Document Type : Original article
Abstract
Background: Bipolar Disorder (BD) is a fairly common serious mental illness. A definitive and reliable biomarker remains elusive despite extensive exploration of various serum markers, brain scans, and genetic variants for diagnostic utility in BD. Reports indicate that serum uric acid levels are elevated in BD. This study aimed to determine whether salivary uric acid levels, as a non-invasive method, change in the same way as serum levels in these individuals.
Methods: In a cross-sectional study, 28 patients aged 18 to 65 with BD based on DSM-5 diagnostic criteria were referred to teaching hospitals of Aja University of Medical Sciences in Tehran, and a control group consisting of 28 healthy individuals of the same gender and age entered the study. The serum and salivary uric acid levels were measured photometrically, and the data were analyzed by Unpaired Student’s t-test using SPSS software.
Results: The mean concentration of serum and unstimulated saliva uric acid was significantly higher in patients than in healthy individuals, and the cut-off point for serum was 6.4 mg/dL with a sensitivity of 79% and a specificity of 68%, and for saliva, it was 3.3 mg/dL with 65% sensitivity and 61% specificity
Conclusion: It seems that the amount of salivary uric acid increases in patients with BD, which may be used as an auxiliary biomarker for monitoring and diagnosis of the disease.
Keywords: Bipolar disorder, Serum, Saliva, Uric acid
Introduction
Bipolar Disorder (BD) is a fairly common serious mental illness, is a chronic and recurring condition characterized by fluctuations in mood and energy levels (1), and influences nearly 2% of the world’s population (2). It typically begins during adolescence or early adulthood (3), leading to cognitive impairment and mental symptoms that disrupt social functioning (4). Despite effective treatments being available, there is often a significant delay of approximately 6 years between the onset of BD and its diagnosis and management (5). Early diagnosis is challenging, since the initial episode of BD may present similarly to unipolar depression (6,7), leading to misdiagnosis and inappropriate treatment with antidepressants without mood stabilizers, increasing the risk of mood swings to hypomania or mania while failing to prevent new depressive episodes (8).
Biomarkers hold significant potential for detection, management of the condition, assessment of treatment efficacy, and advancement of therapeutic approaches in BD. Despite extensive exploration of various serum markers such as increasing magnesium (9), uric acid (10,11), decreasing osmolarity (12), brain scans, and genetic variants for diagnostic utility in BD, a definitive and reliable biomarker remains elusive (13).
The purinergic system represents a crucial biological axis in mood disorders (14). Dysfunction within this system may contribute to the pathophysiology of mood and other psychiatric disorders (15), impacting the activity of multiple neurotransmitters including dopamine, gamma-aminobutyric acid, glutamate, and serotonin (16). Notably, the purinergic system can modulate various behaviors frequently affected in individuals with BD such as sleep patterns, motor activity, aggressive behavior, and social interaction (17).
Uric acid is the final product of purine metabolism, primarily synthesized by xanthine dehydrogenase in the liver and excreted through the kidneys in urine. Elevated uric acid levels are linked to heightened purinergic conversion and reduced adenosinergic transmission (18,19). As a result, it is postulated that individuals with BD may exhibit purinergic dysfunction characterized by elevated uric acid levels compared to healthy individuals and those with other mental disorders (2,18,20). Adenosinergic receptors regulate cellular excitability by suppressing neurotransmitter release in the central nervous system (21).
Studies linking serum uric acid levels to BD show that serum uric acid levels are associated with impulsivity, psychomotor agitation, agitated mood, and hyperthymic mood. In contrast, serum uric acid levels were associated with depressed mood independent of the disorder stage, suggesting that serum uric acid can be a useful biomarker for differentiating BD from major depressive disorder (22,23). Increased uric acid levels have been associated with impulsivity, impulsive behavior, irritability, hyperthymic mood, and severe manic symptoms (24,25).
Therefore, in recent years, efforts have been made to replace blood tests with other samples of biological materials that non-invasive methods can collect. Saliva has been proposed as a potential diagnostic tool for disease monitoring due to its multiple advantages. This provides an inexpensive, simple, and easy-to-use screening method (21-23). On the other hand, diseases such as BD may affect the salivary glands, and since saliva and its composition are important in oral and dental hygiene, speech and even breathing, any change in its composition will be important. Since reports indicate that serum uric acid levels are elevated in individuals with BD, this study aimed to determine whether salivary uric acid levels in these individuals change in the same way as serum levels.
Materials and Methods
In a cross-sectional study, 28 patients aged 18 to 65 with BD based on DSM-5 diagnostic criteria were referred to teaching hospitals of AJA University of Medical Sciences in Tehran, and a control group consisting of 28 healthy individuals of the same gender and age entered the study. Written informed consent was obtained from all the study participants and approved by the Ethics Committee of AJA University of Medical Sciences (IR.AJAUMS.REC.1403.088).
