Document Type : Original article
Abstract
Background: The prevalence of negative act behaviors among medical residents has not yet been assessed in our country. Present study aimed at evaluating the prevalence and impact of negative act behaviors among residents of four academic hospitals in Iran.
Methods: This cross-sectional survey was conducted on medical residents in two educational hospitals affiliated to Iran University of Medical Sciences. An online electronic questionnaire was distributed to all clinical residents in these hospitals via WhatsApp. We used an online electronic four-part questionnaire including demographic data, Negative Act Questionnaire-Revised (NAQ-R), some questions on negative behaviors causes and effects, and General Health Questionnaire 12 (GHQ-12).
Results: In total, 254 completed questionnaires were received, with an overall response rate of 71%. Ninety five percent of participants had experienced negative act behaviors once or more during the last six months, whereas 91% of responders had witnessed negative act behaviors during this time. The most common source of these behaviors were senior residents (73.8% of those bullied, n=178). There was a significant positive correlation between the GHQ score and the NAQ-R score assays.
Conclusion: This study, as the first study on the prevalence of bullying and negative acts in Iranian medical residents, showed that the medical education atmosphere in residency is not optimal. Therefore, there is a need for certain interventions in the medical education environment. We recommend better education of residents and faculty members, strong policy making, situation assessment and feedback regulations as essential steps towards diminishing bullying and negative behaviors in resident training centers.
Keywords: Iran, Mental health, Occupational stress, Residency
Introduction
Bullying is defined as a persistent behavior against a person which is degrading and intimidating and could lead to undermining self-esteem and confidence in him/her (1). Bullying could take many forms from subtle behaviors to obvious abuse that negatively affects the confidence, mental health and progress of the victim (2). Workplace bullying in the health care system is a critical and persistent problem. Its importance could be evaluated from different aspects as at an organizational level, it could cause substantial financial costs. In the UK, the total cost of bullying for organizations in 2007 was estimated at approximately £13.75 billion (3,4).
The effect of bullying, harassment and negative act behaviors on health care system personnel as well as patients is of great importance as doctors, nurses, and other medical staffs are affected by bulling every day. Unfortunately, most of these behaviors could negatively impact health care system ability to care for patients (5).
In Iran, residency programs last three to five years. During these programs, residents are trained to practice medicine under the supervision of senior residents and faculty members. The structure of academic medicine is hierarchal in which there is a closed environment that is often run by its own staffs without the intervention and supervision of others. In such environment bullying may be more widespread than other medical settings (6). In academic hospitals, medical students as well as residents could also be affected (7-9).
The reported prevalence of bullying, harassment and mistreatment in the residency period varies based on various methods of bullying assessment and differences in culture. Previous papers have reported the prevalence of mistreatment and negative acts as 44-78% (10,12). Exposure to bullying could lead to depression, feeling of unworthiness and incompetence, substance abuse, suicidal attempts, psychosomatic and musculoskeletal complaints, and even increase in the risk of cardiovascular diseases (13,14).
To date, the prevalence of bullying, harassment and negative act behaviors among medical residents has not yet been assessed in our country. Therefore, the present study was aimed at evaluating the prevalence and impact of negative act behaviors among residents of four academic hospitals in Iran.
Materials and Methods
Participants
This cross-sectional survey was conducted on medical residents in two educational hospitals (Firoozgar Hospital and Rasoul-e-Akram Hospital) affiliated to Iran University of Medical Sciences (IUMS) from March 2021 to May 2021. These hospitals are large academic general hospitals affiliated to IUMS. An online electronic questionnaire was distributed to all clinical residents in these hospitals via WhatsApp. All participants had a minimum clinical experience of six months, being first to fourth-year residents. A reminder was sent to all the participants after 2 weeks.
Data collection
We used an online electronic four-part questionnaire. Prior to initiating this step, a full explanation of the purpose of the study and the definitions of bullying and negative act behaviors were provided to all the participants.
