Document Type : Original article
Abstract
Background: Recent evidence suggests a connection between celiac disease and dilated cardiomyopathy. Herein, we serologically screened for celiac in dilated cardiomyopathy patients and investigated its correlation with ejection fraction.
Methods: We selected 123 cardiomyopathy patients. Patients were screened for celiac, using anti-tissue transglutaminase (ATA), anti-gliadin (AGA), and anti-endomysial (EMA) immunoglobulin type A (IgA) antibodies. Total IgA levels were also measured.
Results: Of 123 patients, 3 were EMA positive (2.4%), 4 were AGA positive (3.3%) and 5 were ATA positive (4.1%). EMA positive patients had significantly lower EF values compared to EMA negative patients (35±5 vs. 46.52±9.21, p-value: 0.034). Similar results were observed for AGA (32.5±14.34 vs. 46.7±8.8, p-value: 0.002), but not for either ATA positivity (40±10 vs. 46.5±9.21, p-value: 0.126) or IgA deficiency (50±5 vs. 46.14±9.37, p-value: 0.480). No significant difference was observed in the age and gender of seropositive patients compared to seronegative.
Conclusion: We observed a higher prevalence of celiac seropositivity among dilated cardiomyopathy patients compared to the general population. EMA and AGA positive patients had significantly lower ejection fractions compared to their negative counterparts.
Keywords: Celiac disease, Dilated cardiomyopathy, Ejection fraction, Serology
Introduction
Celiac Disease (CD) is an inflammatory gastrointestinal disorder in genetically predisposed individuals, with a reported prevalence of up to 1% in some countries (1). Recent studies suggested that CD is a multisystem disorder that can present or coexist with cancer (2), other autoimmune disorders (3), tuberculosis (4), and adverse outcomes in patients with cardiovascular diseases (5). The standard diagnostic modality is the endoscopic duodenal biopsy, which is an invasive procedure (6). Serologic tests are used as adjuncts to biopsy and also as screening tests for early detection of CD (7,8). These tests include anti-gliadin (AGA), anti-tissue transglutaminase (ATA), and anti-endomysial antibodies (EMA) (9-11). Previous studies reported celiac seropositivity of about 0.2- 0.6% for EMA, 1% for ATA, and 2.4% for AGA in the Iranian general population (12,13).
Dilated Cardiomyopathy (DCM) is one of the most common non-ischemic causes of heart failure with a prevalence of 1 in 2500 individuals (14). DCM is characterized by systolic dysfunction and atrioventricular enlargement which can lead to conduction disturbance, low cardiac output, thromboembolism, and sudden cardiac death. Diagnosis is based on clinical evaluation, in addition to echocardiography and cardiac MRI (15).
Recent evidence suggests a correlation between CD and different types of DCM (16-30). DCM was even the first presentation of CD in some patients (31,32). In addition, a correlation between EMA and ATA was reported with DCM (33,34). There is also growing evidence that a gluten-free diet can result in better cardiac function in DCM cases associated with CD (35,36).
To the best of our knowledge, only a few studies evaluated the correlation between CD seropositivity and cardiac function in DCM patients. In this study, we aimed to serologically screen for CD in a sample of DCM patients and evaluate the correlation of CD seropositivity with EF, as a marker of cardiac function and disease severity.
Materials and Methods
This cross-sectional study was conducted on 150 patients in Tehran Heart Center, a referral cardiology hospital located in Tehran in 2018. The inclusion criteria consisted of ages between 18 to 80 years and an established diagnosis of DCM based on the World Health Organization (WHO) criteria (37). The exclusion criteria included a previous diagnosis of CD, a history of chronic diarrhea and malabsorption due to other specified diseases, and a lack of consent to participate in the study. 27 patients were excluded based on the criteria and 123 patients remained in the study for further evaluations. Written informed consent was taken from all the patients in advance. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki (6th revision, 2008) as reflected in a priori approval by the institution’s human research committee.
Demographic data including age and gender, as well as patients’ most recent Ejection Fraction (EF) measurements (using biplane simpsons method in echocardiography), were obtained from the Tehran heart center database. The timing difference between EF measurement and serologic testing was less than 3 months in all patients.
10 ml of blood were taken from each patient and transferred to the laboratory in standard conditions of ATA, AGA, and EMA immunoglobulin A type (IgA) antibodies, as well as total serum IgA levels, were measured. IgA levels were measured to rule out IgA deficiency, as a cause of CD serology unreliability.
