Document Type : Original article
Abstract
Background: Sacroiliac Joint (SIJ) dysfunction, a common etiology of Low Back Pain (LBP), is a challenging diagnosis. There is controversy over the efficacy of prolotherapy and corticosteroid injections in relieving SIJ dysfunction. Inconsistent success rates reported in previous studies can be due to heterogeneity in selecting the patients and procedures between studies. This study was conducted to compare the efficacy of local injection of dextrose prolotherapy and corticosteroid in treating the SIJ dysfunction.
Methods: This 36-week, double-blind, Randomized Controlled Trial (RCT) included 40 patients with SIJ dysfunction. The clinical impression was confirmed by the use of a diagnostic injection of local anesthetic inside SIJ. Participants received a single injection of either hypertonic dextrose solution or triamcinolone under Ultrasound (US) guidance. The primary outcome measurement tools, including the Visual Analog Scale (VAS) for pain and the Dallas Pain Questionnaire (DPQ), were evaluated initially and after 2, 8, and 36 weeks.
Results: In both prolotherapy and corticosteroid groups, VAS significantly declined within 36-weeks of follow-up. However, there was no remarkable difference between the two groups at any follow-up timepoints. Similarly, DPQ revealed a remarkable improvement in the corticosteroid group while it did not show any meaningful change in the prolotherapy group.
Conclusion: Both local injections of dextrose and corticosteroids can successfully reduce pain in patients with SIJ dysfunction without significant superiority between the two treatments. However, corticosteroid injection was slightly more effective in terms of improvement of functional status. Further investigations are required to extend these results to SIJ dysfunction treatment more reliably.
Keywords: Intra-articular injections, Low back pain, Prolotherapy
Introduction
The Sacroiliac Joint (SIJ) is a frequent source of discomfort for people suffering from Low Back Pain (LBP). SIJ pain has been found to affect up to 75% of people during their lifetime (1). Due to many potential causes, the etiology of LBP is often uncertain, even after extensive clinical and radiographic assessment. Degenerative disc disease, facet arthropathy, ligamentous hypertrophy, muscular spasm, hip arthropathy, and SIJ dysfunction are all potential sources of pain, and a precise clinical and radiological connection is not always attainable (2). The lack of specificity in existing diagnostic methods adds to the challenge (3). SIJ dysfunction is characterized as hyper or hypomobility of the joint, as well as a misalignment or change in position of the sacrum and ilium bones. SIJ dysfunction is often treated by realigning the hypomobile joints via compression, traction, manipulation, mobilization, gliding, and strengthening the surrounding muscles of the hypermobile joints (4). Physical exercise, sacroiliac belts, physiotherapy, manual manipulations, and anti-inflammatory drugs are all options for early nonoperative care of SIJ dysfunction. The efficacy of these treatments varies, and analgesics often do not substantially alleviate this kind of pain (3).
For patients who do not respond adequately, minimally invasive interventions may be beneficial, among which local corticosteroid injection is highly effective. However, some studies have shown its efficacy only for a short period (5,6). Hypertonic dextrose prolotherapy has been increasingly used to treat various types of soft tissue disorders such as chronic LBP, myofascial pain syndrome, etc (7).this method aims to produce dense fibrous tissue to strengthen ligament and joint capsules by inducing proliferation. It was first introduced in 1930 to treat spinal pain disorders, and after that, various techniques have been described for different parts of the body (8).
Due to the complex structure of the SIJ, landmark-guided injections have a low accuracy rate and are quite unreliable; only 22 percent of these injections have reached the articular space (9). Recently, some researchers have used Ultrasound (US) guidance. It has been shown that this inexpensive and real-time modality could be considered as a suitable imaging technique for in-depth musculoskeletal injection guidance (10,11). The objective of this study was to compare the efficacy of dextrose prolotherapy with corticosteroid injections in the treatment of SIJ dysfunction.
