Document Type : Original article
Abstract
Background: This study was conducted to investigate the efficacy of home-based versus center-based cardiac rehabilitation on the risk factors for cardiovascular disease, quality of life and adherence to treatment.
Methods: Sixty-five patients were randomly assigned into the home-based group or the clinic-based group. A 3-month rehabilitation course was designed for patient in each session based on the AACVPR guidelines. Cardiac biomarkers, quality of life (using the SF-36 questionnaire), and treatment adherence (through a questionnaire) were evaluated at the beginning and end of the study for each patient. In both groups, data were compared before and after the rehabilitation, and the data between the two groups were also compared.
Results: In this study, the home group achieved significantly higher scores in three aspects of treatment adherence compared to the clinic group (p<0.01). The clinic group scored significantly higher in the social functioning domain of the quality-of-life measure compared to the home group (p=0.03). Additionally, the clinic group exhibited a lower average serum cholesterol level than the home group after rehabilitation (p=0.001).
Conclusion: Although the clinic group demonstrated better results in some quality-of-life domains and lower serum cholesterol post-rehabilitation, the home-based rehabilitation may offer benefits in terms of treatment adherence. Therefore, it seems that home-based rehabilitation can be considered a viable alternative for patients unable to attend center-based programs, particularly for those who prioritize convenience and adherence, but further research is needed to explore its impact on cardiovascular risk factors like blood pressure.
Keywords: Cardiovascular disease, Home rehabilitation, Hospital rehabilitation, Quality of life, Treatment adherence
Introduction
Heart diseases are the most common cause of death in many countries, including Iran (1). Additionally, the majority of mortality from non-communicable diseases worldwide is attributed to cardiovascular diseases. Based on strong evidence highlighting the prominent role of high blood pressure, hyperlipidemia, diabetes, and smoking in the pathogenesis of coronary heart disease, these factors are recognized as common risk factors (2,3). A suitable and rational approach to manage these patients primarily involves controlling modifiable risk factors to prevent the progression of the disease and the occurrence of serious cardiac events, such as angina, myocardial infarction, congestive heart failure, and death.
Preventing complications associated with cardiovascular diseases and ensuring successful treatment are essential. This necessitates implementing preventive and therapeutic measures, such as engaging in regular physical activity, adhering to a proper diet, and consistently using relevant medications. One of the primary concerns and clinical challenges for healthcare professionals is related to patients’ non-adherence to the prescribed treatment regimen. Treatment adherence becomes particularly crucial in chronic diseases, including heart disease, where individuals must adhere to the prescribed treatment for an extended period. Furthermore, reducing the length of hospital stays provides fewer opportunities to offer information to patients and address their concerns. Therefore, post-discharge follow-up for self-care becomes imperative (4).
Today, one of the important methods that can significantly improve the quality of life for patients is rehabilitation programs. Cardiac rehabilitation contributes to reducing anxiety, depression, angina, ischemia, hospital readmission, and mortality while enhancing the overall quality of life for cardiac patients (5). Although rehabilitation programs are predominantly conducted in hospitals and offer numerous benefits, they also come with drawbacks (5, 6). These challenges include issues related to patient transportation, the recurrence of pains experienced during hospitalization, and the substantial costs associated with hospital-based rehabilitation. In recent years, home-based cardiac rehabilitation has been regarded as a promising strategy to overcome obstacles that impede patient participation in cardiac rehabilitation programs in hospitals. These obstacles include time constraints, transportation issues, and patients’ hesitancy to join rehabilitation groups in healthcare centers. Moreover, home-based rehabilitation fosters an enhanced willingness among participants to engage in rehabilitation programs (5,6).
Considering the points mentioned and recognizing the few studies exploring the impact of home-based cardiac rehabilitation on the quality of life, risk factors, and treatment adherence among cardiac patients, and noting the absence of comprehensive studies in this regard in Yazd province, this research aims to compare the efficacy of home-based vs. center-based cardiac rehabilitation on the risk factors for cardiovascular disease, quality of life, and adherence to treatment.
