Document Type : Original article
Abstract
Background: Noninvasive assessment of arterial stiffness in patients with Coronary Slow Flow Phenomenon (CSFP) could be valuable for evaluating cardiovascular risk. Presystolic Wave (PSW) velocity is considered a predictor of cardiovascular disease and a marker of arterial stiffness. This study aimed to evaluate PSW velocity in patients with CSFP
Methods: This cross-sectional study investigated patients with acute coronary syndrome, dividing them into two groups: Cerebrospinal Fluid (CSF) and Coronary Normal Flow (CNF), with 30 patients in each group. Both groups underwent echocardiography, and PSW velocity was compared between them. Data analysis was performed using SPSS version 24 software.
Results: A total of 60 patients were included in the study. The mean ages in the CSF and CNF groups were 49.8±9.6 and 49.6±10.7 yrs, respectively. In the CSF group, 63.33% were female, compared to 43.33% in the CNF group. There were statistically significant differences in Em and aortic aortic Velocity Time Integral (VTI) among echocardiographic variables (p<0.05). However, PSW velocity did not significantly differ between the CNF and CSF groups (33.6±17.4 vs. 37.8±10.4, p=0.26), though it was slightly higher in slow flow patients.
Conclusion: In this study, no significant difference was found in PSW velocity between patients with slow coronary flow and those with normal coronary flow, and it is not associated with arterial stiffness. Therefore, PSW velocity cannot be used as a predictor of arterial stiffness in CSF patients. Further research is recommended to validate or refute these findings.
Keywords: Acute coronary syndrome, Cardiovascular diseases, Cross-sectional studies, Echocardiography, Heart disease risk factors, No-reflow phenomenon, Vascular stiffness
Introduction
Coronary Slow Flow Phenomenon (CSFP) can occur in the absence of obstructive coronary artery disease and has distinct clinical features and an uncertain prognosis and needs specific treatment (1). It has been shown that approximately 80-90% of patients with Cerebrospinal Fluid (CSF) experience chest pain, with 33% requiring hospital readmission. This condition significantly impacts their quality of life and is associated with a poor prognosis, including an increased risk of ventricular arrhythmias and cardiovascular-related mortality. These adverse outcomes can be severe, potentially leading to sudden death (2). The long-term outcomes and mortality rates for individuals with CSF remain unclear (3). Current understanding suggests that CSF may contribute to myocardial ischemia, linked to factors such as endothelial dysfunction in coronary arteries, inflammatory responses, abnormalities in microvascular reserve function, subclinical atherosclerosis, and genetic factors (4-6).
Conducting invasive procedures like Coronary Angiography (CAG) on asymptomatic patients is often not ethically justified. Hence, alternative methods are needed to accurately assess indices derived from more complex and invasive techniques (7). Noninvasive assessment of arterial stiffness can be valuable for evaluating cardiovascular risk. Arterial stiffness acts as both a structural and functional indicator of the cumulative impact of various cardiovascular risk factors and serves as a proxy endpoint for cardiovascular health, even in asymptomatic individuals without diagnosed Vardiovascular Diseases (CVDs) (7,8). Presystolic Wave (PSW) velocity measurement is considered a predictor of CVDs and a marker of arterial stiffness (9). The PSW is typically observed during the late diastolic phase when using doppler ultrasound to examine the left ventricular outflow tract (10) and may indicate increased arterial stiffness (11).
Recent findings suggest that arterial stiffness is elevated in patients with CSFP (12). Therefore, this study aimed to evaluate PSW velocity in patients with CSFP compared to those with normal coronary arteries to obtain more accurate findings.
Materials and Methods
Participants
In this cross-sectional study conducted at Ghaem Hospital in Mashhad, Iran, during 2023-2024, all patients with acute coronary syndrome (ACS) who underwent CAG as per the guidelines of the American College of Cardiology (ACC) and the American Heart Association (AHA) were investigated. Patients with CSF in any of their three main epicardial vessels, provided they did not have more than 50% occlusion and had a TIMI-corrected slow flow with a frame rate greater than 27 frames/s per second, were included in the study.
