Document Type : Review article
Abstract
Background: Lower Urinary Tract Disorders (LUTDs) are frequently observed among the pediatric population. Posterior Tibial Nerve Stimulation (PTNS) is a form of neuromodulation that aims to alter the aberrant pattern of nerve stimulation that supplies innervation to the bladder and pelvic floor. The objective of this systematic review was to broaden the scope of investigation on PTNS and evaluate its efficacy in the management of LUTDs in children.
Methods: A systematic search was conducted across seven electronic databases (Scopus, Web of Science, PubMed/MEDLINE, ProQuest, EMBASE, CENTRAL, PEDro) from inception to March 31, 2024, without any language restrictions. The search aimed to identify publications that compared the efficacy of PTNS with anticholinergic medications, urotherapy, sham, placebo, or other interventions for the treatment of LUTDs in children. The primary outcome was symptom improvement, and the secondary outcomes were urodynamic parameters and Quality of Life (QoL). The risk of bias was assessed using the Cochrane Collaboration’s tool.
Results: This systematic review included a total of six clinical trial, comprising 203 children. Merely, single research exhibited an overall low risk of bias, while another one demonstrated an overall unclear risk of bias. The studies evaluated a range of symptoms using various assessment methods or tools and found that PTNS resulted in symptom improvement for different LUTDs. Both arms of the two studies evaluating QoL reported a noteworthy improvement. Moreover, a significant improvement in the majority of urodynamic parameters was reported with PTNS across the studies.
Conclusion: The results of the included studies were in favor of PTNS for the treatment of LUTDs in children. Unified symptom assessment tools, standardized response to treatment criteria, a larger sample size, a lower risk of bias, a minimum number of urodynamic parameters, longer follow-ups, and the occurrence of adverse events should be considered for future clinical trials.
Keywords: Children, Lower urinary tract dysfunction, Posterior tibial nerve stimulation, Systematic review
Introduction
Pediatric urologists frequently encounter the challenge of diagnosing and managing Lower Urinary Tract Disorders (LUTDs) (1). Lowe urinary tract symptoms have been documented to impact 17-22% of the pediatric population. The development of the bladder and lower urinary tract physiological function occurs concomitantly with the growth and maturation of children. Voiding control is typically achieved at approximately five years of age (2,3).
To better understand the reasons and appropriate treatment for enuresis, the International Children’s Continence Society has divided the disorder into two categories: aspects and kinds, primary against secondary and monosymptomatic against non-monosymptomatic (4).
Urinary incontinence is the only sign of monosommatic enuresis. On the other hand, patients with non-monosymptomatic enuresis have urination incontinence along with at least one indication of lower urinary tract symptoms, such as urgency, frequency, or dysuria (4,5).
The treatment of LUTDs in children is of great importance, since these children are more likely to develop urinary disorders such as vesicoureteral reflux and recurrent urinary tract infections. These conditions increase the likelihood of renal scarring (6), which in turn, may progress to kidney failure (7). Moreover, children with LUTDs may experience emotional and behavioral disorders such as anxiety, depression, aggressiveness, and social isolation (8).
The effective management of LUTDs has undergone development alongside the enhanced comprehension of the pathophysiological processes associated with dysfunctional voiding and Overactive Bladder (OAB) in pediatric patients (1). The current emphasis has shifted away from pharmacological interventions, which previously relied heavily on anticholinergic medications and antibiotic prophylaxis. Instead, contemporary approaches prioritize educational initiatives, adequate hydration, management of constipation, and computer-assisted pelvic floor muscle retraining programs (1,9,10).
Neuromodulation, including sacral and tibial nerve stimulation has proven to be effective in the treatment of LUTDs (11). Posterior Tibial Nerve Stimulation (PTNS) is a type neuromodulation that seeks to modify the atypical pattern of nerve stimulation which provides innervation to the bladder and pelvic floor. PTNS generates a modifiable electrical stimulus that traverses through the tibial nerve located in the foot towards the sacral nerve plexus, thereby modulating the bladder and pelvic floor function (12).
The majority of previous systematic reviews and meta-analyses have looked at the efficacy of PTNS in adult patients with various conditions, such as OAB and sexual dysfunction (13-19). A meta-analysis evaluated the effect of neurostimulation therapy, including maximal electrical stimulation, Transcutaneous Electrical Nerve Stimulation (TENS), and PTNS, in children with non-neurogenic OAB (20). Another systematic review and meta-analysis compared the outcomes of parasacral electrical nerve stimulation for the treatment of LUTDs in children and reported the benefits of this therapeutic modality (21). Therefore, it was aimed to expand the inquiry on PTNS and examine its effects in managing LUTDs in pediatric patients.
Materials and Methods
The protocol for this systematic review has been duly recorded in the international prospective register of systematic reviews (PROSPERO) with the code CRD42021250560, which can be accessed at: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=250560. This protocol adheres to the guidelines set forth by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (22).
Study selection criteriai.
PICOS criteria for the study
Population: Male and female patients aged <18 years with LUTDs, including chronic pelvic pain, OAB, neurogenic bladder, non-obstructive urinary retention, urinary incontinence, voiding dysfunction, monosymptomatic enuresis, and painful bladder syndrome comprised the population. Patients with a history of lower urinary tract surgery and concomitant treatment with anticholinergic agents or alpha-blockers were excluded.
Intervention and comparator: The intervention was PTNS, including both percutaneous and transcutaneous PTNS. Studies with two or more arms in which at least one arm received PTNS and sham-controlled trials were included. The comparator was anticholinergic agents, urotherapy, placebo, or any other intervention for LUTDs. PTNS was defined as the placement of electrodes (thin needles) into the skin near the ankle, through which a small electrical current was passed to stimulate the posterior tibial nerve. The studies which applied other interventions along with PTNS in the same arm were excluded.