Materials and Methods
Sample selection
This randomized clinical trial study was conducted on cardiac patients referred to Afshar Hospital in 2019. Sampling was done using the convenience sampling method. Considering a meaningful level of 5%, a test power of 80%, and based on a previous similar study (7) and the standard deviation of the SF36 quality of life dimensions, to achieve a significant reduction of at least 15 points in the quality-of-life dimensions, especially the physical aspect, a sample size of 28 individuals was required. Considering a 10% dropout rate, each group required a total of 31 individuals.
Inclusion and exclusion criteria
Inclusion criteria were as follows: ejection fraction greater than 40%, clinical stability (including the absence of unstable angina, heart failure, and conditions restricting exercise such as fluid accumulation diseases in the lungs, respiratory diseases, or infectious diseases), no active or severe arrhythmias (including ventricular arrhythmias or atrial fibrillation) that would interfere with exercise or rehabilitation, normal response to exercise testing, and age between 30 and 75 years.
Exclusion criteria included uncontrolled diabetes and blood pressure, systemic and respiratory diseases restricting exercise, physical disabilities or any exercise-limiting conditions, severe valvular heart diseases, known or suspected aortic dissection, patient dissatisfaction, non-cooperation during the rehabilitation program, patient death, and lack of favorable physical conditions for continuing the rehabilitation program.
Procedure
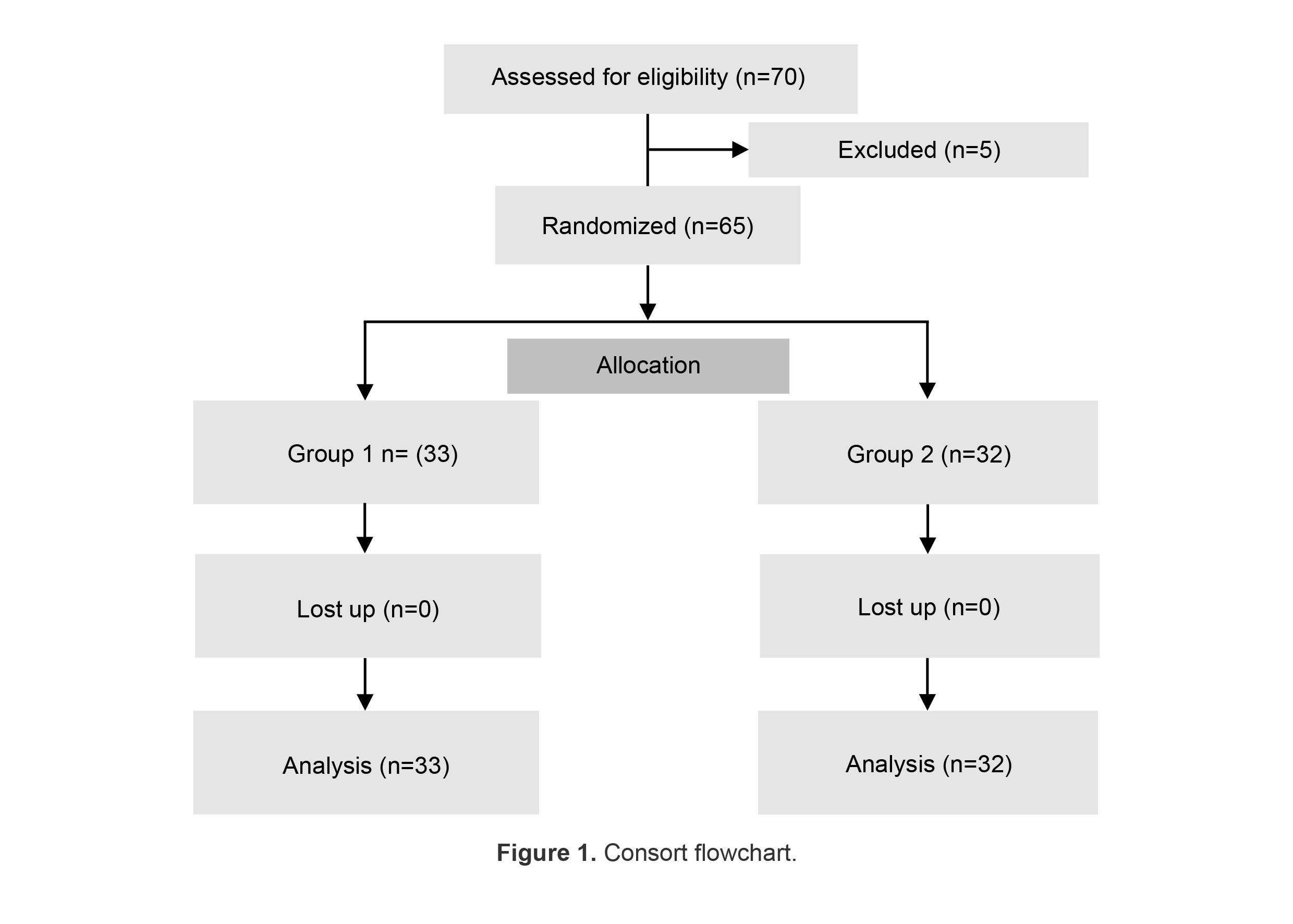
This study was conducted on 65 patients with heart problems, requiring rehabilitation. The purpose and process of the study were explained to the patients, and after obtaining the informed consent and confirming the inclusion criteria, they were enrolled in the research. Patients were randomly divided into two groups: 33 in the first intervention group (receiving rehabilitation interventions at the clinic) and 32 in the second intervention group (receiving rehabilitation interventions at home).
A random allocation method was used to assign the participants to the two groups. The randomization was performed using random number table. This process was conducted to ensure that each participant had an equal chance of being assigned to any of the groups, thereby minimizing selection bias.
Initially, all the patients underwent the examination and evaluation. The demographic characteristics, including age, gender, history of hypertension, history of diabetes, high blood lipid levels, family history of heart disease, and clinical information such as the type of heart disease, blood pressure, heart rate, and paraclinical information (e.g., fasting plasma glucose, lipid profile, exercise test results, and quality of life), were recorded in both groups. Exercise tolerance testing was used to assess the functional capacity, determine the maximum heart rate, and evaluate cardiovascular status, serving as a baseline for determining the duration and intensity of exercises at the end of the period.