ATA and AGA levels were tested using EUROIMMUN® ELISA-based test kits (Medizinische Laboradiagnostika AG, Germany). Serum samples obtained from patients were diluted 1:201 in sample buffer and were transferred into microplate wells (coated with antigens) along with calibrators (200 relative U/ml of IgA, human). The samples were incubated for 30 minutes at room temperature (+18 to +25 °C). Afterward, 100 µl of enzyme conjugate (peroxidase-labeled anti-human IgA) were pipetted into each of the microplate wells. The wells were then incubated for another 30 minutes at room temperature. Following the above steps, 100 µl of chromogen/substrate solution (tetramethylbenzidine/hydrogen peroxide) were pipetted into each of the wells, which were then incubated for 15 minutes at room temperature. Finally, the reaction was stopped by using 100 µl of stop solution (0.5 mol sulphuric acid) in the same order and pace as the substrate solution, and photometric measurements of color intensity were made at 450 nanometers of wavelength (and a reference wavelength of 620 to 650 nanometers) within 30 minutes. Levels of more than 20 and 18 relative U/ml were considered positive for ATA and AGA, respectively.
EMA levels were measured by means of an indirect immunofluorescence assay using microtiter plates coated with purified endomysial antigens. Briefly, the sections were incubated for 60 minutes with the subject’s serum diluted 1:100. After washing, the sections were incubated with fluorescein-labeled goat anti-human IgA antibodies for 30 minutes. Once again after washing, 100 µl of chromogen/substrate solution (tetramethylbenzidine/hydrogen peroxide) were pipetted into each of the plates, which were then incubated for 15 minutes at room temperature. Finally, the reaction was stopped by using 100 µl of stop solution (0.5 mol sulphuric acid) in the same order and pace as the substrate solution. The slides were then washed and examined by fluorescent microscopy. Levels of more than 20 U/ml were considered positive.
Total IgA levels were measured using Hitachi 911 automatic analyzer (Chema Diagnostica, Italy), which is a spectrophotometric assay, and measurements of color intensity were performed at 600 nanometers of wavelength. Levels of less than 80 mg/dl considered IgA deficient.
Statistical analysis was performed using the SPSS software (Statistical Package for Social Science, Chicago, Illinois, USA) version 21. Seropositivity for each antibody was reported as a number and percent of patients. Patients were then sorted into 2 groups (positive vs. negative) according to standard values of positivity for each antibody. Mean age and EF were compared for two groups using independent samples t-test. Correlation between gender and antibody positivity was investigated using the Chi-square test. p-values of less than 0.05 were considered significant.
Results
Of the initial 150 patients included, 123 patients remained in the study based on exclusion criteria. Mean and Standard Deviation (SD) of age were 58±9.5 (males:55.9±9.2, females:60.1±8.6). Gender distribution was almost equal with 61 (49.6%) males and 62 (50.4% ) females. Three patients were EMA positive (2.4 %, all male), 4 patients were AGA positive (3.3%, all male), and 5 patients were ATA positive (4.1%, 4 males). Three of the patients had IgA deficiency (2.4%, 2 male) and were seronegative for all 3 antibodies as well. The mean and SD of patients’ EF was 46.2±9.29.