Outcomes: The primary outcome of this systematic review was improvement of clinical symptoms (urgency, frequency, incontinence, or enuresis) or overall bladder symptoms. The secondary outcomes were Quality of Life (QoL) and urodynamic parameters.
Study design: This systematic review included all the prospective clinical trials that compared the effect of PTNS with anticholinergic medication, urotherapy, sham, or any other intervention, either randomized or non-randomized, with parallel or cross-over designs, single-blind, double-blind, or open-label. Before-after trials with a single arm, case reports, case series, cross- sectional, cohort, and case- control studies, retrospective chart reviews, narrative, scoping, and systematic reviews with/without meta-analyses, study, books and book chapters/sections, animal studies, and study protocols were excluded.
Eligibility criteria
Upon concluding the search, all the citations were imported into the Mendeley Desktop software and any instances of redundant records were subsequently eliminated. The eligibility for inclusion of the primary articles obtained through the search strategy was assessed by reviewing the titles and abstracts. Next, the complete text of the articles that were deemed potentially relevant was independently evaluated by two reviewers. In the event of dissent between the reviewers, a consensus was reached through discussion. Following the failure of the initial reviewers to arrive at a mutual agreement, the ultimate determination was made by a third evaluator, who had greater expertise in the relevant domain.
Search strategy
A systematic search was conducted in seven databases, including Scopus, Web of Science, PubMed/MEDLINE, EMBASE, ProQuest, CENTRAL via Cochrane, and PEDro. The search period was from the inception of each database up to February 31, 2024, and no language restrictions were applied. Furthermore, the IRCTN registry (https://www.isrctn.com/), the National Institute of Health Clinical Trials Register (https://ClinicalTrials.gov/), and the World Health Organization (WHO) ICTRP Search Portal (https://trialsearch.who.int/) were searched to identify unpublished potential studies. (WHO) ICTRP Search Portal (https://trialsearch.who.int/) were searched to identify unpublished potential studies.
The present systematic review extracted pertinent search terms from Medical Subject Headings (MeSH) and Emtree, as well as free text words, based on the population (lower urinary tract disorders) and intervention (posterior tibial nerve stimulation) components. Moreover, an in-depth assessment of pertinent primary studies and reviews was conducted to scrutinize bibliographies for any supplementary relevant studies. Conference papers, theses, and meeting proceedings were searched through Scopus, Web of Science, ProQuest, and annual meetings.
Data extraction
Data extraction was performed by two reviewers independently, utilizing a pre-established extraction form. Following the completion of this process, it was ensured that the extracted data was crosschecked by one of the authors in order to mitigate any potential inaccuracies.
Quality (risk of bias) assessment
The tool developed by the Cochrane Collaboration for evaluating the risk of bias was used to perform a quality assessment (23). This tool examines several parameters, including performance, detection, reporting, and attrition bias, as well as allocation concealment and random sequence generation. The quality assessment was carried out by two authors.
Any discrepancies that arose during the process were resolved through discussion. In cases where agreement could not be reached, a third author was consulted. Research investigations that exhibit a high risk of bias in any of the aforementioned domains were considered to possess an overall high risk of bias. The Cochrane risk of bias tool was utilized as a replacement for PEDro (specified in our PROSPERO protocol). This decision was made due to the Cochrane tool’s more thorough assessment of quality standards, including allocation concealment, random sequence generation, and blinding of the study assessors, when compared to the PEDro tool. The above-mentioned characteristics have been shown to significantly influence the estimates of treatment effects (24).
Statistical analysis