Exclusion criteria included coronary artery disease, congestive heart failure, moderate to severe valvular disease, atrial fibrillation, stroke, active infection or inflammatory disease, hypertensive cardiomyopathies, active malignancy, infective endocarditis, congenital heart disease, suboptimal echocardiographic recordings, diabetes mellitus, and elderly patients (age > 70 yrs). Informed consent was obtained from all the participants before the study began.
Data collection
The demographic characteristics of all the patients, including age, gender, underlying conditions [such as Hypertension (HTN) and dyslipidemia (DLP)], smoking status, and Body Surface Area (BSA), were recorded. The patients were then divided into two groups: those with CSF and those with Coronary Normal Flow (CNF), with 30 patients in each group. After confirming the TIMI Frame Count criteria, echocardiography was performed, and the PSW velocity was evaluated for all the patients. The PSW velocities were then compared between the CSF and CNF groups.
During CAG, cranial and caudal views were used, with 6-8 ml of contrast material administered for each view, and 15 frames viewed per second. The TIMI Frame Count Method was employed to diagnose and stage CSFP. The TIMI Frame Count (TFC) was determined by counting the frames between the first and last frames. The first frame is identified when the dye fully enters the artery, meeting three conditions: (I) the dye extends fully or nearly fully across the artery lumen; (II) the dye touches both artery borders; and (III) the dye moves forward. The last frame is when the dye first reaches the distal landmark branch. For the Left Anterior Descending artery (LAD), this landmark is the distal bifurcation (e.g., the “mustache,” “pitchfork,” or “whale’s tail”). In the circumflex system, it is the bifurcation with the longest total distance, and in the Right Coronary Artery (RCA), it is the first branch of the posterolateral artery. Standard coronary angiogram cine acquisition was performed at 30 frames/s per second, but in this study, it was recorded at 15 frames/s. Therefore, the Corrected TIMI Frame Counts (CTFC) were calculated by multiplying the number of frames by 2. Additionally, the CTFC for the LAD was divided by 1.7 due to its increased length (13), as the normal frame counts for the LAD are 1.7 times greater than the mean for the LCx and RCA. A CTFC greater than 27 frames was considered indicative of CSF. The mean corrected TFC was calculated by averaging the sum of the corrected TFCs for each coronary artery. Subjects with a corrected TFC more than 2 standard deviations above the normal range were considered to have CSFP (14).
Echocardiography
Echocardiography was conducted following the standards set by the American Society of Echocardiography. Initially, the patient’s blood pressure was recorded, and the examination was performed using a 3-5 MHz transducer, 10 min after the patient had rested. The Left Ventricular Ejection Fraction (LVEF) was determined using Simpson’s technique (15).
During the echocardiography, several parameters were evaluated and recorded, including LVEF, Mitral Valve flow E wave Velocity (MV E Velocity), aorta velocity (A Velocity), ventricular tissue Doppler early diastolic velocity (Em), aortic valve annulus size (AV annulus), aortic velocity time integral (aortic VTI), Left Ventricular Outflow Tract Velocity Time Integral (LVOT VTI), Left Ventricular Outflow Tract Velocity (LVOT Velocity), Presystolic Wave Velocity (PSW Velocity), Presystolic Wave Velocity Time Integral (PSW VTI), Left Atrial Volume Index (LAVI), and Pulmonary Artery Pressure (PAP).