In both groups, clinical data (height, weight, systolic/diastolic blood pressure, and heart rate) and paraclinical results (triglycerides, cholesterol, and fasting blood sugar) were collected and recorded at the beginning and end of the 12 weeks.
Patients who visited the outpatient rehabilitation center within the specified time frame (1 week after Percutaneous Coronary Intervention (PCI) and or Myocardial Infarction (MI) with PCI, 3 weeks after Coronary Artery Bypass Grafting (CABG) and/or heart valve surgery, and 1 month after MI without PCI) underwent further evaluations to complete the training. The history of previous illnesses, assessment of the patient’s cardiovascular risk factors, smoking, drug and alcohol use, the patient’s level of activity before the cardiac event, and the post-discharge phase were evaluated. Echocardiography and exercise testing (if indicated and at the discretion of the treating physician) were performed. Based on the above evaluations, each patient was risk-stratified according to AACVPR guidelines for receiving rehabilitation interventions (8).
Implementation of the rehabilitation program
The rehabilitation program generally consisted of a 12-week duration, with three sessions of aerobic exercise per week, lasting 50 min each, including 10 min of warming up, 30 min of aerobic movements, and 10 min to cool down. Participants in the intervention group received structured exercise rehabilitation program and patient’s physical activity was recorded on a specific chart throughout the exercise time.
Participants in the control group were instructed to continue their usual daily activities.
Phone calls were conducted on a regular basis to assess progress, address any concerns or difficulties encountered by the patients, and provide support as needed. Additionally, the patients were encouraged to report any adverse symptoms or challenges, and these were addressed by healthcare professionals overseeing the program.
Therefore, the monitoring system was aligned with the goals of the rehabilitation program, focusing on ensuring adherence to treatment, assessing patient progress, and maintaining communication for ongoing support and guidance. Further, patient compliance with exercise and lifestyle changes was assessed using questionnaire, which helped quantify treatment adherence at the beginning and end of the study.
In addition, parameters such as blood pressure, and patient symptoms were regularly monitored through regular phone calls. The monitoring was designed to ensure that the patients were adhering to the prescribed rehabilitation protocol, including exercise regimens, dietary guidelines, and other lifestyle modifications recommended by the rehabilitation program.