A meta-analysis could not be performed owing to the significant methodological heterogeneity observed in the included studies. Therefore, only a qualitative synthesis of the included studies was carried out.
Results
Identification of studies
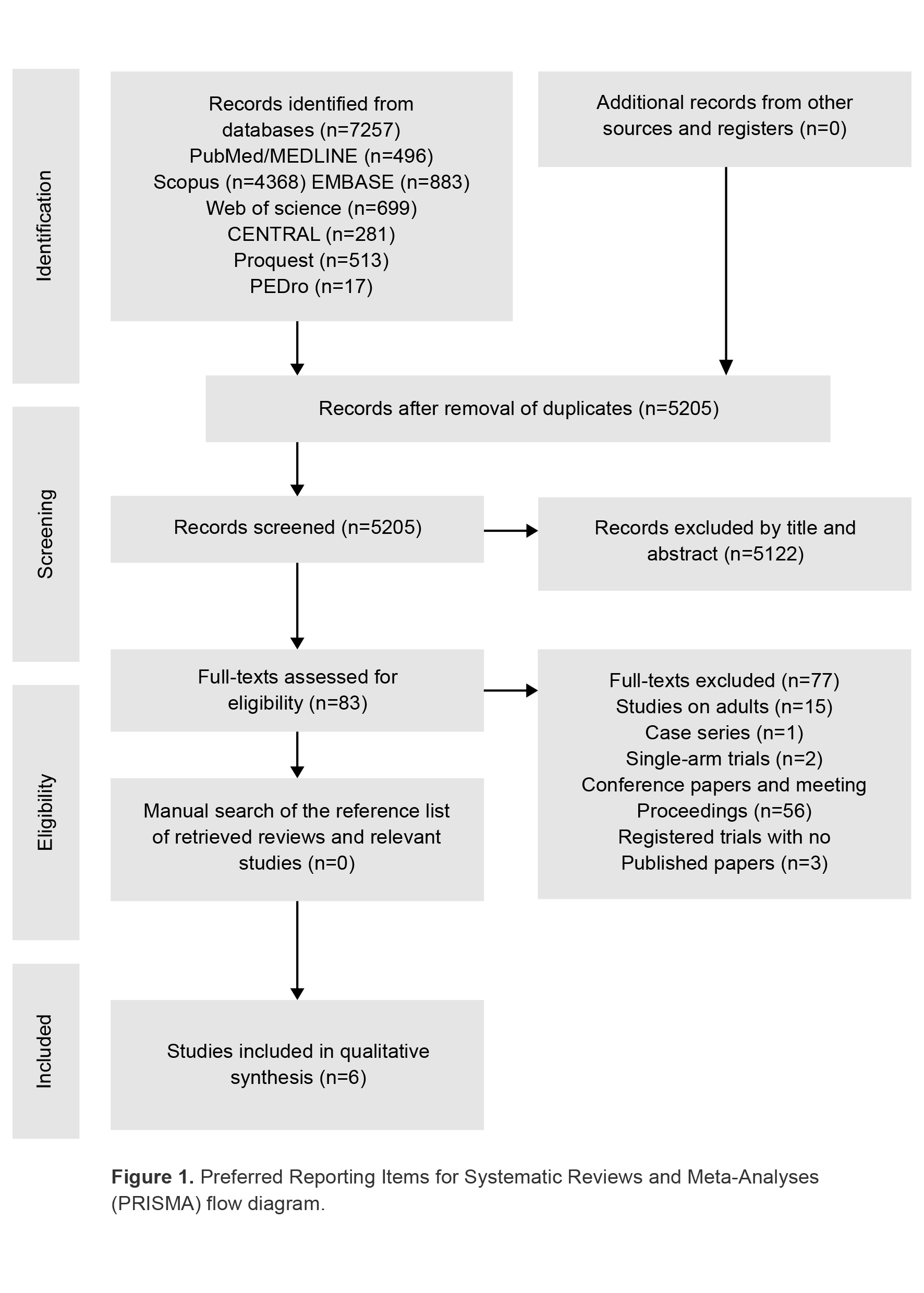
Figure 1 depicts the procedure for study inclusion. The search of databases yielded a total of 7257 publications. Following the removal of duplicates, 5205 publications remained. Subsequently, 5122 publications were excluded based on their titles and abstracts. The eligibility of the remaining studies was evaluated based on their full-text. Upon full assessment of their complete texts, 15 studies were excluded due to their focus on adult participants. One of the publications was a case-series (25), while two were single-arm before-after trials (26,27). There were 56 conference papers and meeting proceedings. Moreover, at three out of four centers, recruitment for the NCT04413461 trial had not yet commenced. The NCT04570605 has concluded its recruitment phase; however, the results have not yet been published. In addition, the recruitment phase of the NCT04256876 trial was terminated due to the COVID-19 pandemic, and only its protocol has been made available to the public (28).
Overview of the included studies
Table 1 provides a summary of the general characteristics of the studies incorporated in the qualitative synthesis. Two studies used percutaneous (29,30) and four transcutaneous PTNS (29-32) in their intervention arm. In the study by Elshafey et al, the patients in the PTNS group also received medical treatment (32). The comparator was sham in all studies with the exception of one (32), in which the control group applied bedwetting and medical treatment.
The duration of PTNS session was 30 mins in all the studies and the treatment duration was 12 weeks except for one study, in which the total treatment duration was two weeks (29). Moreover, the number of sessions ranged from 6 to 36. The patients were assessed in terms of outcome measures in the middle of treatment in Boudaoud et al’s study (31). Two studies evaluated patients after two weeks (33) and within two weeks (30) of the last treatment session, while all others examined outcomes immediately after the last session (27,29,30,32). One study had long-term follow-up of the patients (two years) (33).
A total of 203 pediatric patients were evaluated in the included studies, with sample sizes ranging from 8 to 80. The average age of the patients was 6.32-14 years. The LUTDs treated were monosymptomatic Nocturnal Enuresis (NE) in three studies (29,30,32), OAB in two (2931,34), and dysfunctional voiding in one (33).
Various outcome measures were taken into account across the included studies. Symptom improvement was evaluated by the number of wet nights (30,33), percentage of dry nights (29), incontinence severity (34), incontinence diary (31), NE frequency (32), and daytime episodes of incontinence and urgency (333). Response to treatment was evaluated by the International Children’s Continence Society (ICCS) criteria in the study by Raheem et al (30). A similar response to treatment measure was used in Patidar et al’s study (34). Nevertheless, other studies used recovery from NE (32) and Dysfunctional Voiding and Incontinence Scoring System (DVISS) as response to treatment measures (33). Urodynamic parameters included Post-Void Residual (PVR) volume, bladder pressure, Maximum Voided Volume (MVV), volume at first Overactive Detrusor Contraction (ODC), and maximum ODC pressure. QoL was only assessed in two studies (32,33).
PTNS specifications
The amplitude of the current used for PTNS was 0-25 mA across the studies, while the frequency was set at 10 or 20 Hz, and the pulse width was 200 µs (Table 2). The location of the stimulation electrode was about 2-5 cm cephalad to the medial malleolus. Current intensity was adjusted below the pain threshold in most studies, with the exception of one in which it was set at 1.5 times the threshold for evoking toe fanning and/or plantar flexion (34). Nearly all the studies checked the accuracy of electrode position by means of observing a variety of signs, including curling or flexion of the big toe, fanning of the toes, extension of the foot, tingling sensation, paresthesia along the posterior tibial nerve pathway and the foot arch, and fasciculation of the sural muscle (Table 2).
