Document Type : Original article
Abstract
Background: This study aimed to compare the two methods of pulmonary rehabilitation including continuous and High-Intensity Interval Training (HIIT) on exercise capacity, and quality of life in inpatients with Interstitial Lung Disease (ILD).
Methods: In this clinical trial, 30 patients diagnosed with IPF, were admitted to the pulmonary rehabilitation department and were randomly divided into two groups. In one group, the patients performed continuous training while walking on the treadmill with 60% of the maximum exercise capacity. In the other group, the patients performed HIIT with walking on a treadmill, including 2 min of activity with an intensity of 80% of the maximum exercise capacity, and 2 min of recovery with an intensity of 50 %.
Results: The participants were all Idiopathic Pulmonary Fibrosis (IPF) with a mean age of 12.67±51.50. The mean variables of the six-Minute Walk Test (6MWT) distance, results of the sit-to-stand test, and quality of life (based on a 12-Item Short Form Survey) before and after rehabilitation were significantly different in intragroup analysis. The mean of oxygen saturation, dyspnea, and fatigue before and after rehabilitation in both groups had a significant difference (p<0.001). In the intergroup analysis, the 6MWT distance was significantly improved in favor of the continuous training group (p=0.02), and the quality of life was significantly improved in favor of the high-intensity interval training group (p=0.002).
Conclusion: HIIT was associated with a significant improvement in exercise capacity and quality of life in ILD patients. However, there was no evidence that it was superior to continuous training.
Keywords: Interstitial lung disease, Interval exercise, Training-Pulmonary rehabilitation
Introduction
Interstitial Lung Disease (ILD) is a group of debilitating disorders characterized by degrees of fibrosis and lung inflammation (1). ILD patients are exposed to ineffective and expensive treatments due to the high rate of delayed diagnosis. One of the most important reasons for the delayed diagnosis of this disease is the presence of silent or non-specific symptoms. Symptoms and co-morbidities of ILD patients may exist for years before the definitive diagnosis of the disease. Therefore, many patients are suffering from advanced stages of the disease at the time of referral (2,3).
In most cases, ILD is caused by idiopathic causes, however, occupational factors, connective tissue defects such as sarcoidosis, Non-Specific Interstitial Pneumonia (NSIP), Idiopathic Pulmonary Fibrosis (IPF), and some other rare causes can contribute to disease (4). Patients with ILD often suffer from shortness of breath, cough, fatigue, anxiety, depression, and reduced exercise resistance due to changes in the lung parenchyma and impaired gas exchange (5,6). The destruction and reconstruction of the vascular bed of the pulmonary capillaries lead to a decrease in diffusion capacity, a mismatch of ventilation-perfusion, and as a result, pulmonary hypertension. Therefore, patients usually face arterial hypoxemia, which is aggravated by exercise and physical activity (7,8). In addition to arterial hypoxemia, muscle oxidative stress, systemic disease manifestations, and corticosteroid use increase the dysfunction of skeletal muscles and decrease the patient’s physical activity (8-12). Therefore, exercise tolerance disorder is known as one of the hallmarks of ILD.
Pulmonary rehabilitation is a therapeutic strategy that can improve the quality of life and physical activities of the patients. However, due to various limitations, providing a comprehensive rehabilitation program with long-term benefits for ILD patients has always been challenging. Previously, the positive role of exercise in improving exercise capacity and reducing symptoms such as fatigue and dyspnea of some types of ILD such as IPF has been confirmed (13,14). Foster and Ferreira’s study revealed that exercise included in the lung rehabilitation program of ILD patients can improve dyspnea, quality of life, and functional capacity of these patients (15,16). A Cochrane review that examined the 8-12-week exercise program on 168 ILD patients confirmed the improvement of clinical conditions and the increase in functional capacity of these patients after the exercise period (17). The clinical trial by Dowman et al in Australia confirmed the clinical benefits of exercise training in IPF and asbestosis patients (18).
Pulmonary rehabilitation is usually known as Moderate-Intensity Continuous Training (MICT) as a continuous exercise for 30-60 min with 60-80% maximum heart rate (19). The effectiveness of different modalities of pulmonary rehabilitation in ILD patients has not yet been precisely determined.
High-Intensity Interval Training (HIIT), which is defined as intense exercises with low-intensity intervals or rest (20), can improve peak oxygen uptake and cardiovascular risk factors (21). In many patients with breathlessness, HIIT has been associated with promising results (22-24). Previously, HIIT has been used safely in ILD patients who are candidates for lung transplantation (25). However, a comprehensive guideline for HIIT-assisted lung rehabilitation in ILD patients has not yet been provided. The current study aimed to compare the clinical benefits of HIIT vs. Moderate-Intensity Continuous Training (MICT) in lung transplant candidates with ILD.