In addition, for patients with diabetes, blood glucose was assessed at the beginning and recorded on the chart. If any contraindications were present, the patient was referred to the treating physician for further evaluation based on AACVPR guidelines.
The patient’s physical activity started with a warm-up, conducted by a physiotherapist. The main phase of activity occurred in the main cardiac rehabilitation space, with the presence of nurses, physiotherapists, and the resident physician. The daily activity for the patient was planned based on the patient’s previous session’s activity level, considering the maximum heart rate determined for each patient, and the patient’s understanding of their previous physical activity based on the Borg scale. If there was an increase beyond the specified maximum heart rate, the patient’s understanding of physical activity reached level 13, abnormal changes in the ECG, positive Talk test symptoms, or contraindications based on AACVPR guidelines, the patient’s activity would be reduced or discontinued.
Training
The educational sessions included instruction on nutrition, lifestyle modification, medication management, weight reduction, engaging in daily activities, and avoiding strenuous activities that may lead to fatigue and shortness of breath. Training on how to regularly control vital signs, including pulse and blood pressure, avoiding extreme cold and heat, maintaining a proper diet, limiting salt, alcohol, and fat intake, emphasizing the consumption of fresh vegetables and fruits, promoting fiber and whole grains intake, quitting smoking and alcohol, as well as educating on sexual activities and stress management techniques, were among the topics taught to the participants. In the intervention group (at home), weekly telephone communication with patients was conducted to assess the duration of heart rate activity during exercise and evaluate symptoms during activity using Borg criteria. Exercise testing and echocardiography for patients in the home group were performed at the center.
Questionnaire on patients’ treatment
Adherence: The level of patients’ adherence to treatment was assessed using a questionnaire designed by Modanloo in 2013 (9). This questionnaire consisted of 40 questions covering areas such as interest in treatment, willingness to participate in treatment, adaptability, integration of treatment with life, attachment to treatment, commitment to treatment, and management in the implementation of treatment. The initial scores are converted to a scale of zero to one hundred, with a score of 75-100 indicating very good adherence to treatment, 50-74 indicating good adherence to treatment, 26-49 indicating average adherence, and 0-25 indicating poor adherence to treatment. The validity and reliability of the Persian version of this questionnaire have also been determined.
Quality of life questionnaire
The SF36 quality of life questionnaire was used to assess the quality of life of the study participants. This questionnaire was designed in the United States in 1992, and its validity and reliability have been examined in various patient groups (10). The questionnaire evaluates the quality of life of patients in different physical and mental dimensions, obtained by combining scores from the eight health domains.
The questionnaire comprises 36 items covering eight health domains. The lowest score on this questionnaire was 0, and the highest score was 100. The score for each dimension was determined by the scores assigned to the items in that dimension. The reliability and validity of the Persian version of this questionnaire were confirmed in Iran. Both questionnaires were completed at two separate time points (the beginning and the end of the study) for both groups.
Statistical analysis
Data were entered into SPSS version 25 (IBM Crop., Armonk, NY, USA). For data with normal distribution, mean±SD, and for non-normal data, median (IQR) were used. Moreover, data were analyzed using Paired t-test, independent t-test, Mann-Whitney U test and Wilcoxon singed-rank. P<0.05 was assumed significant. In addition, Univariate Analysis of Variance (ANCOVA) was used for comparison cardiovascular disease risk factors and dimensions of adherence to treatment after intervention.
Results
In the current study, the mean age of the patients in clinic and house groups was 60.3±7.37, and 58.72±8.40 years, respectively (p=0.506). The mean BMI in clinic and house groups before intervention was 27.30±3.70 and 27.73±4.38, respectively. After the intervention, the mean BMI in the clinic group was 27.12±3.76, while in the home group, it was 27.46±4.41 (p=0.593). In terms of gender, 8.75% of the treated patients in the clinic and 6.65% at home were male, with the remaining individuals being female (p=0.360).