Table 1. General characteristics of the included studies
|
Author, Year
Country
PTNS group |
Control group (s) |
Condition (LUTD) |
Sample size |
PTNS duration |
PTNS frequency |
Age (years) Mean |
Sex (females) |
Outcome measures |
Follow ups |
Quality assess- ment total score* |
|
Raheem, 2013(30) Egypt Percutaneous PTNS |
Sham |
Refractory primary monosymptomatic NE (unresponsive to conventional and combination therapies) |
28 PTNS (n=14) Sham (n=14)
|
12 weeks |
Once a week (30min) |
PTNS, 13.7 Sham, 14 |
PTNS, 6 Sham, 5 |
Wet nights per week, ICCS response to treatment, void desire (first & strong), MCC,MVV, presence of DO |
Within 2 weeks of the last session 3 months after the last session |
5 |
|
Patidar, 2015(34) India Transcutan eous PTNS |
Sham |
Non-neurogenic OAB unresponsive to behavioral therapy and at least 6 months of anticholinergic treatment |
37 PTNS (n=21) Sham (n=16) |
12 weeks |
Once a week (30min) |
PTNS, 7.71 Sham, 8.38 |
A total of 24 in both groups |
Response to treatment, NV, AVV, MVV |
Immediately after the last session |
2 |
|
Elshafey, 2015(32) Egypt Ranscutaneous PTNS+medical treatment |
Bed- wetting alarm+ medical treat-ment |
Primary monosymptomatic NE |
80 PTNS (n=40) Control (n=40) |
12 weeks |
3 times a week (30min) |
PTNS, 6.32 Control, 6.50 |
PTNS, 19 Control, 23 |
Response to treatment (recovery from NE), frequency of NE, MVV, QoL (KIDSCREEN- 10 Index score) |
Immediately after the last session |
3 |
|
Boudaoud, 2015(31) France Transcutaneous PTNS |
Sham |
OAB resistant to anticholinergic treatment |
20 PTNS (n=11) Sham (n=9) |
12 weeks |
Twice a week (30min) |
PTNS, 11 Sham, 10 |
PTNS, 6 Sham, 4 |
Urinary score, incontinence diary, PVR, volume voided during urgency, maximum cystomanometry volume, maximum bladder pressure, maximum ODC pressure, volume at the first ODC |
At 6 weeks (in the middle of the trial) Immediately after the last session |
6 |
|
Perez- Martinez, 2018(29) Mexico Percutaneous PTNS |
Sham |
Monosymptomatic enuresis unresponsive to first or second line treatments |
8 PTNS (n=4) Sham (n=4) |
2 weeks |
3 times a week (30min) |
PTNS, 10.5 Sham, 10.7 |
A total of 4 in both groups |
Dry nights, urinary volume, adverse effects |
Immediately after the last session |
2
|
|
Jafarov, 2021(33) Turkey Transcutaneous PTNS |
Sham |
Functional voiding disorder (storage phase dysfunction) |
30 PTNS (n=20) Sham (n=10) |
12 weeks |
Once a week (30min) |
PTNS, 101 Months (median) Sham, 101.5 Months (median) |
PTNS, 10 Sham, 5 |
DVISS (total nighttime, daytime), daytime episodes of urgency and incontinence, number of nocturnal Incontinence per week,QoL |
2 weeks after the last session 2 years |
4 |
Lower Urinary Tract Disorders (LUTDs)
Table 2. Specifications of PTNS in the included studies
|
Author, Year |
Device |
Amplitude (mA) |