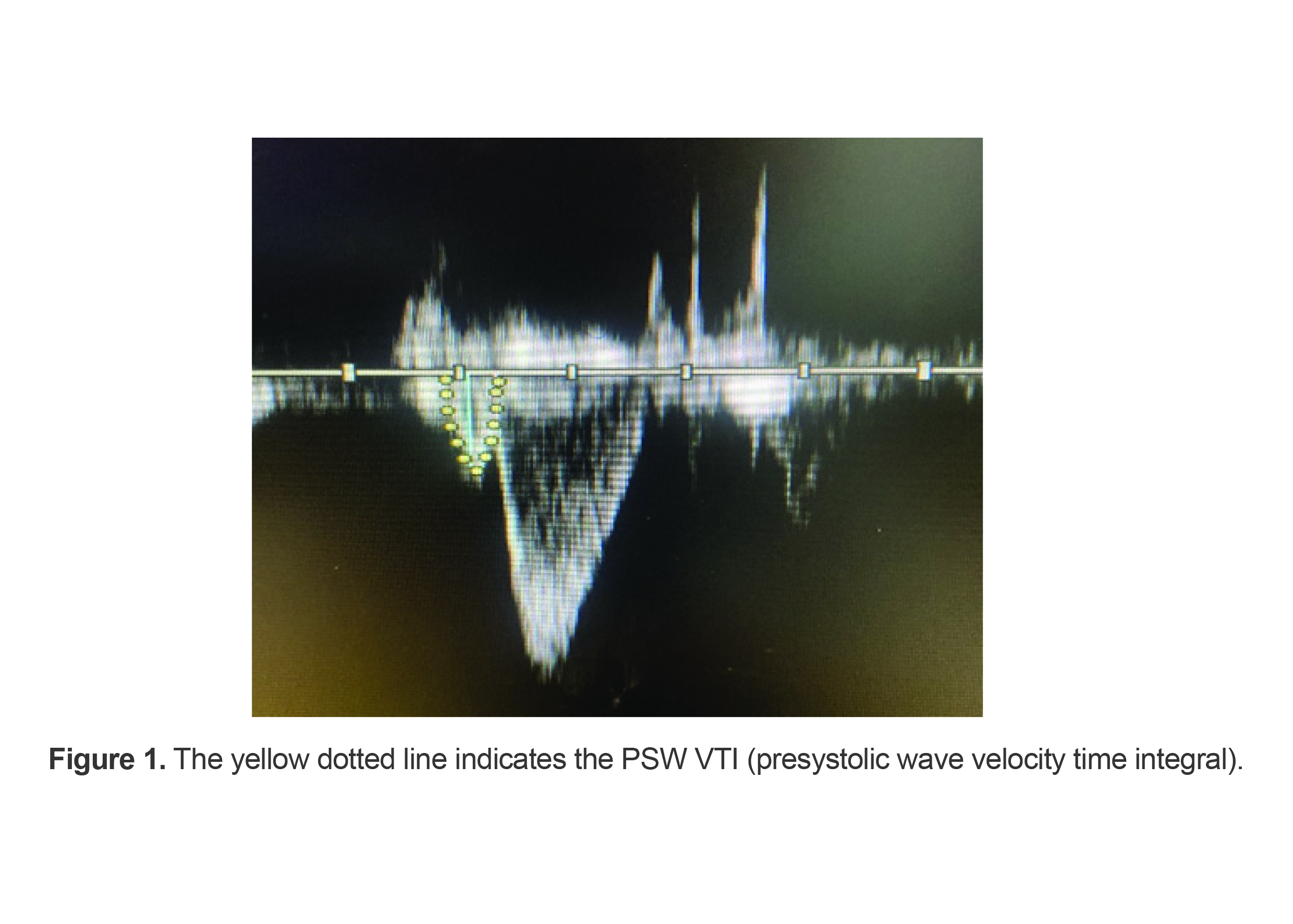
To assess the presence of PSW, a sample volume was placed in the LVOT just proximal to the aortic valve. Pulsed wave Doppler was used for examination through the apical five-chamber window, and the PSW peak velocity was recorded whenever a detectable PSW was observed (Figure 1).