Regarding the underlying diseases, 2.24% and 1.53% of the patients in the clinic and at home had diabetes, respectively. Additionally, 3.33% and 3.56% of the patients in the clinic and at home experienced dyslipidemia (p=0.593). Furthermore, 3.30% and 6.65% of the individuals undergoing treatment in the clinic and at home had hypertension, respectively (p=0.004). Smoking before rehabilitation was observed in 0 patients in group 1 and 6 patients in group 2 (p=0.011).
In the house care group, following rehabilitation, one person reported quitting smoking, and three reported a reduction in smoking. The remaining two showed no change in their smoking habits.
The comparison of cardiovascular disease risk factors in the clinic and house before and after intervention is shown in table 1. As shown in table 1, a significant difference was observed before and after intervention regarding the mean levels of cholesterol in clinic group (group 1) (p<0.05). Furthermore, there was a significant difference before and after intervention in terms of FBS, diastolic blood pressure, and triglyceride in home group (group 2) (p<0.05). When comparing the above factors between the clinic and house care groups using Univariate Analysis of Variance regarding triglyceride, a significant difference was found between the two groups, and it seems that rehabilitation at home had a significant effect on reducing the triglyceride levels of the patients.
In addition, the results of the Univariate Analysis of Variance (ANOVA) reveal that the factors “before SBP” (before systolic blood pressure) and “before Smoke” (before smoking status) significantly influence “after SBP” (after systolic blood pressure), with p-values of less than 0.001 and 0.008, respectively. However, the variable “group” (clinic vs. home) showed no significant effect on after SBP (p=0.389), suggesting that the location of the intervention did not impact the outcome. The overall model was significant (p<0.001) with an R-squared value of 0.549, indicating that nearly 55% of the variance in after SBP can be explained by the predictors included in the model. Thus, while the intervention setting (clinic vs. home) did not affect after SBP, prior blood pressure and smoking status were important determinants.
The Univariate Analysis of Variance (ANOVA) indicates that “before Smoke” (before smoking status) and “before Diastolic Blood Pressure “ (before DBP) significantly affect “after DBP”. Specifically, “before Smoke” [F (1,61)=15.857, p<0.001] and “before DBP” [F(1,61)=69.591, p<0.001] were both found to be significant predictors of after DBP. However, the variable “group” (clinic vs. home) indicated no significant effect [F (1,61)=1.323, p=0.255], suggesting that the setting of the intervention does not significantly influence the after DBP outcome. The model was overall significant [F (3,61)=25.576, p<0.001[, with an R-squared value of 0.557, meaning that approximately 55.7% of the variation in after DBP is explained by the included factors. Thus, while the intervention group had no significant effect, prior blood pressure levels and smoking status were key determinants of the diastolic blood pressure outcome.
The comparison of dimensions of adherence to treatment in patients in each of the two groups, clinic and home is shown in table 2. As shown in table 2, a significant difference was observed before and after intervention in group 1 (clinic group) in terms of interest in treatment, ability to adapt, and commitment to treatment (p<0.05).
In addition, a significant difference was observed before and after intervention in group 2 (house group) in terms of all dimensions of adherence to treatment (p<0.05). In the house care group, dimensions of treatment adherence, including interest in treatment, adherence to treatment, and commitment to treatment showed higher score compared before intervention. Moreover, comparison of the two groups after intervention using Univariate Analysis of Variance demonstrated that these parameters improved in house group than the clinic group.
The comparison of variables of quality of life before and after intervention in the two groups is shown in table 3. As shown in table 3, there was a significant difference before and after the intervention in group 1 regarding all variables of quality of life (p<0.05), except for role emotional health and pain. Additionally, a significant difference was observed before and after the intervention in group 2 in terms of all parameters of quality of life (p<0.05), except for bodily pain.
The comparison of the two groups regarding the quality-of-life parameters is shown in table 4.
As shown in table 4, a significant difference was observed between the two groups in terms of social functioning (p<0.05).