The exclusion criteria for participants from the study included mental retardation, any conditions that prevent giving written consent, drug or alcohol abuse in the past month, any history of intravenous drug abuse, history of taking drugs that affect uric acid levels, and women. Pregnant and lactating, gout, chronic inflammatory disease or any other disease associated with hyperuricemia, anemia, history of any infection in the past 2 months, physical trauma or surgery in the previous month, metabolic syndrome, Body Mass Index (BMI) greater than 35, cirrhosis and it was cancer.
Each of the two groups completed the demographic information checklist, and then 3-5 ml of unstimulated saliva and 5 ml of blood were collected from all the participants in the study. After that, the samples were centrifuged at 5000 rpm for 5 min, and the saliva supernatant and serum were separately transferred to a microtube and stored at -70°C until measurement of uric acid levels by photometrically using a kit prepared according to the manufacturer’s instructions (Biorex, Shiraz, Iran). Each sample was measured at least twice, and in case the Coefficient of Variation (CV) was greater than 15%, the measurement was repeated until the CV was less than 15%. The average of repetitions was considered for statistical analysis. The data has been shown as mean±SEM and were analyzed with independent sample t-test, χ2, and ROC test using SPSS 22 (IBM Corp., Armonk, NY, USA). p<0.05 was considered statistically significant.
Results
The average age of disease onset was 30.6 years, and the number of hospitalizations was 4.9.
The demographic information of the healthy group and those with BD are presented in table 1. There was no difference in the average age, body mass index, and education level, and also frequency in gender and smoking, but the frequency of single in the patients was significantly higher.
The average concentration of serum and saliva of uric acid in patients with BD was significantly higher than that of healthy subjects (Table 2).
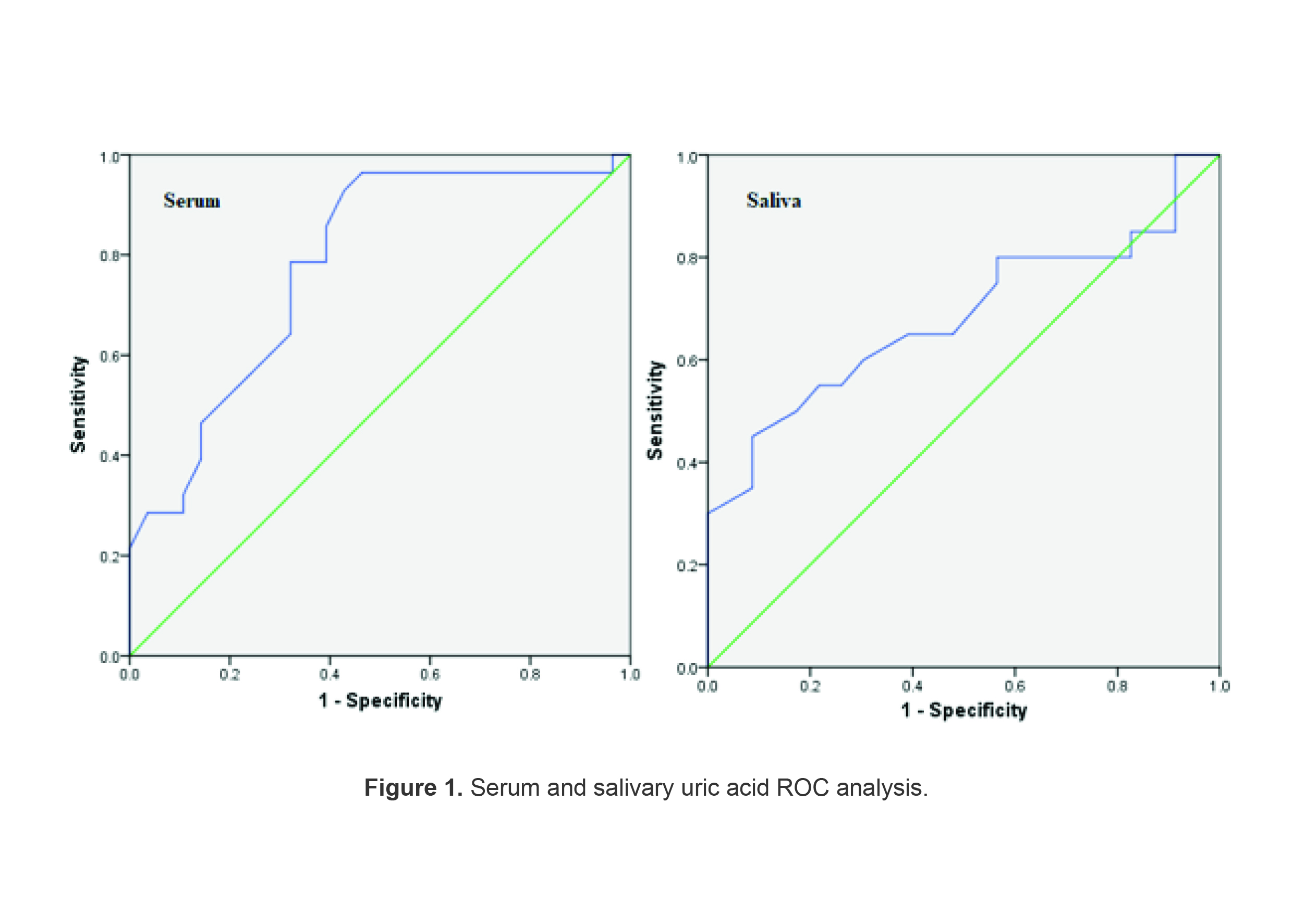
Assuming a cut-off point of 6.4 mg/dL serum uric acid, the sensitivity was 79% and the specificity was 68%. Assuming a cut-off point of 3.3 mg/dL of uric acid saliva, the sensitivity was 65% and the specificity was 61% (Table 3; Figure 1).