Materials and Methods
Design and population
This randomized, double-blind, single-center clinical trial included 130 patients referred to Firoozgar Hospital’s Physical Medicine and Rehabilitation (PM&R) clinic affiliated with Tehran University of Medical Sciences (TUMS) from September 2016 to February 2017. Based on the mean and standard deviations in both groups and according to values of alpha=”0.05, beta=”0.20, the final amount of 36 patients was considered adequate for this study. This study was in line with the Helsinki Declarations and their subsequent revisions (12). The study was also approved by our institutional ethics committee, which approved it with the following number: IR.IUMS.FMD.REC.1396.9411524009. Patients signed an informed consent form after being given a thorough explanation of the study’s procedures and goals. Patients were informed of their right to withdraw from the study without affecting their treatment plan.
In addition, the study protocol has been registered under No. IRCT20170910036107N2 in the national RCT database, accessible at www.irct.ir.
Participants
The primary diagnosis of the patients was based on at least two months of unilateral typical hip, thigh, and groin pain. Patients were included in the study if they had not responded to pharmacological treatments for at least one month. Tenderness below the Posterior Superior Iliac Spine (PSIS) and at least one positive Patrick or Gaenslen test were consistent clinical examinations in favor of a SI origin pathology (13) Given that these tests are not specific (3), a significant reduction in pain (greater than 50% of the baseline level) immediately following an anesthetic injection (2 ml of bupivacaine 2.5%), measured at 100 mm Visual Analog Scale (VAS), was considered a confirmatory tool for the diagnosis of SIJ dysfunction.
Our exclusion criteria were history of surgery, trauma, or any invasive procedure in the lumbosacral region during the past 6 months, and abnormal complete blood count or impaired coagulation tests. Pregnant women, patients on immunosuppressive medications, and those with an underlying systemic inflammatory disease were also excluded. Furthermore, patients with a history of infections, fibromyalgia, cancer, or concurrent lumbosacral radiculopathy were excluded.
Randomization, concealment, allocation, and blinding
After gathering demographic information such as age, gender, occupation, and chronic pain assessment, patients were randomly assigned to one of the two injection groups (in a 1-1 ratio using a computer-generated code): corticosteroid or dextrose water injection. The participants and the assessor physicians were kept in the dark about the groups to which they were assigned. An operator was employed for preparing the injection syringes. The appearances of corticosteroid and dextrose syringes were identical and were covered with Aluminum foil. The patients were unaware of the type of treatment they were receiving, and the assessor physicians were unaware as well. Also, at follow-ups, the assessors were unaware of which group the patient belonged to.
Intervention
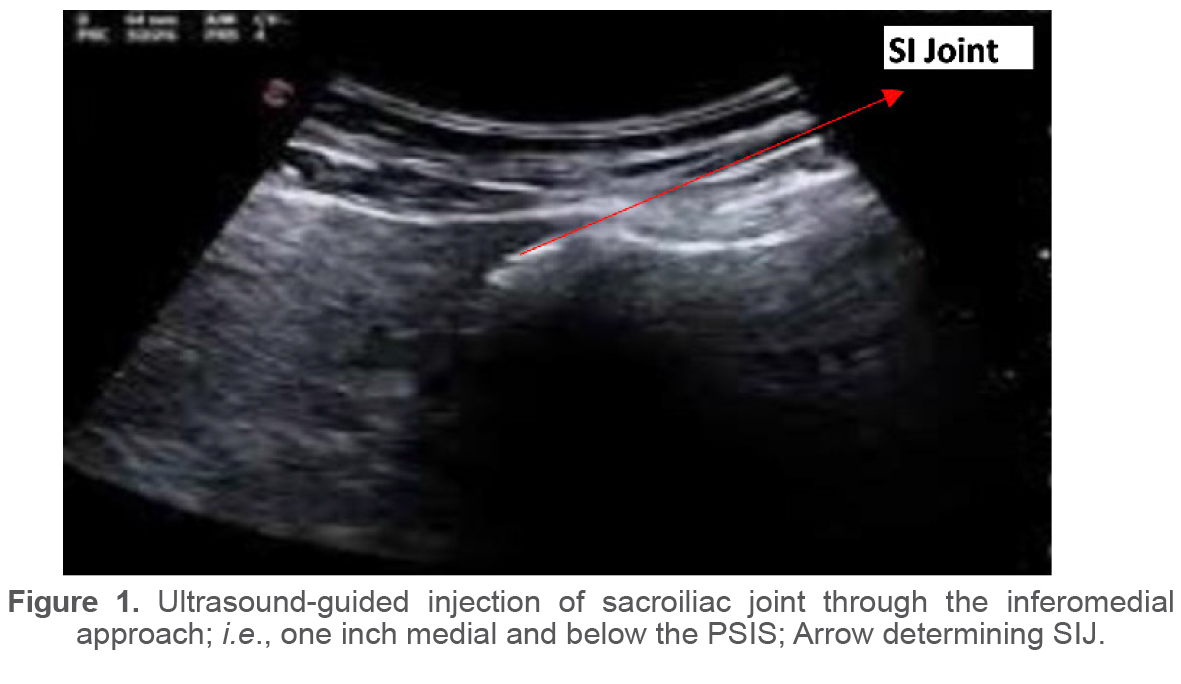