Statistical analysis
Data description were presented as mean±standard deviation and frequency (percent). Normality was assessed by Kolmogorov-Smirnov test. The categorical variables were analyzed by Chi-Square or Fisher’s Exact test. Comparisons of the variables between CSF and CNF group, performed by the student’s t-test or Mann–Whitney U test.
Data analysis was performed by SPSS software (IBM Corp., Armonk, NY, USA, version 24). p-value less than 0.05 were considered as statistically significant.
Results
Sixty patients were included in the final analysis. The mean age of them in CSF and CNF group were 49.8±9.6 and 49.6±10.7 yrs, respectively. In CSF group 63.33% and in CNF group 43.33% of patients were female. No significant difference was found in terms of underlying diseases, smoking and BSA among studied groups (p>0.05) (Table 1).
As shown in table 2 and according to echordiographic characteristics, patients with CNF and CSF had statistically significant difference in terms of Em and aortic VTI (p<0.05), which they were lower in slow flow patients (Em: 8.5±3.0 vs. 8.0±3.0; p=0.049, aortic VTI: 26.7±5.4 vs. 23.8±4.9; p=0.032). The other echocardiographic indexes including MV E Velocity, A Velocity, AV annulus, LVOT VTI, LVOT Velocity, PSW Velocity, PSW VTI, LA Volume index and PAP did not have significant difference in the groups (p>0.05). Moreover, PSW velocity showed no significant difference between CNF and CSF groups (33.6±17.4 vs. 37.8±10.4, p=0.261), but it was slightly higher in patients with slow flow.
Table 1. Distribution of demographic characteristics of the patients in studied groups
|
Parameter |
|
Normal (N=30) |
Slow flow (N=30) |
p-value |
|
Age (yrs) |
|
49.6±10.7 |
49.8±9.6 |
0.920 a |
|
Sex |
Female |
13(43.33) |
19(63.33) |
0.059 |
|
Male |
17(56.66) |
11(36.66) |
|
|
|
BSA (m2) |
|
1.76±0.22 |
1.83±0.31 |
0.251 a |
|
Underlying diseases |
HTN |
6(20.0%) |
5(16.6%) |
0.732 b |
|
DLP |
9(30.0%) |
3(10.0%) |
0.053 b |
|
|
Smoking |
|
2(6.6%) |
0(0.0%) |
0.140 c |
BSA: Body Surface Area, DLP: Dyslipidemia, HTN: Hypertension.
Mean±Standard deviation, N (percent).
a Independent T-test, b Chi Square, c Fisher exact test.
Table 2. Echocardiographic characteristics of the patients in the two studied groups
|
Parameter |
Normal |
Slow flow |
p-value |
|
LVEF (%) |
60(1.25) |
60.0(0.0) |
0.005 a |
|
MV E Velocity (cm/sec) |
67.20±14.70 |
69.03±12.20 |
0.600 b |
|
A Velocity (cm/sec) |
65.40±13.30 |
61.50±13.08 |
0.261 b |
|
Em (cm/sec) |
8.50(3.0) |
8.00(3.0) |
0.049 a |
|
AV annulus (cm) |
1.90(0.3) |
2.00(0.1) |
0.210 a |
|
Aortic VTI (cm) |
26.70±5.40 |
23.80±4.90 |
0.032 b |
|
LVOT VTI (cm) |
17.43±3.30 |
18.14±2.90 |
0.370 b |
|
LVOT Velocity (cm/sec) |
89.60±15.17 |
91.90±16.94 |
0.571 b |
|
PSW Velocity (cm/sec) |
33.60±17.4 |
37.80±10.40 |
0.261 b |
|
PSW VTI (cm) |
2.95(3.6) |
3.40(1.1) |
0.170 a |
|
LAVI (cc/m2) |
22.0(11.25) |
20.0(7.45) |
0.550 a |
|
PAP (mmHg) |
20.0(12.25) |
20.0(0.0) |
0.862 a |
LVEF: Left Ventricular Ejection Fraction, MVE Velocity: Mitral Valve Flow E wave Velocity, A Velocity: Aorta Velocity, Em: Ventricular tissue doppler early diastolic velocity, AV annulus: Aortic valve annulus size, Aortic VTI: Aortic velocity time integral, LVOT VTI: Left ventricular outflow tract velocity time integral, LVOT Velocity: Left ventricular outflow tract velocity, PSW Velocity: Presystolic wave velocity, PSW VTI: Presystolic wave velocity time integral, LAVI: Left atrial volume index, PAP: Pulmonary artery pressure. a Mann-Whitney Test, b Independent T-test.