Table 1. Demographic information of the patients with bipolar disorder and healthy individuals
|
Variable |
Healthy controls |
Bipolar disorder |
p-value |
|
Age (years) |
36.0±6.6 |
37.4±10.2 |
0.556 |
|
Gender: Male/Female (%) |
15(53.6%)/13(46.4%) |
22(78.6%)/6(21.4%) |
0.089 |
|
BMI (kg/m2) |
26.2±3.8 |
26.2±2.9 |
0.986 |
|
Education (years) |
14.0±2.3 |
13.6±2.1 |
0.469 |
|
Smoking status: Smoker/ Non-smoker |
11(39.3%)/17(60.7%) |
19(67.9%)/9(32.1%) |
0.060 |
|
Marital status: Single/ Married |
9(32.1%)/19(67.9%) |
19(67.9%)/9(32.1%) |
0.015* |
Table 2. Serum and salivary uric acid levels in patients with bipolar disorder and healthy indi viduals
|
|
Healthy |
Bipolar disorder |
95% Confidence interval |
p-value |
|
Serum uric acid |
5.7±0.3 |
7.5±0.3 |
-2.58 to -0.92 |
<0.001 |
|
Saliva uric acid |
3.0± 0.17 |
3.8±0.3 |
-1.50 to -0.03 |
0.033 |
Data are presented as mean±standard error and analyzed with Independent
Student’s t-test and p<0.05 was considered significant.
Table 3. Serum and salivary uric acid cut-off point for differentiating the patients with bipolar disorder from healthy individuals
|
p-value |
Sensitivity (%) |
Specificity (%) |
AUC |
Cutoff |
|
|
<0.001 |
68 |
79 |
0.781 |
6.4 (mg/dl) |
Serum uric acid |
|
0.041 |
61 |
65 |
0.683 |
3.3 (mg/dl) |
Saliva uric acid |
Discussion
Uric acid is produced as the final product of the purinergic system by xanthine dehydrogenase, and the increase in the level of uric acid indicates the acceleration of purinergic transformation and the reduction of adenosinergic transmission, which can be an indicator of manic state ( 25). Determining uric acid amounts in serum and saliva can help diagnose and manage the disease (26). This study aimed to compare the serum and salivary levels of uric acid in BD with healthy individuals. The study demonstrated that the serum and saliva levels of uric acid in BD are higher than in healthy people which is in agreement with various studies considering the increase in serum uric acid levels in BD ( 18,25,27-29).
According to a study conducted by Lu et al (30) in China, patients with BD had higher levels of uric acid than those with major depression, thus uric acid may be a potential biomarker for diagnosing BD from major depression. Chung et al (31) reported that BD patients were at an increased risk of hyperuricemia.
One possible mechanism for the increase in serum and saliva uric acid in patients with BD may be because it has been reported that serum osmolarity is low in BD (12), hence it seems that low osmolarity may cause swelling of body cells, which in turn increases the destruction of some cells. With cell destruction, catabolism of nucleic acids increases, and more purine bases are converted to uric acid. To investigate the validity of this explanation, it is necessary to examine the relationship between serum osmolarity and serum and salivary uric acid, which is one of the limitations of this study.
Today, many studies are being conducted to create and standardize laboratory methods for using saliva as a diagnostic fluid. The main reason for these efforts is the simplicity and non-invasive nature of saliva sampling, which enables easy, low-cost, painless, and frequent sampling of patients. Therefore, it may be useful in the health maintenance program in the diagnosis, monitoring, and screening of diseases (26,32). The results of this study suggested that salivary levels of uric acid as well as its serum level in patients with BD were significantly higher than in healthy individuals. In addition, there was a significant serum and saliva cut-off point for differentiating BD from healthy individuals. Therefore, in BD, saliva contents are probably affected. In addition, serum and salivary uric acid assay may have the potential to be used in the diagnosis of rBD.
Conclusion
It seems that the amount of salivary uric acid increases in patients with BD, which may be used as an auxiliary biomarker for monitoring and diagnosis of the disease.
Acknowledgement
The authors thank the control subjects and patients for their participation in providing samples.
Conflict of Interest
There was no conflict of interest in this manuscript.