In the first part of the questionnaire, in a researcher-developed demographic sheet, the demographic data including age, gender, educational status, specialty, residency year, etc. were recorded.
For the second part of the questionnaire, the Negative Act Questionnaire-Revised (NAQ-R) was utilized. NAQ-R was designed by Hoel and Notelaers as a validated 22-item questionnaire which is widely used to measure workplace bullying in different languages (15). The participants should imagine the last 6 months of their workplace and respond to the 22 items of bullying behaviors by a 5-point Likert scale as never (1 point), sometimes (2 points), each month (3 points), each week (4 points) and each day (5 points). Although the validity and reliability of this questionnaire has been confirmed in previous studies, but its main problem is the recalling of related occasions that may also differ each day from each week. Therefore, in order to increase the accuracy of the responses, we changed the scale of the questionnaire to a 4-point Likert scale consisting of never (1 point), rarely (2 points), sometimes (3 points), and frequently (4 points). This scale has also been validated in previous studies (16,17). For analysis, each question in the NAQ-R was scored as 1-4 with 1 for events never occurred and 4 for those occurring frequently. Previous researchers (18,19) have divided the 22 items of the NAQ-R into three main categories of bullying including work-related bullying, person-related bullying and physical intimidation-related bullying. The questionnaire was analyzed by the Chowdhury et al method (18) in total and for the 3 mentioned domains. We calculated the Mean Bullying Score (MBS) in total and for each domain of bullying by computing mean scores.
In part three, the residents were asked to specify who subjected them to bullying, whether their health had been affected by bullying behaviors, and if they had witnessed other residents being bullied. In this part of questionnaire, the residents were asked to disclose their thought regarding suicide, injury to the person who was the source of bullying and withdrawal from education due to bullying behaviors.
To assess the impact of bullying on mental health, in the final part of the study questionnaire, we used the General Health Questionnaire 12 (GHQ-12) which lists 12 items, each assessing the severity of a mental problem over the past six months (20,21). Responders scored each item considering how they had been feeling about that item during the past six months based on a 4-point Likert scale (less than usual, no more than usual, rather more than usual, or much more than usual). The two most common scoring methods for analyzing the GHQ12 are the bi-modal (0-0-1-1) and Likert (0-1-2-3) scoring methods (22,23). The scores were used to generate a total score ranging from 0-12 in the bimodal scale and 0-36 in the Likert scale, with higher scores indicating the worst conditions the participants had experienced (24). Based on the previous studies, we utilized both methods for analysis and set 3.7 and 14.5 as the cut-off values for mental health status (21). Both the GHQ-12 and NAQ-R were translated into Persian and further confirmed the reported reliability and validity of these questionnaires in previous studies (21,25).
Data analysis
The data were analyzed by the Statistical Package of Social Sciences for Windows version 20 SPSS 20 (IBM Corp., Armonk, New York, USA). Kolmogorov-Smirnov test was used to test the normal distribution of the data. Differences between normally distributed continuous variables and non-normally distributed variables were assessed using independent sample t-test and non-parametric tests, respectively. A p-value<0.05 was considered as statistically significant.
Ethical concerns
The study protocol was approved by the Ethics Committee of IUMS (IR.IUMS.REC.1399.1273) and supported by the Education Development Center of Iran University of Medical Sciences.
Results
In total, 254 completed questionnaires were received, with an overall response rate of 71% (254/357). The number of male and female participants was 102 and 152, respectively with a mean age of 31.8±4.7 yrs. Chronic medical diseases were reported by 3.9% (n=10) of the responders whereas none of the responders had a disability. The largest group of participants were second-year residents (29.1%). Baseline characteristics of the studied participants are presented in table 1.