Materials and Methods
Study population
Patients with ILD who are candidates for lung transplantation admitted to the pulmonary rehabilitation department of Masih Daneshvari Hospital, Iran based on the study inclusion criteria including age over 18 years, 19Before starting the study, written consent was obtained from the patients and the design protocol was explained to them. How to perform exercises and the role of exercise and physical activity in improving lifestyle were explained to patients in face-to-face visit sessions. All the routine clinical and treatment processes of the patients were monitored by the treatment team and expert doctors. In addition, the treatment team was constantly responding to the patient’s questions and needs during the research, and their level of satisfaction with the exercises was evaluated daily before, during, and after the exercises through face-to-face interviews.
Allocating the patients to groups
In this study, patients were randomly divided into two groups. Patients in the control group performed continuous exercises (walking on the treadmill) with 60% of the maximum exercise capacity. The intervention group performed interval exercises by walking on a treadmill, including 2 min of activity with an intensity of 80% of the maximum exercise capacity, and 2 min of recovery with an intensity of 50%. Both groups of the patients performed 5 min of body grouping exercises with an intensity of 70% of the maximum heart rate before the start of the exercise program, and after finishing their continuous exercises, they cooled down the body for 5 min and 20-30% of the maximum heart rate. The duration of the exercises was 30 min during the period of 10 days. The exercises were performed under the direct supervision of a team consisting of a specialist physiotherapist, a doctor specializing in physical medicine and rehabilitation, lung specialists and nurses in the lung rehabilitation department. Supplemental oxygen was adjusted according to the needs of each patient. Dyspnea was recorded by taking into account the graded Borg scale, percentage of oxygen saturation and heart rate using a pulse oximeter. The sit-to-stand test and the six-Minute Walk Test (6MWT) were performed according to the international protocol. This study was a blind strain, and in order to prevent any possible complications, the specialist doctor and clinical supervisor were fully aware of the assignment of the study groups, and only the responsible data analyst was blind. The information of the patients was provided to the data analyst in coded form.
Measurements
The primary outcome included the patients’ exercise capacity, which was assessed by the 6MWT according to the American Thoracic Society (ATS) protocol (26). For this purpose, the patients were asked to walk as fast as they can in the 30-meter flat corridor of the hospital. The most traveled distance and oxygen saturation determined the patient’s exercise capacity. Dyspnea was assessed using the Borg classification scale (27). Fatigue measurement was done with the Borg scale. The sit to stand test was done based on the international protocol (28). The quality of life was checked with the help of sf-12 questionnaire (29). Sampling was done through total sampling and evaluation of all the available qualified patients.
Statistical analysis
Statistical Package for Social Science (SPSS) software version 24 was used for statistical analysis. Baseline data and exercise index measurements were defined as Mean (M)±Standard Deviation (SD) for normal distribution and median and IQR for non-normal distribution. Independent samples t-test was used to check the difference of quantitative variables of each group before and after rehabilitation (with normal distribution), and Wilcoxon sign rank test was utilized for qualitative variables (without normal distribution). independent t-test was used to understand the difference of quantitative variables with normal distribution between two control and intervention groups, and Mann-Whitney Test was utilized for qualitative variables without normal distribution. A significance level of less than or equal to 0.05 and a 95% Confidence Interval (CI) were considered for all indices.