For US guidance, the transducer was positioned transverse to the sacral hiatus (sacral cornea) and then moved slightly lateral to reach the sacrum’s outer edge until the joint appeared in the US field (in-plane method). The treatment groups in this survey were unknown to the patients, the assessor physician, and the physician who performed the injections. The syringes used looked identical and were wrapped in an aluminum envelope. All injections were performed under sterile conditions by a PM&R specialist with 10 years of experience in musculoskeletal injections using the spinal needle Gauge 22 through an inferomedial approach, i.e, one inch medial and below the PSIS (Figure 1). Initially, each patient received 2 ml of 2.5% bupivacaine intra-articular injection as a confirmatory test for SIJ dysfunction. 2.5 ml of dextrose 20% solution was injected into the prolotherapy group, while 2.5 ml of triamcinolone 40 mg/ml was injected into the steroid group. A program of stretching exercises and Acetaminophen consumption was recommended to control potential post-injection reactions.
Outcome measurements
Patients were reassessed after 2, 8, and 36 weeks using the VAS score and Dallas Pain Questionnaire (DPQ). The VAS score is a method for assessing the severity of pain experienced by patients. It comprises a 100-mm-long line with a grinning face image on the left side representing no pain and a frowning face image on the right side representing the worst pain ever (14). This measuring tool was tested in three different positions: lying down, standing up, and sitting.
The DPQ was created to assess how much chronic pain affects four aspects of patients’ lives: daily activities, anxiety/depression, work/leisure activities, and social interest. This scale consists of 16 questions to which our patients can respond using a scale similar to the VAS (15). The DPQ was not assessed at the last follow-up time point.
Statistical analysis
Finally, the data were analyzed using IBM SPSS Statistics for Windows, version 22 (IBM Corp., Armonk, N.Y., USA). The baseline data normality was evaluated utilizing the Kolmogorov-Smirnov test. The Chi-square method was used for the qualitative variables, independent samples t-test, and ANOVA for quantitative parameters. VAS and DPQ scores between the two groups of the trial during the study course were compared with the General Linear Model (GLM) analysis of the repeated measures (Greenhouse–Geisser corrected in case of non-sphericity). p values below 0.05 were considered statistically significant.
Table 1. Demographic characteristics and baseline variables of participants by their treatment group
|
Characteristics |
Prolotherapy |
Corticosteroid |
p-value |
|
Number of Participants |
18 |
18 |
- |
|
Age, Mean (SD) [year] |
50.72 (7.3) |
52.44 (7.6) |
0.49 |
|
Gender, (Female: Male ratio) |
13:5 |
12:6 |
0.28 |
|
VAS score, Mean (SD) |
81.7 (15.0) |
77.6 (17.1) |
0.44 |
|
Dallas subscale 1 (Daily activities) , Mean (SD) |
60.50 (16.6) |
58.83 (16.5) |
0.76 |
|
Dallas subscale-2 (Work and leisure), Mean (SD) |
61.39 (25.4) |
57.78 (26.5) |
0.68 |
|
Dallas subscale-3 (Social interest), Mean (SD) |
51.00 (25.3) |
48.33 (19.0) |
0.72 |
|
Dallas subscale-4 (Anxiety/depression), Mean (SD) |
45.00 (21.5) |
43.61 (23.8) |
0.85 |
|
Dallas Total, Mean (SD) |
217.8 (29.5) |
208.5 (28.7) |
0.34 |
Table 2. Between group analysis of outcome measures by treatment groups
|
|
Before intervention |
After 2 weeks |
After 8 weeks |
After 9 months |
||
|
VAS, mean (std. Deviation) |
||||||
|
Prolotherapy group |
8.17(1.54) |
4.50(2.12) A |
4.11(1.45) A |
2.67(1.24) A |
||
|
Corticosteroid group |
7.76(1.70) |
3.71(2.12) A |
4.48(2.60) A |
2.62(1.63) A |
||
|
Dallas score total, MEAN (Std. Deviation) |
||||||
|
Prolotherapy group |
217.89(72.87) |
182.94(84.62) A |
195.83(47.41) A |
|
||
|
Corticosteroid group |
208.56(70.69) |
165.54(62.12) A |
158.83(78.81) A |
|
||
A: no statistical significance between prolotherapy and corticosteroid groups.