Frequency (Hz) |
Pulse width (µs) |
Stimulation electrode location |
Earth/negative electrode location |
Threshold |
Position accuracy check |
|
Raheem, 2013(30) |
Urgent® PC Neuromodulation System |
Slow increase up to a tolerable level (pain threshold) |
- |
- |
1 electrode about 5 cm cephalad to the medial malleolus and 1 cm from the posterior margin of the tibia |
Same leg, near the arch of the foot, over the calcaneus |
Pain threshold |
Curling of the largest toe, fanning of digits, or extension of the entire foot |
|
Patidar, 2015(34) |
TENS III stimulator (indigenous machine) |
0-10 |
20 |
200 |
2 electrodes, medial region of the foot, about 3-4 cm cephalad to the medial malleolus between the posterior margin of the tibia and the soleus muscle |
- |
Maximum tolerable level (1.5 times the threshold for evoking plantar flexion of the toes and/or toe fanning) |
Flexion of the big toe, fanning of the toes, or a tingling sensation |
|
Elshafey, 2015(32) |
- |
0-10 |
20 |
200 |
About 2-3 cm proximal to the negative electrode |
Negative, behind the medial malleolus of the same foot |
Pain threshold |
- |
|
Boudaoud, 2015(31) |
- |
10 |
10 |
200 |
2 electrodes, on the pathway of the posterior tibial nerve above and below the medial malleolus |
Earth, over the same area |
Pain threshold |
Perception of paresthesia on the pathway of the posterior tibial nerve and the foot arch |
|
Perez-Martinez, 2018(29) |
EMS+2 (Staodyn) |
1-9 |
20 |
200 |
1 electrode, 3-4 cm cephalad to the medial malleolus of the dominant foot, immediately posterior the edge of the tibia |
- |
Pain threshold |
Plantar flexion of the first toe, fanning out of the toes, fasciculation of the biceps surae, paresthesia in the foot |
|
Jafarov, 2021(33) |
BiolitoTM (MTR+Vertriebs GmbH) |
10-25 and gradually increased by 1 mA intervals |
- |
- |
2 electrodes, proximal part of the medial malleolus between the posterior margin of the tibia and musculus soleus, the other on the plantar region |
- |
Pain threshold |
Flexion of the big toe, fanning of the toes, and tingling |
Quality assessment
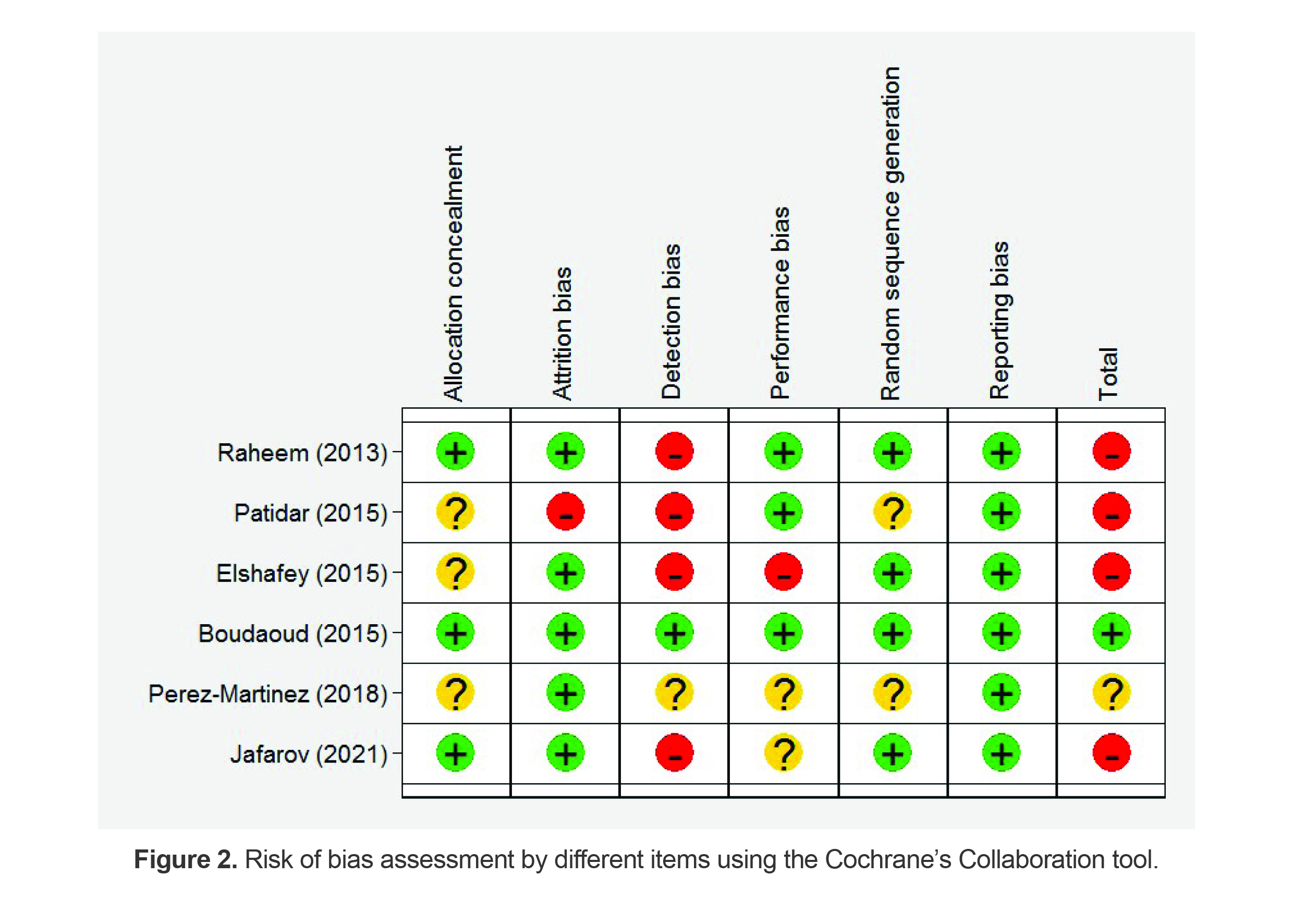
The results of the quality assessment are presented in figure 2. The overall score is reported in table 1. Overall, only one study had a low risk of bias in all categories (31) and the risk of bias was unclear in another (29). All the studies had a low risk of reporting bias. Also, attrition bias was low in all the studies except for one (334). On the other hand, the majority of studies (5/6) had unclear or high risk of detection bias. In terms of allocation concealment and random sequence generation, the risk of bias was either unclear or low. Regarding the performance bias, three studies had a low risk (30,31,34), two had unclear risk (29,33), and one had a high risk of bias (32).