Table 1. The comparison of cardiovascular disease risk factors in clinic and house
|
p-value*** |
After rehabilitation |
Before rehabilitation |
Variables |
Clinic/House |
|
0.47 |
122.36±37.3 |
138.94±47.99 |
Triglyceride |
Clinic (group 1) |
|
0.045 |
139.94±35.19 |
143.91±39.70 |
Triglyceride |
House (group 2) |
|
- |
0.056 0.033 |
0.651 |
p-value* p-value** |
|
|
<0.001 |
125.55±23.25 |
156.24±35.063 |
Cholesterol |
Clinic (group 1) |
|
0.9 |
156.91±40.246 |
156.53±36.17 |
Cholesterol |
House (group 2) |
|
- |
<0.001 0.000 |
0.974 |
p-value* p-value** |
|
|
0.51 |
111.67±25.33 |
114.79±22.91 |
Fast blood sugar (FBS) |
Clinic (group 1) |
|
0.001 |
120.91±45.28 |
130.28±51.85 |
Fast blood sugar (FBS) |
House (group 2) |
|
- |
0.312 0.612 |
0.122 |
p-value* p-value** |
|
|
0.32 |
115.55±9.220 |
117.30±10.18 |
Systolic blood pressure |
Clinic group |
|
0.168 |
123.16±22.05 |
126.78±21.08 |
Systolic blood pressure |
House group |
|
- |
0.830 0.832 |
0.024 |
p-value* p-value** |
|
|
0.47 |
72.21±8.26 |
73.24±9.73 |
Diastolic blood pressure |
Clinic group |
|
<0.001 |
75.88±8.46 |
79.53±9.16 |
Diastolic blood pressure |
House group |
|
- |
0.770 0.770 |
0.008 |
p-value* p-value** |
|
|
0.43 |
73.48±4.59 |
74.45±6.91 |
Heart rate |
Clinic group |
|
0.242 |
75.31±7.11 |
73.69±8.75 |
Heart rate |
House group |
|
- |
0.226 0.118 |
0.696 - |
p-value* p-value** |
* Independent T-test.
**Univariate Analysis of Variance.
***Paired sample t-test
Table 2. Dimensions of adherence to treatment in patients in each of the two groups, clinic and house
|
Clinic house |
Dimensions of adherence to treatment |
Before rehabilitation |
After rehabilitation |
p-value*** |
||
|
Before median |
Interquartile range (IQR) |
After median |
Interquartile range |
|||
|
|
Willingness to participate in treatment |
25.7 34.2 |
(21.4) (11.4) |
22.8 28.6 |
(15.7) (13.6) |
0.123 0.042 |
|
p-value* p-value** |
0.13 - |
0.347 0.981 |
- |
|||
|
Clinic house |
Interest in treatment |
31.1 31.1 |
(30) (15) |
24.4 40 |
(22.2) (12.8) |
0.002 0.001 |
|
p-value* p-value** |
0.751 - |
0.008 0.000 |
- |
|||
|
Clinic house |
Ability to adapt |
31.4 92.4 |
(22.9) (19.3) |
28.6 37.1 |
(17.1) (17.1) |
0.021 0.001 |
|
p-value* p-value** |
0.563 - |
0.004 0.000 |
- |
|||
|
Clinic house |
Integration of treatment with life |
32 32 |
(8) (16) |
32 7 |
(8) (23) |
0.801 <0.001 |
|
p-value* p-value** |
0.894 - |
<0.001 0.000 |
- |
|||
|
Clinic house |
Adherence to treatment |
32 27.5 |
(22.5) (15) |
25 60 |
(25) (10) |
0.345 <0.001 |
|
p-value* p-value** |
0.752 - |
<0.001 0.000 |
- |
|||
|
Clinic house |
Commitment to treatment |
80 34 |
(18) (12) |
84 84 |
(10) (19) |
0.007 <0.001 |
|
p-value* p-value** |
0.000 - |
0.131 0.000 |
- |
|||
|
Clinic house |
Measures in the implementation of treatment |
86.7 33.3 |
(13.3) (13.3) |
93.3 86.7 |
(20) (13.3) |
0.146 <0.001 |
|
p-value* p-value** |
0.000 - |
0.768 0.424 |
- |
|||
* Mann-Whitney U test.