Results
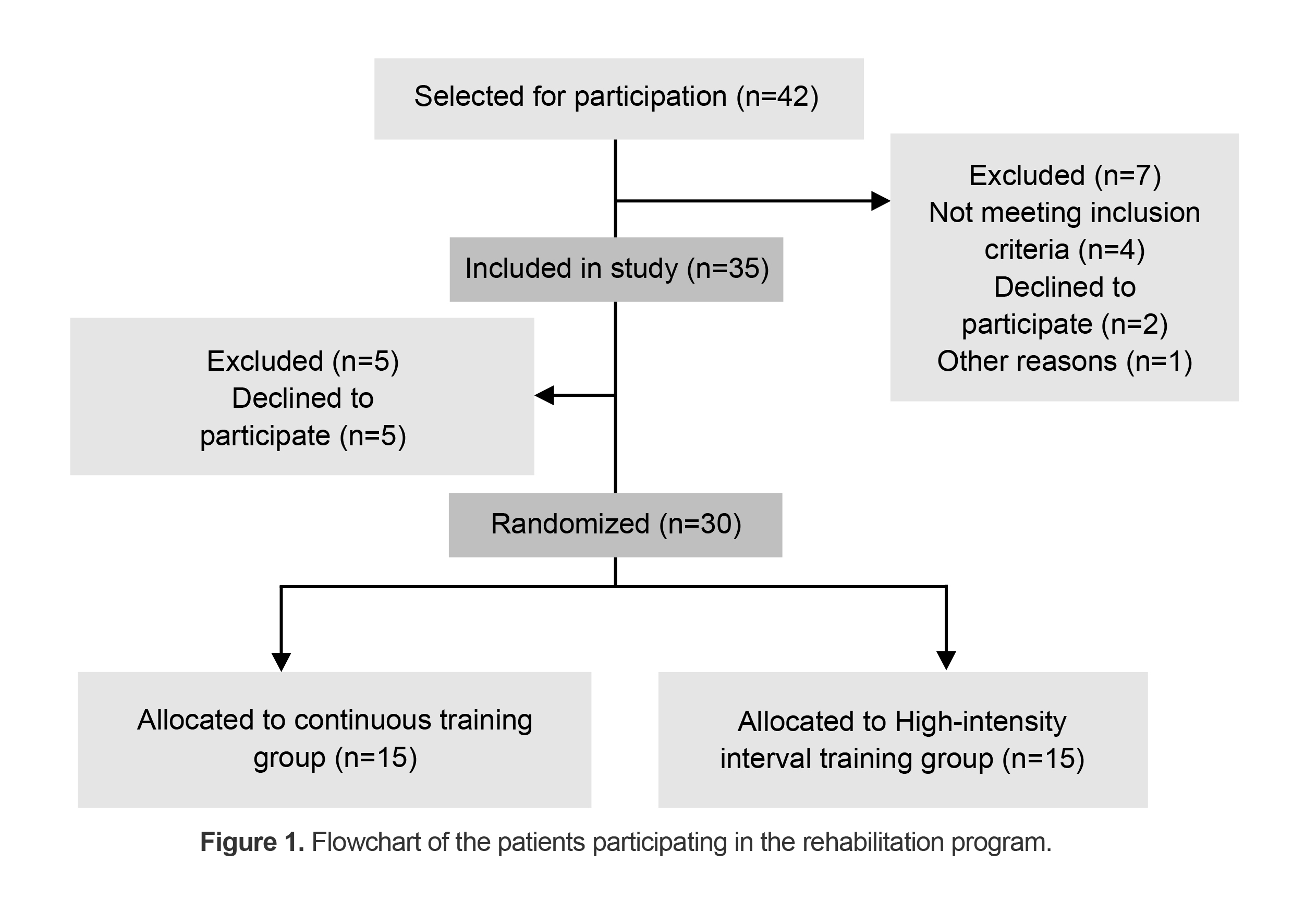
In general, 42 ILD patients were hospitalized in the pulmonary rehabilitation department of the hospital during the period of the study, and 35 of them were included in the study. Five patients were excluded from the study due to the aggravation of some symptoms including muscle pain, shortness of breath, high oxygen loss, and the patient’s unwillingness to continue exercising. Finally, 30 of them completed the pulmonary rehabilitation program. Figure 1 shows the diagram of patients participating in the rehabilitation program of two groups.
Table 1 illustrates the basic and demographic information of the patients participating in the study. In general, the average age of the patients was 51.50±12.67, and 57.5% of them were female. Based on the results presented in this table, there were no significant differences between the study groups in terms of baseline information and patient’s gender.
Table 1. Analysis of the demographic information and baseline variables
|
Character |
Continuous training |
High-intensity interval training |
Sig. (p-value) |
|
Age (yrs); mean±SD |
49.05±15.76 |
53.95±8.30 |
0.226 |
|
Gender; N(%), Male/Female |
9(45.00)/11(55.00) |
8(40.00)/12(60.00) |
0.756 |
|
Height (cm); mean±SD |
166.00±7.45 |
163.40±6.48 |
0.246 |
|
Weight (kg); mean±SD |
66.60±6.29 |
66.70±6.94 |
0.922 |
|
6MWTD (m); mean±SD |
281.75±67.07 |
301.15±59.06 |
0.338 |
|
SF-12 (total) |
61.75±11.22 |
56.50±15.17 |
0.221 |
|
Sit to stand |
19.50±1.88 |
19.65±1.09 |
0.759 |
|
Borg dyspnea scale median (IQR) |
4.50(1.00) |
4.50(1.00) |
|
|
Oxygen saturation; median (IQR) |
3.00(2.00) |
4.00(2.00) |
|
|
Fatigue: median (IQR) |
2.50(1.00) |
3.00(1.00) |
|
|
Fatigue; Z based on Mann-Whitney Test |
-0.67 |
0.578 |
|
|
Borg dyspnea scale; Z based on Mann-Whitney Test |
-0.44 |
0.696 |
|
|
Oxygen saturation; Z based on Mann-Whitney Test |
-1.48 |
0.145 |
|
Abbreviations; yrs: years, SD: Standard Division, N: number, 6MWTD: 6-Minute Walk Test Distance, IQR: Interquartile Range.