Table 3. The intra-group analysis by treatment group and interaction effects of time and group on outcome measures
|
VAS, mean (Std. Deviation) |
|||
|
|
After 2 weeks, compared to baseline |
After 8 weeks, compared to baseline |
After 9 months, compared to baseline |
|
Prolotherapy group |
3.67(0.56) B |
4.06(0.59) B |
5.50(0.51) B |
|
Corticosteroid group |
4.05(0.51) B |
3.29(0.54) B |
5.14(0.48) B |
|
Dallas score total, mean (Std. Deviation) |
|||
|
|
After 2 weeks, compared to baseline |
After 8 weeks, compared to baseline |
|
|
Prolotherapy group |
34.94(24.68) A |
22.06(18.12) A |
|
|
Corticosteroid group |
43.00(14.02) B |
49.72(17.44) B |
|
|
VAS, mean (Std. Deviation) |
|||
|
|
After 8 weeks, compared to 2 weeks |
After 9 months, compared to 2 weeks |
After 9 months, compared to 8 weeks |
|
Prolotherapy group |
0.39(0.45) A |
1.83(0.39) B |
1.44(0.25) B |
|
Corticosteroid group |
-0.76(0.41) A |
1.10(0.36) B |
1.86(0.24) B |
|
Dallas score total, mean (Std. Deviation)
|
|||
|
|
After 8 weeks, compared to 2 weeks |
|
|
|
Prolotherapy group |
-12.89(12.31) A |
|
|
|
Corticosteroid group |
6.72(12.31) A |
|
|
|
Overall interaction effects of time and group between two treatment groups (p-value) |
|||
|
VAS |
|
Dallas |
|
|
0.316 |
|
0.386 |
|
A: No statistical significance (p-Value > 0.05)
B: Statistical significance (p-Value ≤ 0.05)
Results
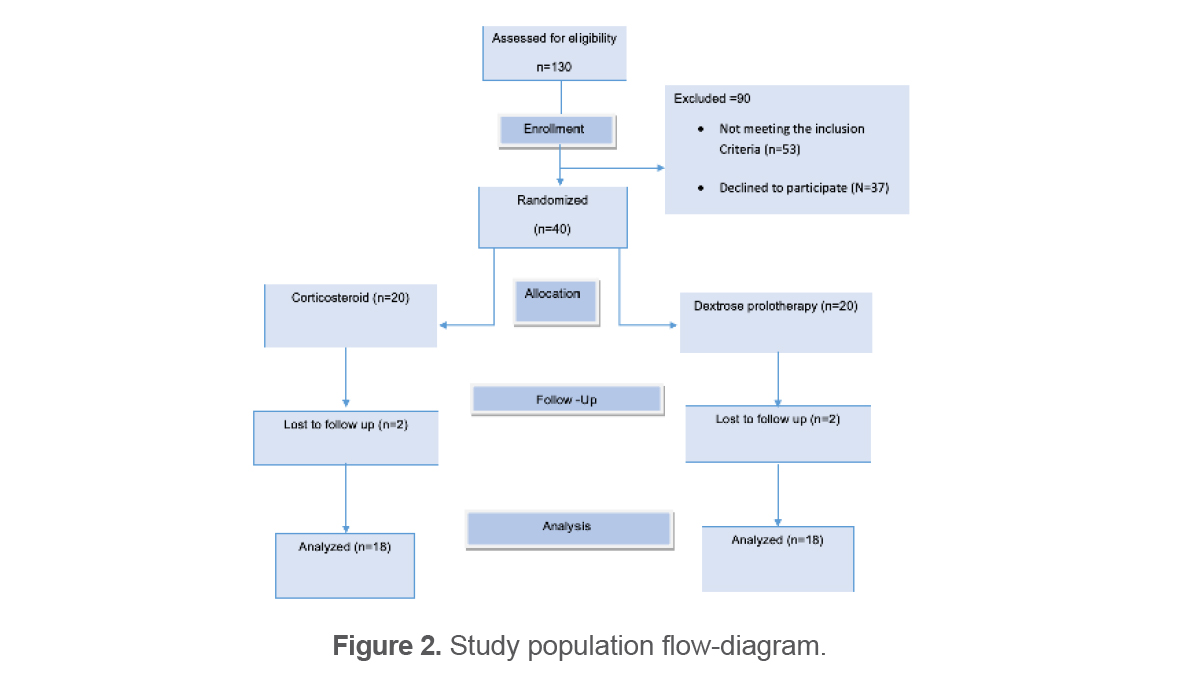
Out of 130 patients assessed for the trial’s eligibility, 40 patients met the inclusion criteria and accepted participation in this study. They were randomized into two groups of the trial and received either Corticosteroid (n=20) or Dextrose (n=20) injection. 36 patients completed the trial as two subjects from each group withdrew from the study due to personal affairs (Figure 2). None of them were dropped due to complications or injection-related adverse events. All the variables were distributed normally based on the Kolmogorov-Smirnov test. Detailed baseline characteristics of the participants (including age, gender, etc.) are shown in table 1. None of the baseline characteristics was significantly different between treatment groups (p-value >0.05). Additionally, none of the clinical variables before injection (VAS and DPQ) showed a significant difference between the two arms of the study (Table 1).