**Univariate Analysis of Variance.
***Wilcoxon singed-rank test
Table 3. Comparison of variables of quality of life before and after intervention
|
p-value |
After rehabilitation |
Before rehabilitation |
Variables of quality of life |
|
|
<0.001 |
88.94±8.174 |
65.61±23.77 |
Physical functioning |
Clinic (group 1) |
|
0.003 |
79.55±26.84 |
62.88±41.51 |
Role-physical health |
|
|
0.084* |
100±0 |
100±34 |
Role-emotional health* |
|
|
0.002 |
85.64±11.53 |
78.94±16.75 |
Vitality |
|
|
0.002 |
91.27±10.66 |
83.55±17.82 |
Mental health |
|
|
0.001 |
93.77±10.520 |
84.55±19.07 |
Social functioning |
|
|
0.84 |
96..97±17.40 |
97.42±9.196 |
Bodily pain |
|
|
0.001* |
95±8 |
90±20 |
General health* |
|
|
0.001 |
88.28±12.35 |
72.66±24.49 |
Physical functioning |
House (group 2) |
|
0.001 |
71.09±18.83 |
53.13±25.98 |
Role physical health |
|
|
0.001 |
100±34 |
100±67 |
Role emotional health |
|
|
0.001 |
85.63±14.35 |
71.88±28.39 |
Vitality |
|
|
0.002 |
87.34±16.43 |
78.88±24.93 |
Mental health |
|
|
<0.001* |
87.69±11.73 |
76.50±21.60 |
Social functioning |
|
|
0.16 |
98.91±6.18 |
97.50±9.41 |
Bodily pain |
|
|
<0.001* |
90±15 |
75±24 |
General health* |
Table 4. The comparison of the two groups regarding quality-of-life parameters
|
p-value |
Rehabilitation house (group 2) |
Rehabilitation clinic (group 1) |
Parameters of quality of life |
|
0.80 |
88.28±12.35 |
88.94±8.17 |
Physical functioning |
|
0.14 |
71.09±18.08 |
79.55±26.84 |
Role-physical health |
|
0.13 |
100±34 |
100±0 |
Role- emotional health* |
|
0.225 |
85.63±14.35 |
85.64±11.5 |
Vitality |
|
0.256 |
87.34±16.43 |
91.27±10.660 |
Mental health |
|
0.031 |
87.69±11.73 |
93.79±10.5 |
Social functioning |
|
0.555 |
98.91±6.187 |
96.97±17.40 |
Bodily pain |
|
0.08 |
60±15 |
95±8 |
General health* |
Discussion
So far, conflicting results have been obtained regarding the effectiveness of cardiac rehabilitation at home compared to the hospital (standard rehabilitation center environment). The present study represented that cardiac rehabilitation at home was not less effective than rehabilitation in the clinic in some cases. Both groups of the patients demonstrated promising results regarding the improvement of the considered indicators during the study. The main difference between the two groups was in areas related to treatment adherence, primarily observed in the group of patients receiving home care. However, the clinic patients were more successful in controlling risk factors and improving the quality of life, especially in the area of social functioning, than the patients receiving home care. Iranian studies with similar subjects indicated results consistent with the findings of the present study. In a clinical trial, Limoui et al reported that volunteers who received rehabilitation services at home had a significantly higher quality of life score compared to the control group (hospital) (11). Similarly, Salvati et al, obtained comparable results in another center (12). Both recent studies utilized the MacNew questionnaire to assess the quality of life, which evaluates well-being in three areas: emotional, physical, and social. It is worth noting that the questionnaire employed in this study also covers these aspects, making its results directly comparable with those of the aforementioned studies.
Aronov et al compared the effectiveness of cardiac rehabilitation alone at home and the combination of rehabilitation at the treatment center and home. They followed up with the patients for 12 months, examining functional and clinical parameters (13). Functional tests, including the exercise tolerance test, revealed more promising results in the group of patients who received coordinated care both at the treatment center and at home. Another unexpected finding was the increased level of cardiovascular disease risk factors, including blood lipid levels, in the group that received rehabilitation measures at home.
In contrast to the present study, none of the risk factors in either the clinic or home-based groups exhibited an increasing trend at the beginning and end of rehabilitation. While this study had the advantage of a longer follow-up period, the smaller number of volunteers (18 people in each group) may account for the differences in results. Additionally, the present study examined treatment adherence, highlighting it as one of its focuses or advantages.