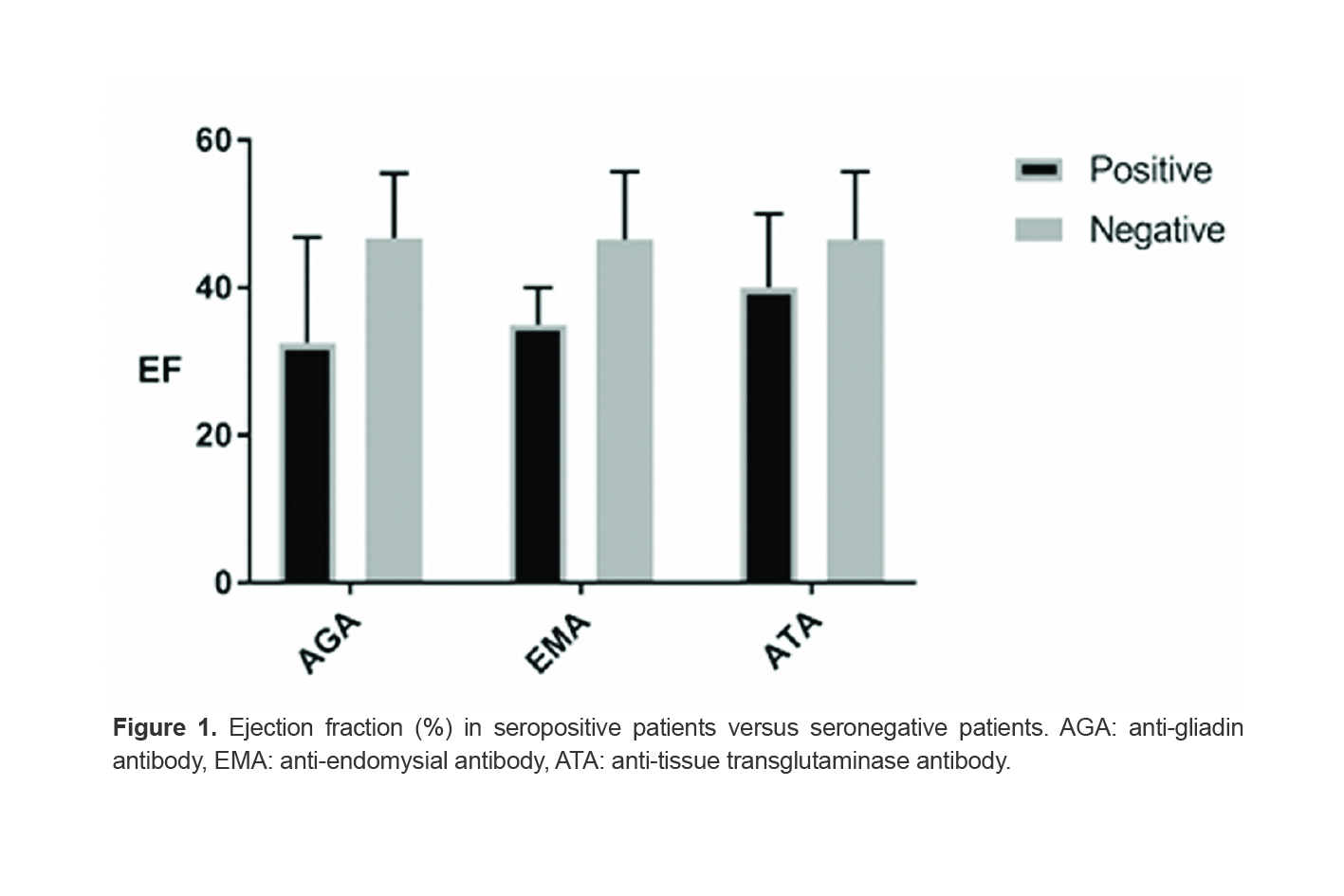
Seropositive patients had lower EF values compared to antibody negative patients (Figure 1).
This decline was statistically significant for EMA positive (35%±5 vs. 46.52%±9.21, p-value:0.03) and for AGA positive patients (32.5%±14.34 vs. 46.7%±8.8, p-value: 0.002), but not for either ATA positivity (40%±10 vs. 46.5%±9.21, p-value: 0.126) or IgA deficiency (50%±5 vs. 46.14%±9.37, p-value: 0.480).
There was no significant age difference between seropositive and seronegative groups of either ATA (53.4±18.95 years vs. 58.26±8.91 years, p-value: 0.59) or EMA (49.67±18.23 vs. 58.27±9.21, p-value: 0.125). The same was also true for IgA deficient vs. non-deficient subgroups (67.5±0.7 vs. 57.81±9.55, p-value: 0.157). However, the AGA positive patients were significantly younger compared to AGA negatives (41.33±10.59 years vs. 58.54±9.09 years, p-value: 0.002).
There was also no significant difference between male and female subgroups regarding ATA (4 vs. 1, p-value: 0.165) and EMA positivity (3 vs. 0, p-value: 0.077) and IgA deficiency (2 vs. 1, p-value: 0.549). On the other hand, there were significant differences between AGA positive and negative subgroups regarding gender (all 4 cases male, p-value: 0.040).