Table 1. Demographic data of the participants
|
Sex |
|
|
|
|
Male Female |
102 (40%) 152 (60%) |
|
Age (years) |
31.8±4.7 |
|
|
Residency year |
|
|
|
|
First year |
36 (14%) |
|
|
Second year |
74 (30%) |
|
|
Third year |
70 (28%) |
|
|
Fourth year |
70 (28%) |
|
Working site |
|
|
|
|
Work in operation room |
135 (53%) |
|
|
Did not work in operation room |
119 (47%) |
|
Underline disease |
|
|
|
|
Physical illness |
10 (4%) |
|
|
Psychological disease |
4 (2%) |
|
Negative thoughts |
|
|
|
|
Withdrawal from education |
109 (42.9%) |
|
|
Suicide |
9 (3.5%) |
|
|
Injury to others |
8 (3.1%) |
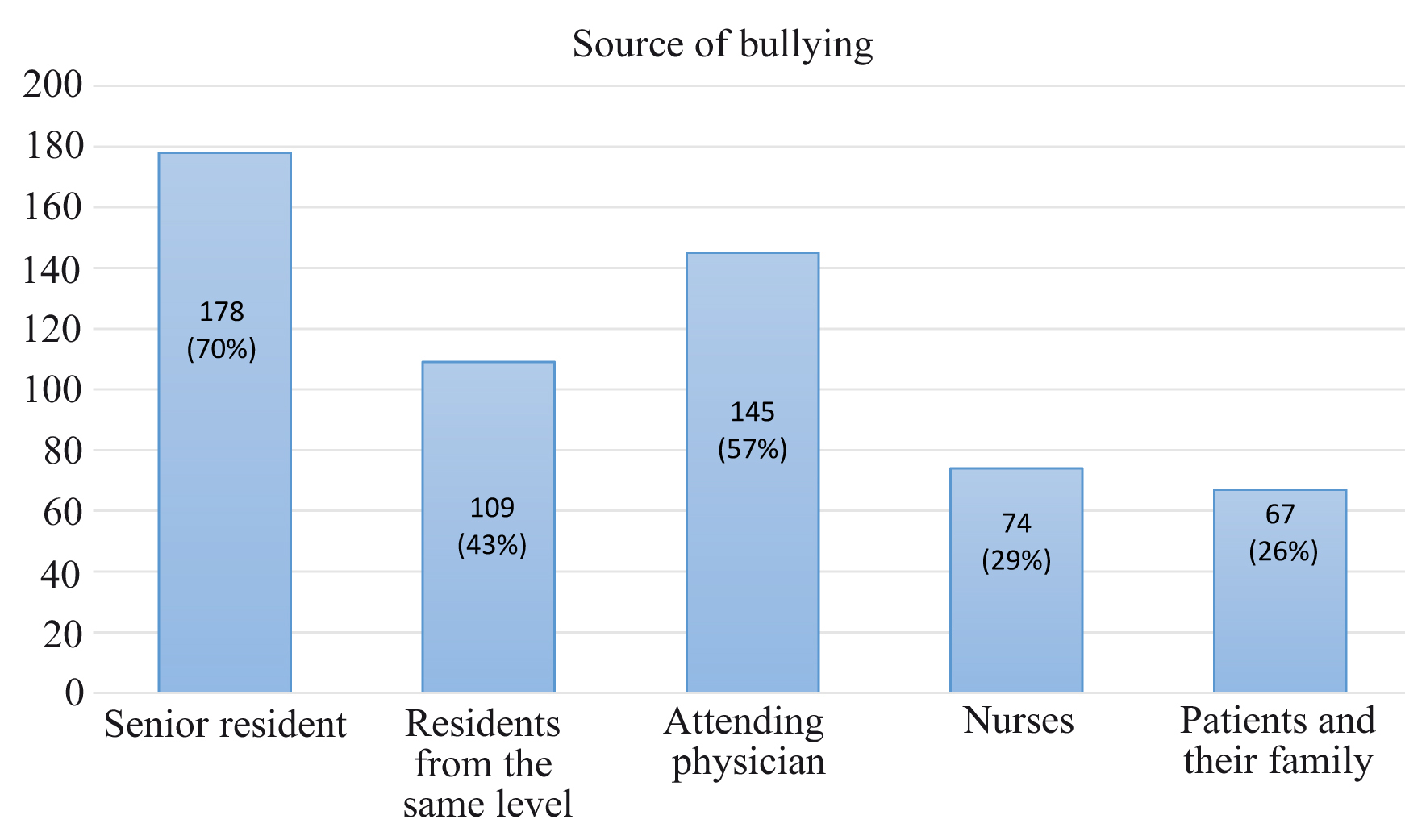
This study showed that 95% of the participants had experienced negative act behaviors once or more during the last six months, whereas 91% of the responders had witnessed negative act behaviors during this time. “Negative act behavior” was defined as each negative behavior listed as a NAQ-R item. Based on the responders who had experienced negative act behaviors, the most common source of these behaviors were senior residents (73.8% of those bullied, n=178), followed by attending physicians (60.1% of those bullied, n=145) (Figure 1).