Discussion
This study aimed to evaluate PSW velocity in patients with CSFP compared to those with normal coronary arteries. The findings indicated differences in some echocardiographic parameters between patients with CSF and those with normal flow. Specifically, Em and aortic VTI were lower in patients with slow flow, but PSW velocity demonstrated no significant difference between the groups. PSW is typically observed during the late diastolic phase when using Doppler ultrasound to examine the left ventricular outflow tract (10) and may predict increased arterial stiffness (11).
Dursun et al found that the presence of PSW was associated with higher LVEF and lower stages of diastolic dysfunction in patients with acute myocardial infarction (16). Another study suggested that PSW could be useful for risk stratification in hypertensive patients (10). Additionally, PSW is commonly observed in the LVOT (17) and it has been linked to aortic stiffness, as indicated by reduced aortic distensibility, and may serve as an independent predictor of aortic stiffness (18). Increased arterial stiffness can lead to systolic hypertension, left ventricular hypertrophy, and impaired coronary perfusion, thereby increasing cardiovascular risk (19).
PSW is a parameter that reflects the late diastolic period during Doppler evaluation of the left ventricular outflow tract, although its mechanism is not fully understood., PSW is a parameter that reflects the late diastolic period during Doppler evaluation of the left ventricular outflow tract. Although its mechanism is not fully understood (17). Mohammadzad et al found that LVEF and E wave were significantly lower in the CSFP group compared to the control group (20), which contrasts with the findings of the current study.
Recent studies have shown that patients with CSFP often have metabolic syndrome, high cholesterol, high fasting glucose, and high body mass index (21). However, in the present study, there was no difference in terms of HTN, DLP and BSA in the CSF group between the CSFP group and the control group. Various studies have examined the echocardiographic, clinical, and angiographic findings and risk factors of CSFP patients (22,23). The findings revealed no significant difference in smoking status, HTN, and DLP between patients with slow flow and those with normal coronary arteries. Another study found that smoking and HTN were significantly higher in the CSFP group, while no intergroup difference was found in DLP (20), which aligns with our findings. Additionally, some studies found no relation between CSFP, HTN, and DLP (24,25).
Dutta et al demonstrated that CSF refers to patients who exhibit reduced coronary flow velocity and elevated microvascular resistance at rest, but it has poor sensitivity and specificity for detecting coronary microvascular dysfunction (26). This study has some limitations, including being a single-center study with a limited sample size. Furthermore, there are few studies evaluating PSW velocity in echocardiography of CSF patients, limiting our ability to compare the findings with other studies.
Conclusion
In conclusion, this study found no difference in PSW velocity between patients with slow coronary flow and those with normal coronary flow, and it is not associated with arterial stiffness. Therefore, PSW velocity cannot be used as a predictor of arterial stiffness in CSF patients. Further research is recommended to validate or refute these findings.
Ethical statement
Ethical approval code was received from Mashhad University of Medical Sciences (code: IR.MUMS.MEDICAL.REC.1401.346). This study was conducted in accordance with the Declaration of Helsinki.
Funding
No fund was received for this study.
Acknowledgement
We thank all the participants who were investigated in the study and the colleagues in Ghaem Hospital, Mashhad, Iran. We express our especial thanks to ethics committee of Mashhad University of Medical Sciences.
Conflict of Interest
There was no conflict of interest in this manuscript.