Snoek et al, in a large clinical trial involving 179 patients across five European countries, investigated the impact of cardiac rehabilitation at home using telemonitoring (via mobile phone). The study revealed positive results concerning increased functional capacity and VO2 peak levels during the one-year follow-up period. Additionally, improvement was seen in clinical indicators such as systolic and diastolic blood pressure in the intervention group. Notably, the group receiving the intervention demonstrated a decrease in glycosylated hemoglobin levels, while no changes were observed in other cardiovascular biochemical risk factors such as triglycerides and cholesterol during the one-year follow-up (14). Comparatively, in contrast to the present study, the group of patients receiving rehabilitation services at home exhibited a similar trend of changes, with the distinction that triglycerides were significantly reduced in this patient group.
One aspect of the current study focuses on patients’ adherence to treatment, which yielded significant results both in the clinic patient group and the group of patients receiving rehabilitation measures at home.
Pashchaman et al investigated treatment adherence in patients following coronary heart bypass surgery (15). They utilized Modanloo’s questionnaire (16) to measure patient adherence, making it a suitable basis for comparison with the present study. Comparing centrality indices between the two studies indicates the positive and effective performance of rehabilitation measures at home.
A notable point in the study was the level of treatment adherence in the group receiving rehabilitation measures in the clinic. Approximately 20% of the individuals referred to rehabilitation clinics refuse to do even one session of rehabilitation measures (6,17,18). This refusal may stem from commuting difficulties, reduced activity in old age, or a lack of sufficient motivation to continue treatment and rehabilitation. In alignment with the results of Snoek et al’s study, cardiac rehabilitation at home appears to be a suitable option for this particular group of patients.
In the present study, there was no significant difference between the two groups in terms of the quality of life. However, the group undergoing rehabilitation in the clinic had a superiority in social aspects compared to the home-based group. This finding aligned with other studies confirming the effectiveness of face-to-face interactions and patient communication compared to remote monitoring through phone assistance in motivating patients (19).
Overall, this study suggests that recommending home-based rehabilitation interventions can be a suitable or even optimal option for cardiovascular patients who, for any reason, are not inclined to participate in rehabilitation sessions at a center. This approach demonstrates positive effects similar to those observed in center-based rehabilitation. However, for the optimal enhancement of all aspects of rehabilitation, hybrid options that combine both home-based and center-based approaches can also be proposed to patients.
Strengths and limitations of the study
This study represented the first simultaneous investigation of the quality of life, treatment adherence, and risk factors associated with the occurrence of heart diseases in patients eligible for cardiac rehabilitation. However, it was important to acknowledge the limitations of this study. It should be noted that increasing the duration of patient follow-up could yield more reliable results.
Considering that the majority of rehabilitation studies had been conducted internationally, it was essential to conduct investigations tailored to the unique conditions and facilities of each country. This included an assessment of the cost and economic efficiency associated with home-based rehabilitation vs. clinic-based rehabilitation, aspects not addressed in the current study, which could serve as a foundation for future research.
Recognizing the distinctive life circumstances of each patient, it becomes possible to tailor rehabilitation interventions uniquely to different patient groups, taking into account factors such as livelihood status, literacy level, place of residence, and more to provide more comprehensive services and achieve improved results.
Conclusion
According to these findings, although the clinic group demonstrated better results in some quality-of-life domains and lower serum cholesterol post-rehabilitation, the home-based rehabilitation may offer benefits in terms of treatment adherence. Therefore, it seems that home-based rehabilitation can be considered a viable alternative for patients unable to attend center-based programs, particularly for those who prioritize convenience and adherence. In addition, these findings suggest that prior blood pressure levels and smoking status are key factors in determining blood pressure outcomes, while the location of rehabilitation does not significantly affect these results.
Ethical considerations
This study was approved by Ethics Committee of Shahid Sadoughi University of Medical Sciences (IR.SSU.MEDICINE.REC.1399.093). Additionally, it was approved by Iranian registry clinical trial (IRCT20210927052610N1).
Acknowledgement
The authors highly appreciate the assistance of participants in completing the questionnaires and responding to the inquiries presented in the thesis.
Conflict of Interest
There was no conflict of interest in this manuscript.