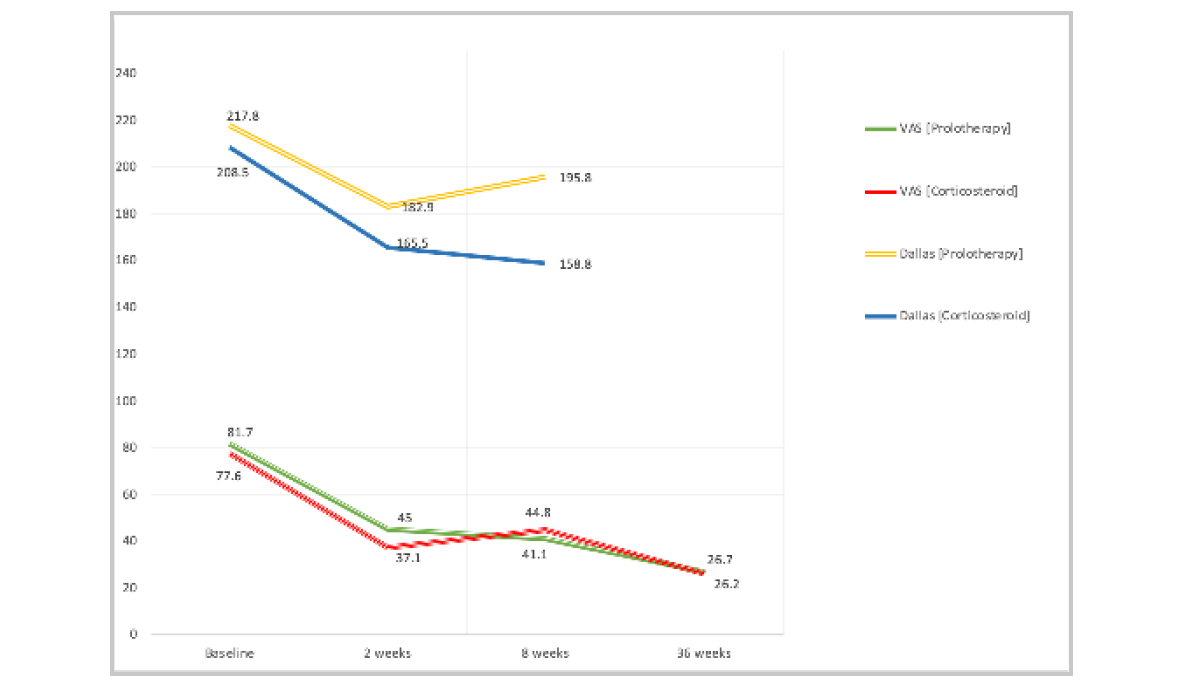
In figure 3, the therapeutic trajectory of dextrose and steroid interventions within the two groups has been depicted. Although we detected a remarkable improvement within the two groups, there was no significant superiority between the two interventions at neither follow-up time points (Table 2). Within the dextrose prolotherapy group, a significant improvement was observed in VAS at the 2nd-week visit, and this improvement remained significant after 8 and 36 weeks compared to the baseline value (Table 3). Similarly, in the steroid group, a significant improvement was observed at all intervals, compared to the baseline value. In contrast, there was no remarkable additional improvement after the 2nd-week visit within neither of the two groups. Exceptionally, during the interval between 2 and 8-week follow-up, a borderline significant change within both groups was detected (Table 3).
DPQ was assessed only through the initial 8 weeks of intervention; it showed quite a different manner. The improvement at both the 2-week and 8-week visits compared to baseline was significant only for the steroid group. In comparison, this improvement was not statistically significant within the parallel group (Table 3). However, it should be kept in mind that data analysis revealed no significant superiority between the two groups (Table 2). As a common finding, the maximum amount of change in both groups was found in daily and occupational activities, much larger than the other two subscales, i.e, anxiety/depression subscale and social interest domain.