Results of pulmonary rehabilitation in continuous and interval groups Six-minute walk test
Examining the 6MWT results of the patients participating in the study demonstrated that the average distance traveled in this test before and after lung rehabilitation in each group has a significant difference(p<0.001) (Table 2). In the intergroup analysis, the difference in the average distance traveled in the six-minute walking test of the patients in the continuous training group was significantly higher than in the high-intensity interval training group (p=0.02) (Table 3).
Table 2. Descriptive statistics and t-test results in the study groups
|
Variables |
Continuous training (M±SD) |
p-value |
High-intensity interval training (M±SD) |
p-value |
||
|
Before |
After |
Before |
After |
|||
|
6MWTD |
281.75±67.07 |
302.45±67.04 |
<0.001* |
301.15±59.07 |
313.85±60.37 |
<0.001* |
|
SF-12 |
61.75±11.22 |
62.65±11.18 |
<0.001* |
56.50±15.17 |
59.75±13.80 |
<0.001* |
|
STST |
19.50±1.88 |
22.60±1.60 |
<0.001* |
19.65±1.09 |
23.00±0.92 |
<0.001* |
Abbreviations; 6MWTD: 6minute walk test distance,SF-12: The 12-Item Short Form Health Survey, STST: Sit-to-stand test, * significant p value<0.05.
Sit to stand
Examining the data obtained from the sit to stand test showed a significant difference in each of the continuous and interval groups before and after lung rehabilitation (p<0.001 and p<0.001, respectively) (Table 2). Meanwhile, the intergroup analysis of this test indicated that pulmonary rehabilitation showed no significant difference in the average STOS results before and after the rehabilitation (Table 3).
Table 3. Independent samples T-test analysis of significance difference between the variables by study groups
|
Variables |
Continuous training (M±SD) |
High-intensity interval training (M±SD) |
Mean difference |
T test p-value |
|
6MWTD |
20.70±12.59 |
12.70±8.11 |
8.00 |
0.02* |
|
SF-12 |
0.90±0.97 |
3.25±3.02 |
2.35 |
0.002* |
|
STST |
3.10±1.80 |
3.35±1.35 |
0.25 |
0.622 |
Abbreviations; 6MWTD: 6-minute walk test distance, SF-12: The 12-Item Short Form Health Survey, STST: Sit-to-stand test, * significant p value<0.05.
Quality of life
The quality of life of the patients in this study was evaluated using the sf-12 quality of life questionnaire. The reviewed results showed that the mean scores in the quality-of-life questionnaire in the continuous group and the HIIT group before and after lung rehabilitation had a significant difference (p<0.001) (Table 2). Examining the quality of life of the participating patients in the two groups showed that the mean of quality of life of the two groups has a significant difference (p=0.002) (Table 3).
Oxygen saturation
Examining the decrease in oxygen saturation percentage of patients in the continuous group revealed that the decrease in saturation before and after rehabilitation has a significant difference (p<0.001) (Table 4). In patients of the HIIT group, changes in oxygen saturation were also significant (p<0.001) (Table 4). Moreover, no significant difference was observed in the changes of oxygen saturation of the two groups under the information (p=0.35) in the intra-group comparison (Table 4).
Table 4. Results of Wilcoxon’s signed rank test and Mann-Whitney Test for study groups
|
Variables |
Continuous training |
High-intensity interval training |
Mann-whitney test for study groups |
|||||
|
Mean ranks |
Z |
Sig. (two-tailed) |
Mean ranks |
Z |
Sig. (two-tailed) |
Z |
Sig. (two-tailed) |
|
|
Fatigue |
9.00 |
-3.75 |
<0.001* |
9.50 |
-3.83 |
<0.001* |
0.046 |
0.46 |
|
Dyspnea |
7.77 |
-3.11 |
<0.001* |
6.77 |
-2.85 |
<0.001* |
0.611 |
0.46 |
|
Oxygen saturation |
17.23 |
-3.31 |
<0.001* |
9.00 |
-3.69 |
<0.001* |
0.317 |
0.35 |
Dyspnea
Examining the mean of dyspnea before and after rehabilitation showed that in the continuous group, lung rehabilitation exercises caused significant changes in the mean of this variable compared to before rehabilitation (p<0.001). Similarly, there was a significant difference in mean of dyspnea before and after rehabilitation in the interval group (p<0.001) (Table 4). Examining the mean of dyspnea between the continuous and interval groups showed no significant difference in the scores of this variable (p=0.64) (Table 4).
