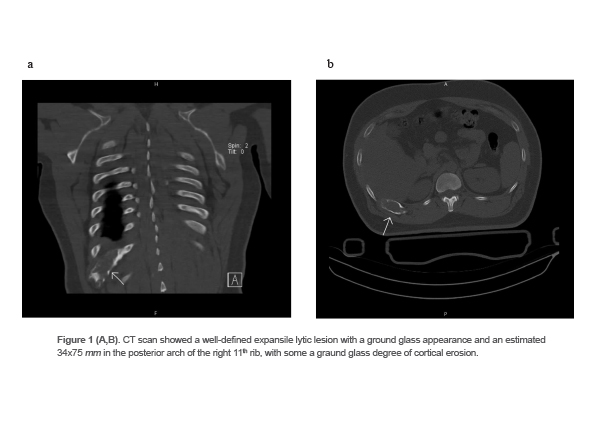
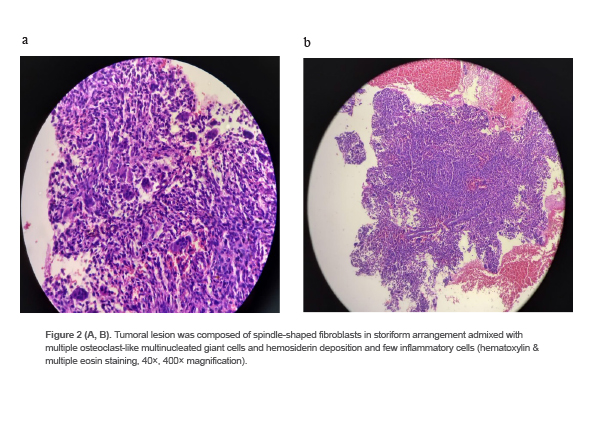
A 32-year-old man was referred to the radiology department with a complaint of a prolonged cough after an accident. The CT scan showed a well-defined expansile lytic lesion with a ground glass appearance and an estimated 34x75 mm in the posterior arch of the right 11th rib, with some degree of cortical erosion. The differential diagnoses in imaging were fibrous dysplasia, lymphoma and metastasis (Figures 1A and 1B). Due to the uncertainty of the diagnosis, a core needle biopsy of the lesion was taken. The specimen consisted of multiple pieces of bony tissues measured together 1×0.1 cm. The histological examination showed bone trabeculae with tumoral lesion composed of spindle-shaped fibroblasts in storiform arrangement admixed with multiple osteoclast-like multinucleated giant cells and hemosiderin deposition and few inflammatory cells (Figures 2A and 2B). Based on the imaging and H&E studies, non-ossifying fibroma of rib was confirmed.
Discussion
Non-ossifying fibroma is the most common benign tumor of the bone and mostly affects children and adolescents, but it has been reported in the age range of 3-42 years. The current case was a 32-year-old man. The most common sites are metaphysis in distal of femur and proximal of tibia, but it is very rare in ribs. Non-ossifying fibroma of rib like elsewhere is usually asymptomatic and is detected in imaging incidentally, but large tumors can cause pain or pathological fracture (1-15). In the study conducted by Blaz et al, out of 28 cases of long bone non-ossifying fibromas that were studied, 27 cases were diagnosed after trauma and 1 case after chronic knee joint pain, and 1 case with pathological fracture was detected (12). In the case series conducted by Rammanohar et al, all of the 5 cases of non-ossifying fibroma of long bones were asymptomatic and detected in imaging studies incidentally (11). Other synonyms for non-ossifying fibroma were fibrous cortical defect, non-osteogenic fibroma, metaphyseal fibrous defect, giant cell variant of bone cyst, xanthic variant of giant cell tumor, healing variant of giant cell tumor, and solitary xanthoma (2-5,8,10). Lesions limited to the cortex are called “fibrous cortical defect” and those extended to the medulla are called “non-ossifying fibroma”. Also, some of them are bilateral or multiple cases that are related to fibrous dysplasia or neurofibromatosis (4).
Although the gold standard for diagnosis of bone tumors is histopathological examination, diagnosis of a typical non-ossifying fibroma is based on the radiological findings (1-14).
In the present case, due to the uncertainty of the diagnosis a core needle biopsy was taken. In X-ray imaging, non-ossifying fibromas were well-defined and radiolucent with a sclerotic margin and tinned cortex and in CT scan, they were lucent with thin sclerotic rim, polycyclic and multiloculated. In MRI that is rarely needed, they were low signal in T1-weighted and intermediate to high signal in T2-weighted images and may reveal septation with variable signal intensity (1-4,10-13). Pyo et al reported a non-ossifying fibroma of rib in a 15-year-old soccer player after blunt trauma while playing soccer.
Radiographic images showed a 2.5 cm cystic lesion in posterior portion of sixth right rib and CT scan demonstrated an expansile cystic lesion (2). In the histopathological examination, they composed of spindle-shaped fibroblasts with storiform pattern, multinucleated giant cells, hemosiderin deposition and foamy histiocytes with mild lymphocyte infiltration (2-6,9-11,13). The differential diagnosis in radiological features include fibrous dysplasia, benign fibrous histiocytoma, Langerhans cell histiocytosis, desmoplastic fibroma, aneurysmal bone cyst, chondromyxoid fibroma and giant cell tumor of bone. The differential diagnosis in histological examination includes benign fibroma, giant cell tumor, histiocytoma, pigmented villonodular synovitis, malignant fibrous histiocytoma and osteosarcoma (1,5,8,11-13). Non-ossifying fibroma regress spontaneously, but for lesions with persistent pain or occupying more than 50% of the bone diameter or longer than 33 mm and lesions with pathologic fracture, surgery is necessary (1-15). Recurrence of non-ossifying fibromas is rare, and malignant transformation has not been reported (4,8,9).
Conclusion
Although the most common sites of non-ossifying fibroma are metaphysis of long bones, they can occur in any bone. The diagnosis of non-ossifying fibroma is based on radiological findings, and the correct diagnosis in imaging studies reduces invasive procedures and imposing additional costs and stress on the patient.
Acknowledgement
The authors are grateful for the cooperation of ethics committee of Yazd Shahid Sadoughi University of Medical Sciences for approving this case report with the code of ethics IR.SSU.REC.1402.066.
Conflict of Interest
The authors declare no conflict of interest.