Table 2 shows the prevalence of 22 negative behaviors among medical residents based on the NAQ-R. The most frequent negative behaviors were “Being ordered to do work below your level of competence” and “Being exposed to an unmanageable workload”. The 22 items of the NAQ-R questionnaire were divided into three main categories of bullying including; work-related bullying, person-related bullying and physical intimidation-related bullying (18, 19). The questions consisting of each domain are presented in table 2. The total MBS, work-related MBS, person related MBS and physical intimidation-related MBS were 2.5±0.7, 2.9±0.8, 2.4±0.8 and 2.1±0.7, respectively.
Table 2. Frequency and percentage of the residents experiencing negative behaviors over the last 6 months (NAQ-R)
|
Negative behavior |
Never (frequency/percent) |
Rarely (frequency/percent) |
Sometimes (frequency/percent) |
Frequently (frequency/percent) |
|
Having your opinions and views ignored |
52 (20.5%) |
78 (30.7%) |
83 (32.7%) |
41 (16.1%) |
|
Being exposed to an unmanageable workload |
28 (11%) |
30 (11.8%) |
64 (25.2%) |
132 (52%) |
|
Someone withholding information which affects your performance |
29 (11.4%) |
62 (24.4%) |
109 (42.9%) |
54 (21.3%) |
|
Being ordered to do work below your level of competence |
18 (7.1%) |
34 (13.4%) |
79 (31.1%) |
123 (48.4%) |
|
Being given tasks with unreasonable or impossible targets or deadlines |
29 (11.4%) |
50 (19.7%) |
83 (32.7%) |
92 (36.2%) |
|
Being humiliated or ridiculed in connection with your work |
23 (9.1%) |
71 (28%) |
92 (36.2%) |
68 (26.8%) |
|
Having key areas of responsibility removed or replaced with more trivial or unpleasant tasks |
35 (13.8%) |
43 (16.9%) |
77 (30.3%) |
99 (39%) |
|
Being ignored or facing a hostile reaction when you approach |
68 (26.8%) |
84 (33.1%) |
76 (29.9%) |
26 (10.2%) |
|
Being shouted at or being the target of spontaneous anger (or rage) |
31 (12.2%) |
55 (21.7%) |
99 (39%) |
69 (27.2%) |
|
Spreading of gossip and rumors about you |
69 (27.2%) |
54 (21.3%) |
78 (30.7%) |
53 (20.9%) |
|
Being ignored or excluded |
63 (24.8%) |
65 (25.6%) |
78 (30.7%) |
48 (18.9%) |
|
Repeated reminders of your errors or mistakes |
49 (19.3%) |
64 (25.2%) |
81 (31.9%) |
60 (23.6%) |
|
Pressure not to claim something which by right you are entitled to (e.g., sick leave, holiday entitlement, travel expenses) |
45 (17.7%) |
42 (16.5%) |
57 (22.4%) |
110 (43.3%) |
|
Persistent criticism of your work and effort |
50 (19.7%) |
83 (32.7%) |
76 (29.9%) |
45 (17.7%) |
|
Excessive monitoring of your work |
36 (14.2%) |
72 (28.3%) |
77 (30.3%) |
69 (27.2%) |
|
Having insulting or offensive remarks made about your person (i.e., habits and background), your attitudes or your private life |
80 (31.5%) |
59 (23.2%) |
62 (24.4%) |