Fatigue
The results of the fatigue analysis revealed that the mean of this variable was significant in each of the continuous and HIIT groups (both groups p<0.001) (Table 4). However, in the inter-group comparison, no significant difference was observed in the mean of fatigue of the two groups with different lung rehabilitation methods (Table 4).
Discussion
The results of this study confirmed the effectiveness of pulmonary rehabilitation exercises using continuous and high-intensity interval training programs in significantly improving the quality of life and 6MWT results of hospitalized IPF patients. Most of the past studies have examined this training in outpatients. Studies have shown that exercise training significantly improves shortness of breath, 6MWT and quality of life in IPF patients and other ILD cases (30,31).
Holland et al demonstrated the positive role of exercise training in improving dyspnea and 6MWT of IPF patients (14). Perez-Bogerd et al also obtained similar results and confirmed the role of pulmonary rehabilitation in improving 6MWT and quality of life of ILD patients (32).
Due to physical disability, ILD patients are able to carry out limited exercise and rehabilitation programs. On the other hand, without considering the promising evidence, it cannot be concluded that drug treatments alone have the expected effectiveness and the toxic effect of consumed drugs can be associated with serious complications for some ILD patients (33). Therefore, it is challenging to provide a comprehensive and homogeneous guideline for these patients. So far, no clinical trial study has provided a standard and universal rehabilitation exercise program for ILD patients (14,34,35). In addition, the improvement of the respiratory function of these patients after rehabilitation programs has been associated with different results (4). The improvement of shortness of breath and quality of life after rehabilitation in both of the groups can be related to the increase in respiratory demand during exercise and the increase in elasticity and expansion of the pleura. Therefore, increasing peak minute ventilation (VE) and tidal volume (VT) and improving pulmonary compliance can play a significant role in improving dyspnea (34,36,37).
According to the results, the functional capacity of the patients improved significantly before and after rehabilitation. In addition, dyspnea and fatigue in patients of both study groups improved significantly before and after the developed rehabilitation program, however, no significant difference was found in these variables in intergroup analysis. Interestingly, a significant difference was observed in the results of 6MWT distance and the quality of life of the two groups. In the intergroup analysis, it was observed that the patients in the continuous training group covered more distance in the six-minute walking test, while the quality-of-life index improved in favor of the HIIT group. This point highlights the importance of paying attention to the type of lung rehabilitation program in patients with different tolerance.
It was shown that dyspnea, fatigue, and decrease in oxygen saturation percentage of IPF patients were not different in the intergroup analysis of patients undergoing continuous HIIT exercises, therefore, HIIT can also be used in the pulmonary rehabilitation programs of ILD patients according to the patient’s conditions and facilities.
Standard rehabilitation is at least 8 weeks with 2-3 day. In this study, the rehabilitation program of the hospitalized patients was carried out daily for 10 days. The present study was a pilot study to provide a rehabilitation program for hospitalized IPF patients.
Study limitations
The results showed the applicability of HIIT as a safe and accessible pulmonary rehabilitation program for patients in the inpatient phase. However, two methods of pulmonary rehabilitation during hospitalization were only examined. This study was conducted in the only inpatient pulmonary rehabilitation center in Iran. In addition to being single-centered, the sample size has been another limiting factor of the current study. Using a larger sample size and comparing different types of exercises in various subgroups of ILD can help to obtain valid results.
Conclusion
The present pilot study showed the feasibility of pulmonary rehabilitation with the help of HIIT programs for ILD patients. However, there was no evidence of the superiority of this method over continuous training. Despite the proven effectiveness of HIIT-based rehabilitation programs, the implementation of these exercises requires more and more careful monitoring than conventional exercises. The results of this study cannot be generalized to other patients with various types of interstitial lung diseases. Thus, further studies are required.
Acknowledgement
This study was approved by the local biomedical research ethics committee of the Masih Daneshvari Hospital (IR.SBMU.NRITLD.REC.1401.107) and was registered in the clinical trial system (IRCT20160516027929N12). The authors are grateful to all those who contributed to this study.
Conflict of Interest
There was no conflict of interest in this manuscript.