Table 3. The summary of the results of the included studies in terms of primary and secondary outcomes
|
Author, Year |
Wet/dry nights/days |
Response to treatment |
MVV (ml) |
QoL |
Other outcome measures |
Adverse effects |
|
Raheem, 2013 (30) |
Wet nights per week PTNS: 4.7±1.3 before, 2.6±2.2 after (p=0.002) Sham: 5.1±1.4 before, 4.7±2.1 after (p=0.041) After-treatment comparison between groups,p=0.041 At 3 months PTNS: 2.9 Sham: 4.2 (p=0.07) |
Within 2 weeks after treatment* PTNS: 4(28.6%) complete, 7(50%) partial, 3 no response Sham: 2(14.3%) partial, the rest no response (p=0.002) At 3 months PTNS: 2 complete, 4 partial Sham: no change (p=0.13) DO PTNS: 7 patients before, 5 after (p=0.44) Sham: 6 before, 6 after (p=1.0) Between-group comparison, p=0.7 |
PTNS: 266.57±82 before, 280.14±71.81 after (p=0.022) Sham: 288.93±106.29 before, 291.07±96.84 after (p=0.73) Between-group comparison, P=0.6 |
- |
MCC (ml) PTNS: 291.21±86.82 before, 322.5±65.89 after (p=0.000) Sham: 322.21±76.04 before, 323.57±77.44 after (p=0.57) Between-group comparison, p=0.97 Void desire (ml) First PTNS: 148.46±25.89 before, 177.71±35.48 after (p=0.002) Sham: 153.50±21.65 before, 154.14±20.71 after (p=0.59) Between-group comparison, p=0.041 Strong PTNS: 260.43±84.18 before, 283.64±72.03 after (p=0.01) Sham: 271.79±75.43 before, 271.6±72.8 after (p=0.94) Between-group comparison, p=0.67 AVV (ml) PTNS: 68(57-103) before, 89(69-140) after (p=0.001) Sham: 74(49-98) before, 79.5(55-100) after (p=0.088) |
None |
|
Patidar, 2015 (34) |
Incontinence severity PTNS: 0 no, 7(33.33%) mild, 8(38%) moderate, 6(28.5%) severe before; 15(71.42%) no, 5(23.81%) mild, 1(4.76%)moderate, 0 severe after Sham: 0 no, 5(31.25%) mild, 7(43.75%) moderate, 4(25%) severe before; 2(12.5%) no, 5(31.25%) mild, 6(37.5%) moderate, 3(18.75%) after (p<0.001) NV PTNS: 11(10-13) before, 7(6-11) after (p=0.001) Sham: 10(9-13) before, 10(7-12) after (p=0.325) |
PTNS: 14(66.66%) full response, 5(23.81%) response, 2(9.5%) partial response, 0 no response Sham: 0 full response, 1(6.25%) response, 3(18.75%) partial response, 12(75%) no response (p<0.001) |
PTNS: 116(90-205) before, 190(120-300) after (p=0.001) Sham: 110(88-193) before, 45.5 (105.5200) after (p=0.072) |
- |
- |
Not reported |
|
Elshafey, 2015 (32) |
NE frequency PTNS: 5.90±0.41 before, 1.20±0.14 after (p=0.001) Control: 6.30±0.23 before, 3.40±0.35 after (p=0.001) |
PTNS: 35 (87.5%) recovered, 5 (12.5%) not recovered Control: 30 (75.0%) recovered, 10(25.0%) not recovered (p=0.04) |
PTNS: 160±15 before, 192±12 after (p=0.001) Control: 155±14 before, 176±10 after (p=0.110) |
KIDSCREEN -10 Index score PTNS: 1.80±0.04 before, 3.90±0.73 after (p=0.001) Control: 1.56±0.09 before; 2.80±0.05 after (p=0.001) |
- |
Not reported |
|
Boudaoud, 2015 (31) |
Incontinence diary PTNS: 5(45%) poor, 1(9%) medium, 0 good, 5(45%) very good Sham: 3(33%) poor, 0 medium, 0 good, 6(66%) very good (p=0.65) Urinary score PTNS: 5.72±2.14 before, 6.18±4.55 after (p=1.00) Sham: 5.66±3.08 before, 5±3.87 after (p=0.054) Between-group comparison, (p=0.54)
|
|
|
- |
Volume voided during urgency (ml) PTNS: 184.2±102.6 before, 265.6±120.7 after (p=0.002) Sham: 184.4±65.41 before, 181.4±58.06 after (p=0.023) PVR (ml) PTNS: 13.36±25.97 before, 9.81±10.22 after (p=0.83) Sham: 8.44±10.74 before, 13±20.81 after (p=0.70) Maximum cystomanometry volume (ml) PTNS: 215.7±106 before, 274.5±129 after (P=0.024) Sham: 189. 2±69.82 before, 213.3±78.7 after (P=0.77) Maximum bladder pressure PTNS: 18.73±7.69 before, 18.45±8.57 after (p=0.87) Sham: 18.89±6.11 before, 22.56±9.24 after (p=0.20) Maximum ODC pressure PTNS: 61.09±34.37 before, 46±25.1 after (p=0.042) Sham: 56.78±42.62 before, 67.67±39.78 after (p=0.048) Volume at first ODC (ml) PTNS: 48.82±48.76 before, 174.3±139.9 after (p=0.001) Sham: 61.22±33.09 before, 80.22±42.48 after (p=0.0009) |
None |
|
PerezMartinez, 2018 (29) |
Wet nights(%) PTNS: 12.5±7.5 before, 92.5±1.4 after Sham: 6.3±3.7 before, 10±3.5 after Between-group comparison, p<0.001 |
- |
- |
- |
Urinary volume (enuresis) PTNS: 204.3±84.8 before, 110.5±15.5 after Sham: 229.2±91.3 before, 114±15.7 after Between-group comparison, p=0.314 |
PTNS: 2 fear of puncture, 1.5 pain at puncture site, 1.25 bleeding at puncture site, 1.25 pain during PTNS Sham: 1.5, 1.25, 1, 1.25 (p=0.595, 0.374, 0.374, 1.000) |
|
Jafarov,2021(33) |
Wet nights per week PTNS: 3.00±3.24 before, 2.15±3.01 after, 1.35±2.25 long-term, (before vs. long-term: p=0.006) Sham: 1.80±2.39 before, 0.60±0.52 after,0.40±0.70 long-term (non-significant) Daytime episodes of incontinence PTNS: 2.25±2.80 before, 0.70±1.03 after, 0.60±1.66 long-term (before vs. after: p<0.006, before vs. long-time: p=0.049) Sham: 1.50±2.17 before, 0.90±1.59 after, 0.40±0.52 long-time (non-significant) Daytime episodes of urgency PTNS: 4.9±4.9 before, 1.90±2.3 after, 1.9±1.8 long-term (before vs. after: p<0.001, before vs. long-term: p=0.041) Sham: 5.90±6.85 before, 5.20±6.66 after, 3.4±3.80 long-term (non-significant) |
DVISS total PTNS: 15.65±6.73 before, 7.25±6.55 after, 6.20±5.04 long-term (before vs. after: p<0.001, before vs. long-term: p<0.001) Sham: 17.30±8.52 before, 8.10±5.76 after, 5.90±5.44 long-term (before vs. after: p=0.007, before vs. long-term: p=0.013) VISS nighttime PTNS: 4.05±4.03 before, 3.45±3.94 after, 2.65±3.42 long-term (nonsignificant) Sham: 3.80±3.49 before, 3.00±2.58 after, 1.20±2.09 long-term (nonsignificant) DVISS daytime PTNS: 11.50±4.20 before,3.70±4.01 after, 3.55±4.17 long-term (before vs. after: p<0.001, before vs. long term: p<0.001) Sham: 13.50±5.32 before, 5.10±3.57 after, 4.70±3.56 long-term (before vs. after: p=0.005, before vs. long-term: p=0.005) |
- |
PTNS: 1.65±0.99 before, 1.15±1.09 after, 0.85±0.87 long-term (before vs. after: p=0.019, before vs. long-term: p=0.014) Sham: 2.30±0.82 before, 1.20±1.03 after, 0.70±0.67 long-term (before vs. after: p=0.040, before vs. long-term: p=0.007)
|
- |
None |
*Based on the International Children’s Continence Society (ICCS) criteria
Abbreviations: AVV, Average Voided Volume; DO, Detrusor Overactivity; DVISS, Dysfunctional Voiding and Incontinence Scoring System; MCC, Maximum Cystometric Capacity; MCV, Maximum Cystomanometry Volume; MVV, Maximum Voided Volume; NE, Nocturnal Enuresis; NV, Number of Voids daily; ODC, Overactive Detrusor Contraction; PVR, Post-void Residual; QoL, Quality of Life.