53 (20.9%) |
|
Having allegations made against you |
93 (36.6%) |
57 (22.4%) |
71 (28%) |
33 (13%) |
|
Intimidating behavior such as finger-pointing, invasion of personal space, shoving, blocking/ barring the way |
100 (39.4%) |
57 (22.4%) |
58 (22.8%) |
39 (15.4%) |
|
Being the subject of excessive teasing and sarcasm |
83 (32.7%) |
67 (26.4%) |
62 (24.4%) |
42 (16.5%) |
|
Hints or signals from others that you should quit your job |
119 (46.9%) |
53 (20.9%) |
45 (17.7%) |
37 (14.6%) |
|
Practical jokes carried out by people you don’t get on with |
86 (33.9%) |
80 (31.5%) |
59 (23.2%) |
29 (11.4%) |
|
Threats of violence or physical abuse or actual abuse |
203 (79.9%) |
31 (12.2%) |
13 (5.1%) |
7 (2.8%) |
There was no significant difference between the total MBS, work-related MBS, person related MBS and physical intimidation-related MBS in terms of the number of years of training, the residents’ gender and underlying diseases. However, a significant difference was achieved between total MBS, work-related MBS, person related MBS and physical intimidation-related MBS between residents who worked in the operation room and those who did not (Table 3).
Table 3. Comparison of total MBS, work-related MBS, person related MBS and physical intimidation-related MBS in terms of the number of years of training, the residents’ gender, underlying illness and working site
|
|
Work-related MBS |
Person-related MBS |
Physical intimidation-related MBS |
Total MBS |
|
|
Gender |
NS |
NS |
NS |
NS |
|
|
|
Male Female |
2.78±0.73 2.94±0.76 |
2.37±0.79 2.42±0.81 |
2.07±0.73 2.10±0.76 |
2.47±0.74 2.53±0.73 |
|
Residency year |
NS |
NS |
NS |
NS |
|
|
|
1st 2nd 3rd 4th
|
2.79±1.94 2.99±0.75 2.85±0.78 2.86±0.78 |
2.31±0.80 2.57±0.80 2.37±0.83 2.31±0.77 |
1.94±0.74 2.23±0.72 2.05±0.81 2.08±0.72 |
2.40±0.72 2.66±0.73 2.46±0.75 2.45±0.71 |
|
Working site |
p: 0.008 |
p: 0.000 |
p: 0.004 |
p: 0.001 |
|
|
|
In the operation room Outside the operation room |
3.02±0.68 2.76±0.84 |
2.61±0.76 2.22±0.80 |
2.24±0.77 1.96±0.71 |
2.67±0.68 2.36±0.75 |
|
Past medical history |
NS |
NS |
NS |
NS |
|
|
|
Physical or psychological illness None |
2.60±0.76 2.90±0.78 |
2.26±0.85 2.41±0.80 |
2.02±0.79 2.09±0.75 |
2.39±0.74 2.51±0.74 |
NS: non-significant, p: p-value, Mean Bullying Score (MBS).
In the final step, we assessed the impact of bullying behaviors by two different strategies; at first, we asked a question about each resident’s thoughts and ideas regarding bullying in their medical workplace. Second, we used the GHQ-12 as a measure of the current mental health status of the residents. Accordingly, 110 responders (43%) had considered educational dropout, 9 residents had suicidal ideas and other 9 had thoughts about beating or killing the person who was the source of bullying.