To sum up, the patients reported pain and functional status improved in both dextrose and steroid groups during this study. This improvement was detected mainly within the first two weeks, and after that, all trend-lines declined in VAS and even reversed in DPQ (Figure 3). This improvement was more remarkable in the corticosteroid group (52% for VAS and 20% for DPQ) than the dextrose prolotherapy injection (52 vs. 45% in VAS; 20 vs. 16% in DPQ, respectively). There was, however, no remarkable superiority between the two interventions. Furthermore, all of the interaction effects of time and group between two treatment groups were statistically insignificant (p-value >0.05).
The only adverse reaction observed in patients was a mild flare reaction after the injection (three participants in the corticosteroid group and three in the dextrose water group), which was not statistically significant between the two groups (p-value >0.05).
Discussion
In this study, we compared two treatment groups of corticosteroid injection and prolotherapy. US guidance was utilized for a confirmed diagnosis of sacroiliac joint pain since the ability to diagnose the SIJ as the primary pain generator on patients’ history and physical examination is not absolute (16–18). US guidance also had an essential role in the accuracy of injections in both treatment groups. A meaningful cut-off value for VAS was a patient score improvement of more than 30 mm. In the case of DPI, a cut-off value of 25 points was considered significant. Our results showed that the VAS score of the patients significantly decreased in both groups in 2-week and 8-week follow-up time points and remained significant even after 36 weeks compared to the baseline characteristics. Also, the current study indicated that there was no significant difference between the treatment groups. But the DPQ was evaluated only in 2-week and 8-week follow-up time points and only showed significant improvement in the score of the corticosteroid group. Also, with respect to the reported side effects, both treatment options were well-tolerated, similar, and safe. Since patients were randomly assigned to the treatment arms and baseline characteristics were not significantly different, the improved VAS score and DPQ can be attributed to the beneficial effects of the injections.