Effects of PTNS on symptoms
After treatment, the number of wet nights per week was significantly lower with PTNS compared to sham, as reported by Raheem et al (30); however, after three months, the difference between groups was no longer statistically significant (Table 3). On the other hand, Elshafey et al showed a significant reduction in both the PTNS and control groups in terms of NE frequency but after-treatment results were not compared (32). Another study assessed the percentage of dry nights and reported a significantly higher percentage with PTNS than with sham after treatment (29). The incontinence severity was significantly different between PTNS and sham groups of the Patidar et al’s study after treatment. Likewise, the number of voids daily decreased significantly only in the PTNS group of this study (34). In Jafarov et al’s study, only in the PTNS arm did the number of wet nights per week and daytime episodes of incontinence decreased significantly after intervention and at the 2-year follow-up compared to baseline. The same results were achieved regarding daytime episodes of urgency (33). Contrarily, incontinence diary showed no difference between Sham and PTNS (29). A urinary score of 0 to 13 was developed by Boudaoud et al with higher scores indicating worse conditions (31), which indicated no significant difference between the groups after treatment.
Response to treatment
By using the ICCS criteria, Raheem et al showed a significantly better response to the treatment with PTNS within two weeks after the final treatment session, but not at the 3-month follow-up (30). Similar results were reported by Patidar et al (34). Another study evaluated the proportion of recovered patients (from NE) which was significantly higher with PTNS (32). DVISS total and daytime scores improved significantly in immediate- and long-term compared to baseline in both PTNS and sham groups of Jafarov et al’s study; nevertheless, DVISS nighttime score improvements were non-significant in both groups (33). Furthermore, the number of patients with Detrusor Overactivity (DO) was not different before and after treatment in any of the study arms of Raheem et al’s study, neither was it different after treatment between the two groups (30).
Effects of PTNS on QoL
The two studies evaluating QoL as an outcome measure reported significant improvement in both arms (32,33). Nevertheless, the tool used for QoL assessment was not specified by Jafarov et al (33). Moreover, long-term and immediate QoL were significantly better than baseline values in both groups of this study (33).
Effects of PTNS on urodynamic parameters
MVV was examined in three studies (30,32,34) and all showed a significant increase only in the PTNS arm after treatment. Perez-Martinez et al evaluated the urinary volume which did not differ between the two groups after treatment (29). Average voided volume (AVV) improved significantly with PTNS (34). Other outcome measures in urodynamic studies, cystometric, and cystomanometric evaluations included void desire (first and strong), maximum cystometric capacity (MCC), and maximum cystomanometry volume (MCV), which only improved significantly with PTNS. Volume voided during urgency, maximum ODC pressure, and volume at first ODC improved significantly in both groups (31), while PVR volume and maximum bladder pressure yielded considerable improvement in any of the groups (31).
Adverse effects of PTNS
Three studies showed no adverse effects for PTNS in children (30,31,33), while two did not evaluate the potential unfavorable effects of PTNS (32,34). Pain and bleeding at puncture site, fear of puncture, and pain during PTNS were reported by a number of patients in both the percutaneous PTNS and sham groups of the study by Perez-Martinez (29); nonetheless, the difference between the two groups was not statistically significant.
Discussion
Considering the literature, this systematic review represents the first comprehensive review assessing the impact of PTNS in managing a diverse spectrum of LUTDs among pediatric patients. The studies included in this systematic review looked at different LUTDs, namely OAB, primary monosymptomatic NE, and functional voiding disorder. Symptom improvement was observed with PTNS in the majority of studies compared to sham/control; however, the method of assessment and the type of symptoms differed across studies, potentially depending on the underlying LUTD. According to Fernandez et al’s meta-analysis, neurostimulation therapy was found to probably result in superior partial amelioration of non-neurogenic OAB in children compared with standard urotherapy. Nevertheless, it may not yield a conclusive full response (20).