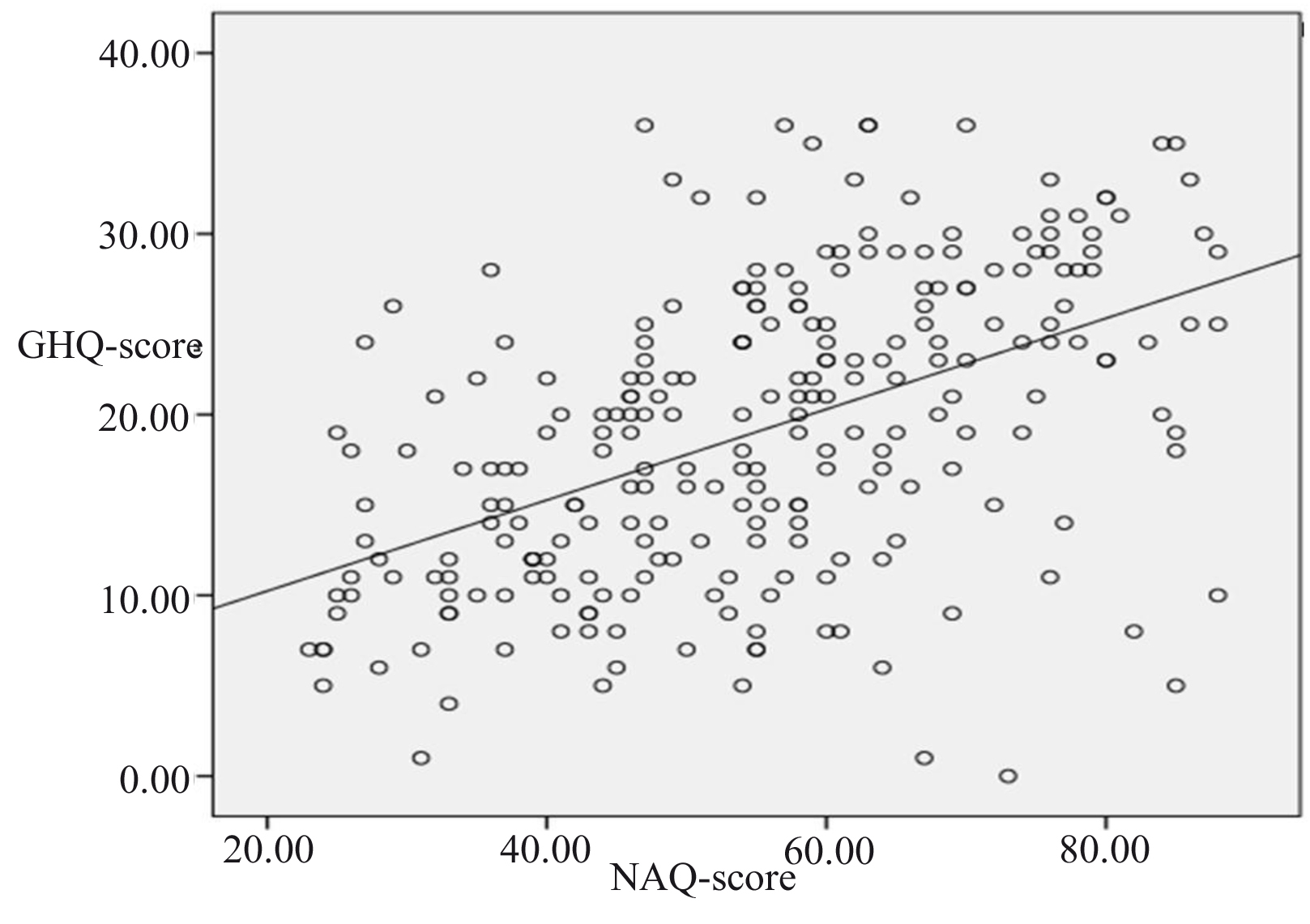
For analyzing the GHQ-12, 3.7 and 14.5 were utilized as cut-off values in the bimodal and Likert scoring methods. Based on the bimodal and Likert scoring, 175 (68.9%) and 171 (67.3%) residents achieved a high score, indicating that they were experiencing symptoms of psychological distress. In addition, Pearson’s correlation coefficient showed a significant positive correlation between the GHQ score and the NAQ-R score assays (r=0.496 and p=0.000) (Figure 2).