Discussion
The prevalence of celiac disease seropositivity among DCM patients is higher than the reported prevalence among the general population of Iran. We observed ATA and EMA positivity of about 4 folds higher than that reported in the general population (12,13), which is consistent with findings in previous studies for both antibodies (24,27,34).
Interestingly, EF values were lower in seropositive patients for all 3 antibodies, although this decline was only statistically significant in EMA and AGA positive patients compared to their negative counterparts. To the best of our knowledge, previous studies failed to evaluate this correlation. However, our results should be interpreted with caution since the explanation of CD seropositivity in DCM is not yet completely determined and might be due to a common pathophysiologic condition rather than CD itself.
A number of studies investigated the prevalence of CD among adults and children with different types of DCM (17-20,24,36). For instance, Not et al screened 238 patients diagnosed with DCM, 418 of their relatives, and 2000 healthy blood donors for CD using ATA, EMA (both IgA and IgG subtypes, unlike our study which included only IgA subtypes), Human Leukocyte Antigen (HLA) types DQ2 and DQ8 and duodenal biopsy to confirm the diagnosis of CD (27). Their findings suggested a correlation between CD and DCM, although a causal relationship was not elucidated, neither were the associations of antibodies with EF.
On the contrary, Vizzardi et al found no evidence regarding the higher prevalence of CD among DCM patients (38). Ischemic and idiopathic DCM patients underwent serologic testing for ATA and were further evaluated by endoscopy and biopsy in case of ATA positivity. CD prevalence was not statistically different from the Italian general population. Furthermore, the patients showed no improvement regarding their cardiac function in echocardiography after one year on a gluten-free diet. They hypothesized that seropositivity might be confounded by unrecognized similar conditions in CD and DCM patients rather than an etiologic association.
There has been an ongoing debate regarding the test of choice for CD screening in patients with heart failure. De Bem et al studied a group of heart transplant candidates for EMA and ATA IgA positivity (19). Seropositive cases underwent endoscopy and biopsy. However, only EMA positive patients showed histopathologic evidence of CD. Consistent with their findings, Peracchi et al observed a high prevalence (50%) of ATA seropositivity in a group of EMA negative end-stage heart failure patients with no clinical evidence of CD, with an estimated CD prevalence of about only 2% (34). The authors argued that the high prevalence of ATA positivity in asymptomatic cases was more related to underlying cardiac conditions rather higher than the expected diagnosis of CD. Tissue-transglutaminase may be involved in fibrogenesis and apoptosis (39). Therefore, elevated ATA levels in DCM may be due to overexpressed cardiac tissue-transglutaminase, as described in some experimental models of heart failure (40). Thus, EMA can be the test of choice for CD screening in this patient population. Interestingly, EMA was correlated with lower EFs and not ATA in our study.
Age and gender differences among positive and negative subgroups were only significant for AGA. This finding might be due to our small sample size or higher rates of AGA positivity compared to ATA and EMA in the younger population similar to what was observed in a pediatric study (41). It is also notable that AGA has been less frequently studied than EMA and ATA in previous articles and to our knowledge, this is the first study to report a higher prevalence of AGA among DCM patients and its probable link to poor left ventricular function.
Our study had numerous limitations. First, our sample size was limited and we did not have a control group of neither healthy individuals nor patients with other causes of heart failure to compare serology results. We also tested only for IgA antibodies, hence we screened for IgA deficiency in our sample to detect possible CD patients without positive IgA antibodies. However, the mean EF was not significantly different from other patients. Most importantly, our study was based solely on serologic tests for CD and we did not perform endoscopy or HLA testing on seropositive patients to further validate the results (due to ethical and financial limitations). However, we do hope to expand our study in the future by further validating our results using biopsy samples with vast sample size and a proper control group. In addition, studying the effect of a gluten-free diet on this patient population could be evaluated as a feasible approach to affect patients’ prognosis. With all these limitations in mind, this study is the first study in this field on Iranian DCM patients and can be used as the initial step for further studies.
Conclusion
We observed a higher prevalence of CD seropositivity among DCM patients. EMA and AGA positivity was also correlated with lower EFs. Despite these findings, the pathophysiology of antibody increase in DCM patients has not yet been completely determined and our results should be interpreted with caution. Further evaluation of CD seropositivity in DCM patients compared to healthy controls and patients with heart failure due to other causes, as well as seropositivity correlation with disease severity and response to a gluten-free diet is recommended.
Conflict of Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.