An earlier systematic review investigated the efficacy of percutaneous PTNS in the treatment of LUTDs (17). In this review, patients with OAB, painful bladder syndrome, nonobstructive urinary retention, neurogenic bladder, chronic pelvic pain, and pediatric voiding dysfunction were evaluated. Yet, the efficacy of PTNS appears to be higher in OAB patients than in other conditions (17). Another review suggested that tibial nerve stimulation can be effective and safe for the management of neurogenic LUTDs (35). Overall, the majority of previous systematic reviews and/or meta-analyses of PTNS have been carried out on adult patients and those with OAB (11,19).
The current study revealed significant improvement in the majority of urodynamic parameters with PTNS compared to sham/control. Urodynamic parameters were also evaluated in the systematic review and meta-analysis by Wang et al who examined the efficacy of percutaneous PTNS for OAB. They reported a significant clinical effect of PTNS on maximum cytometric capacity and compliance and found PTNS to be effective and safe in treating OAB symptoms (13).
The detrusor muscle’s contractility is innervated by the parasympathetic nervous system, specifically through the involvement of sacral nerves S2, S3, and S4. The bladder is comprised of M2 and M3 muscarinic receptors, with M3 being primarily accountable for bladder contractility. Therefore, the utilization of anticholinergic medications was aimed at inhibiting the parasympathetic acetylcholine pathway, resulting in a decrease in the contractile ability of the detrusor muscle (36). The conventional method of percutaneous PTNS involves the placement of a needle above the medial malleolus to activate the posterior tibial nerve, a peripheral branch of the sciatic nerve. Stimulation of the tibial nerve results in the activation of the hypogastric plexus, which in turn activates sympathetic inhibitory neurons while simultaneously inhibiting the pelvic nerve, which is responsible for parasympathetic excitatory neurons. Consequently, the outcome is a decrease in the contractions of the bladder (37,38).
The findings indicated a significant improvement of LUTD symptoms with PTNS applied both percutaneously and transcutaneously. Consistently, the systematic review and meta-analysis conducted by Alomari et al showed no statistically significant difference between transcutaneous and percutaneous PTNS or anticholinergic medication for the treatment of adult OAB patients (15). The results of this study were supported by the inclusion of high-quality clinical trials. Nevertheless, one study in this systematic review which employed percutaneous PTNS reported adverse events associated with the puncture site and needle insertion (29).
The utilization of surface electrodes by transcutaneous PTNS as opposed to needles in percutaneous PTNS may present a more favorable alternative for patients. Moreover, transcutaneous PTNS has the potential to reduce expenses and minimize inconvenience since there is no requirement for skilled personnel or a predetermined delivery schedule (16,39), which is specifically important for pediatric patients. On the other hand, this method can potentially be utilized by patients in the comfort of their own homes, thereby circumventing the expenses associated with travel. In general, this can facilitate patient autonomy and promote individual lifestyle preferences (40). Likewise, although the improvement in QoL observed in two studies of the current systematic review can be attributed to the placebo effect as both groups showed significant improvements, transcutaneous PTNS was the selected method in these studies.
The present study had several limitations. The most important limitation was preclusion of meta-analysis driven by the severe methodological heterogeneity of the included studies and the fewer than minimum number of studies than had reported similar outcomes such as MVV. QoL was also evaluated in two studies, yet the direction of changes was different; increase in the score interpreted as improvement in one study and decrease in the score in another. Accordingly, sensitivity analysis could not be carried out. Moreover, publication bias assessment and subgroups analyses were out of the question. Another limitation was the variety of outcome measures both in terms of symptom improvement and urodynamic parameters, that made qualitative comparison difficult. Furthermore, the effectiveness of percutaneous and transcutaneous PTNS could not be compared in the treatment of LUTDs in children. In addition, had authors adhered to the <10 years of age inclusion criterion outlined in our PROSPERO protocol, the total number of studies would not have surpassed two; therefore, the authors were compelled to disregard this criterion.
Conclusion
The present systematic review demonstrated that PTNS intervention yielded significant improvement in symptoms associated with various LUTDs. The studies assessing QoL indicated a significant enhancement in this regard, yet in both study arms. Furthermore, a noteworthy improvement in the majority of urodynamic parameters was documented through the implementation of PTNS across different studies. Further high-quality clinical trials are required to determine the efficacy of PTNS for the treatment of LUTDs in children. Also, response to treatment evaluations need to be standardized in these clinical trials and a minimum of urodynamic parameters should be assessed in every study. Moreover, longer follow-ups are warranted to pinpoint long-term effects, recurrence rate and maintenance PTNS requirement.
Adverse events should also be noted and reported in future clinical trials. As it is evident, the absence of extensive research and the significant heterogeneity present have hindered the ability to conduct a meta-analysis. Therefore, it is essential to carry out additional randomized clinical trials with larger sample sizes, less risk of bias, evaluation of a wider range of urodynamic parameters, longer follow-ups, and precise documentation of adverse effects to explore the effectiveness of PTNS.
Ethical approval and consent to participate:
The research obtained ethical clearance from the Ethics Committee of Iran University of Medical Sciences, with ethics code: IR.IUMS.FMD.REC.1400.170. The protocol for this systematic review has been duly registered in the international prospective register of systematic reviews (PROSPERO) with the code CRD42021250560, which can be accessed at: https://www.crd.york.ac.uk/prospero/display_record.php? RecordID=250560.
Funding
The current study received no financial support.
Acknowledgement
The diligent endeavors of the staff at the Neuromusculoskeletal Research Center, Iran University of Medical Sciences, Tehran, Iran, are greatly valued. The research obtained ethical clearance from the Ethics Committee of Iran University of Medical Sciences, with ethics code: IR.IUMS.FMD.REC.1400.170. This Research was supported by grant No. 21434 from Iran University of Medical Sciences, Tehran, Iran.
Conflict of Interest
There was no conflict of interest in this manuscript.