Discussion
The present study showed that 95% of the participants had experienced negative behaviors once or more during the last six months, whereas 91% of the responders had witnessed negative act behaviors during this time. At least one instance of intimidation, harassment, and discrimination during residency was reported by 78.2% of the Canadian residents in 2018 according to national surveys conducted by Resident Doctors of Canada (10). Karim and Ducherer in a review article in 2014 stated that 45% to 93% of residents in different countries experience intimidation and harassment in at least one occasion during their residency (11). In another review and meta-analysis by Fnais et al, 63.4% of the residents had experienced mistreatment during their residency period (12). The various reported prevalence of bullying in different studies is not compatible due to the different methods used in these studies. The high rate of negative act behaviors achieved in our study is an indicator of the inappropriate atmosphere in our resident training centers; however, these results should be interpreted with caution as we measured the frequency of negative behaviors (even once) in this study, whereas bullying is defined by the continuity of negative behaviors. In other words, the frequency of negative behaviors was 95% in the current study, and not bullying.
According to our results, the frequency of negative behaviors was not significantly different between male and female participants. However, in some studies the risk of negative behaviors was reported higher among females (26,27). Nevertheless, this equality in negative behaviors in the two genders could be justified by the high number of female residents in our hospitals.
Moreover, based on our findings, the prevalence of negative acts significantly differed between various residency fields and residents who mostly worked in the operation room suffered from higher rates of negative behaviors in comparison to residents who solely worked in the wards. This result is consistent with that of the Royal Australasian College of Surgeons in 2015, which reported a higher rate of bullying among surgical trainees (28). Maybe this could also be understandable by the lens of social learning theory (29). According to this theory, interpersonal interactions in the workplace could change our mode of behavior (30), indicating that negative behaviors could be contagious between residents of the operating room. On the other hand, unquarried surgery specific behaviors (31) and stressful workplace lead to high prevalence of negative act behaviors in the operating room.
We also found that the frequency of negative behaviors was equal between different residency levels. Interestingly, the main source of negative behaviors was senior residents who had experienced the same behavior when they were at junior level. It seems that such behaviors are contagious and could be further explained by the social learning theory (29). Based on this theory, learning occurs through intersection of engagement with others as well as during engagement in daily activities in our workplace (32,33). Therefore, in many studies senior levels were reported as the main source of bullying and negative behaviors (34,35). From another aspect, in the residency system each fault has a punishment, and in some cases the junior residents prefer bullying instead of being punished officially.
In the current study, the GHQ score was higher in patients with a higher NAG score, indicating that negative behaviors could be related to negative mental health outcomes. A systematic review by Szubert et al reported that intimidation, harassment, and discrimination can cause psychiatric sequel and can increase the risk of anxiety disorders, sleep disorders and suicidal attempts by 3 to 16 folds (36). In another study, sexual harassment was associated with impaired mental health (37). We think there is an egg and chicken theory here since impaired mental health status negatively affects communication with colleagues and ultimately the culture of the medical profession. Although, impaired mental health and poor communication skills are not reasonable causes to deserve bullying, impaired communicational skills can predispose an individual to bullying and harassment (38).
Conclusion
This study, as the first study on the prevalence of bullying and negative acts in Iranian medical residents, showed that the medical education atmosphere in residency is not optimal. Therefore, there is a need for certain interventions in the medical education environment.
Ethics approval
The study protocol was approved by the Ethics Committee of Iran University of Medical Sciences (IR.IUMS.REC.1399.1273).
Consent for publication
Not applicable.
Availability of data and material
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Funding
The research was supported by Education Development Center of Iran University of Medical Sciences (grant number: 99-1-10-17691).
Acknowledgements
We wish to acknowledge Firoozgar Clinical Research Development Center (FCRDC), Iran University of Medical Sciences for supporting in the data collection and analysis.
Conflict of Interest
The authors have no competing interests.