There is debate regarding the effectiveness of ligament prolotherapy in symptom relief of sacroiliac joint dysfunction. Previous studies’ incoherent treatment outcomes could be attributed to differences in patient selection methods used between studies (10). Nowadays, a great deal of attention has been paid to the clinical use of regenerative drugs, particularly in the field of musculoskeletal medicine. It is trusted that such treatment will anticipate utilitarian decays, reestablish power, and upgrade musculoskeletal steadiness by reinforcing ligament, muscles, and tendons. Prolotherapy has been proposed as an injection-based complementary therapy for multiple musculoskeletal diseases. Prolotherapy has been recommended for the treatment of lower back pain for many years. Yet, its reported results have not been constant. According to a major, well-conducted randomized controlled study, prolotherapy was not any better than normal saline solution injection (19). Dextrose, as the current agent, is applied in prolotherapy. The solution injected (hypertonic dextrose) was easily obtainable and a common solution for prolotherapy injections. Injectable corticosteroids are also used in other inflammatory and non-inflammatory musculoskeletal disorders, such as tendinitis, arthritis, tenosynovitis, and other musculoskeletal complaints.
Other potential mechanisms for pain reduction include decreased prostaglandin and leukotriene synthesis, modulation of peripheral nociceptor neurons, direct membrane stabilization mechanism, and modulation of spinal cord dorsal horn cells. They might even have a mild anesthetic effect (16).
In a study conducted by Kim et al (10), VAS decreased more than 50% after the SIJ injection under fluoroscopy in both Prolotherapy and corticosteroid groups. At 2-week follow-up, the amount of pain reduction in both groups was slightly higher than in the current study, which could be attributed to patient selection. At six months, the long-term follow-up of that study revealed a significant reduction in pain in the Prolotherapy group, more than in the corticosteroid group. The recent finding was inconsistent with our findings; our data revealed that pain relief was not statistically different in both groups after 36 weeks of follow-up.
In addition, Lee et al (8) found that three consecutive weekly injections of dextrose in the SIJ resulted in an 80% pain reduction, based on VAS, within the first month, which was far greater than our study finding (40% pain improvement at the first visit, from 81-mm to 45-mm). This higher reduction could be due to the multiple injections of dextrose in that study. In another study, Cusi et al (19) evaluated the effectiveness of dextrose 50% in participants with SIJ dysfunction. Within three months of the injection, they discovered that patients experienced moderate pain relief (approximately a 45-mm reduction on a 100-point scale). It was nearly in line with our findings considering pain improvement after 2 months of prolotherapy (40-mm reduction in VAS). Furthermore, the pain reduction trend persisted in that study until two years of follow-up.
Interestingly, in a Cochrane collaboration report by Yelland et al (7), it was proved that prolotherapy injections alone were not more helpful than control injections. They found that, as compared to controlled injections, Prolotherapy injections alone had no significant impact on sacroiliac joint dysfunction. However, with the assistance of co-interventions, prolotherapy injections were more beneficial than controlled injections, especially when both injections and co-interventions were controlled at the same time (7). Anyway, these findings may be attributed to the lack of a validated diagnosis for patient selection and variations in the proliferant injection techniques. In addition, Hsieh et al (20) found that US-guided prolotherapy was also a safe and effective complementary treatment for acromial enthesopathy and acromioclavicular joint arthropathy.
It is noteworthy that none of the treatment methods had any severe complications related to the injection. This study used the DPQ and the VAS score, which could be expanded in further studies for better comparisons and data pooling. Although this research has many benefits, such as a double-blind design, thorough adjustments for baseline characteristics, and novelty, certain limitations should be addressed to prevent the results from being overgeneralized. For starters, our main limitation in this study was an insufficient sample size. A bigger sample size seems to be required to give a better understanding of the extent of improvement in patient symptoms. Second, we did not investigate the dose-response connection in our research. Third, since SIJ dysfunction is a chronic illness with a complex course, a more extended follow-up period may provide more comprehensive observations.
Conclusion
Local injections of dextrose prolotherapy and corticosteroid can reduce pain in patients with SIJ dysfunction, while both have a minor effect on the patients’ functional score. Future studies with larger sample sizes and more extended follow-up periods could validate these findings.
Disclosure
None of the authors received funding for writing this article. The authors have no financial or non-financial competing interest in this research to disclose, and they are satisfied with the list of names in the article.
Acknowledgements
All authors would like to acknowledge all staff in the Physical Medicine and Rehabilitation (PMR) clinic of Firoozgar Hospital in Tehran.
Conflict of Interest
The authors declare no conflict of interest.