Document Type : Original article
Abstract
Background: Ovarian tumors are mostly detected in advanced stages. Early diagnosis of malignant ovarian germ cell tumors is so vital to keep life and fertility of the patients. We aimed to find out different presentations of malignant ovarian germ cell tumors based on age, parity and histology to help early diagnosis of the tumors.
Methods: In this study, malignant ovarian germ cell tumors admitted in a referral center of gynecology oncology were studied 2001-2018. The symptoms and signs of the patients were collected and analyzed according to age, parity and specific histology.
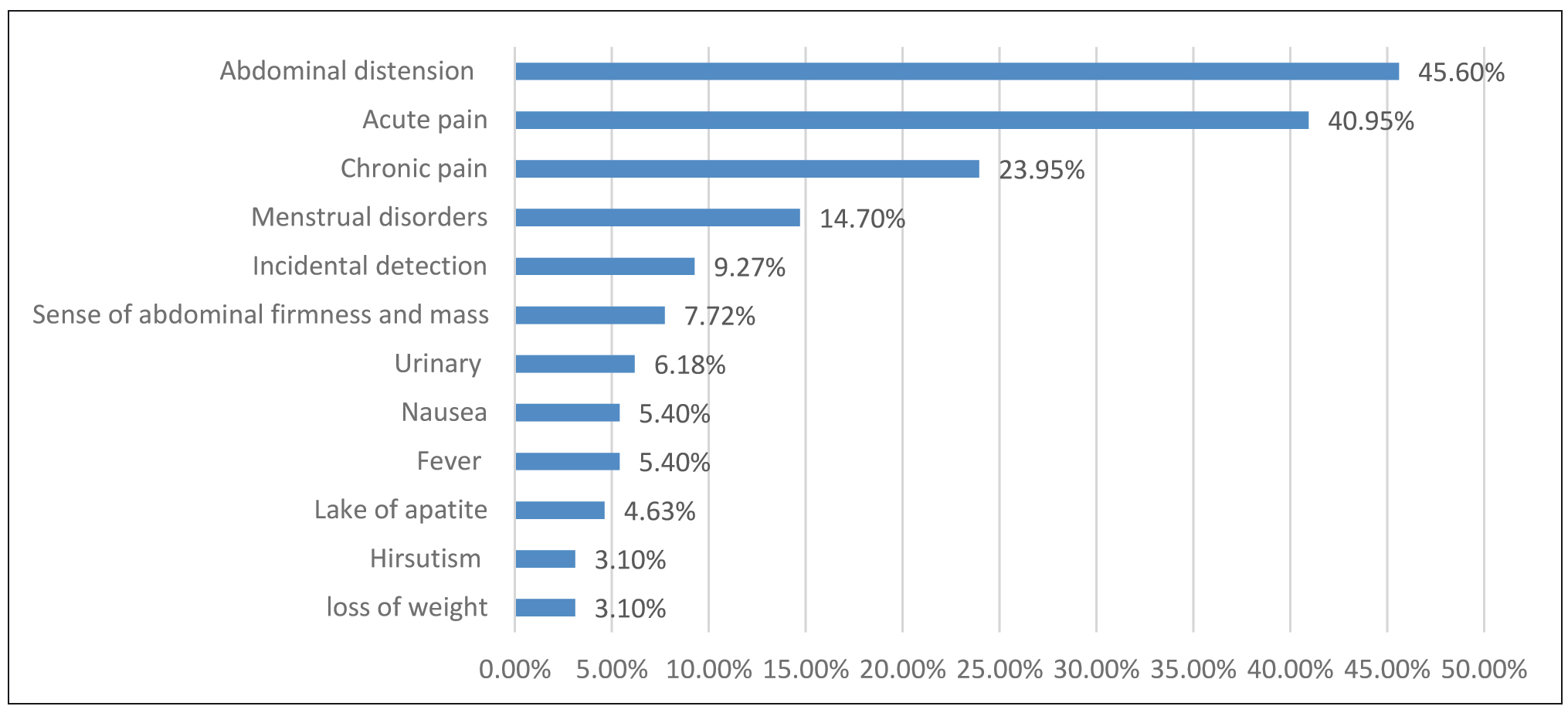
Results: 128 cases of malignant germ cell tumors were detected. The primary symptoms included abdominal distension (45%), acute pain (40.95%), chronic pain (23.95%), menstrual irregularity (14.7%), sense of abdominal firmness and mass (7.72%), nausea (5.4%), fever (5.4%), lack of appetite (4.63%), virilization (3.1%), depletion of weight (3.1%), and 9.27% detected incidentally. Abdominal distension, and acute pain decreased after 24. Menstrual disorders and incidental detection in multiparas were significantly more than nulliparous (p<0.05). Abdominal distension was the prominent sign in dysgerminomas (50%). Almost 45% of immature, yolk sac, and mixed tumors referred with acute abdominal pain. The data showed that 85% of the patients had been suffering from some discomforts for days to months prior to the diagnosis.
Conclusion: The majority of cases are symptomatic for a long time before the first visit although aging and parity can lessen their severity. Late diagnosis can lead to acute abdomen in some histology types. Young women and health providers should be warned about concerned presentations of ovarian tumors.
Keywords: Clinical presentation, Germ cells, Histology, Ovary, Parity
Introduction
Ovarian cancer is the most fatal gynecologic malignancy in women (1,2). The outcome of the affected women largely depends on the stage at the primary visit. Unfortunately, over 70% of these women are diagnosed in the advanced stages, when the tumor has disseminated beyond the pelvis (3). In spite of attempts to find a modality for screening the ovarian cancer, there is no approved model in this regard yet (4). Therefore, recognition of the clinical manifestations is still the sole solution for the primary detection of the tumors.
Malignant Ovarian Germ Cell Tumors (MOGCTs) account for 3% and 15% of the ovarian malignancies in the western and Asian countries, respectively. They commonly affect adolescents and young adults (5-8). Five-year survival of MOGCTs in the early stages is estimated 70-90% while it is 20-30% in the advanced stages (9). Late diagnosis of these tumors can sometimes lead to acute abdomen and emergency laparotomy due to fast overgrowth, rupture or torsion of the affected ovary which in turn can influence the cytoreduction procedures during staging or hurt the ability of fertility in the patient (10,11). Thus, having the right knowledge of the clinical manifestations in these tumors seems very important to avoid urgent situations.
“Whether the ovarian tumors are asymptomatic or the patients do not notice the symptoms” has been argued for decades. Recent reports showed that ovarian cancers are usually symptomatic but the symptoms may be neglected by the patients and/or the caregivers (9-12). Anyway, this delay can advance the stage of the tumor and consequently impact the outcome. In order to detect the disease at the early stages, we aimed to find out the associations between the symptoms of MOGCTs and age, parity and specific histology to help early diagnosis of the tumors.
Materials and Methods
The present study was conducted in Vali-e-Asr Hospital, the main center of gynecology oncology in Tehran, Iran, during 18 years from 2001. After providing the approval of the ethics committee (IR.TUMS JKHC.Rec.1396.4819), and taking the informed consents, the cases of MOGCTs were enrolled in the study and classified according to the histology subtypes. Using a questionnaire containing demographic and obstetric characteristics and related clinical manifestations including abdominal distention, pain, menstrual irregularity, sense of mass, nausea, urinary discomfort, fever, lack of appetite, virilization and weight depletion, the data was collected. Interview with the patients and hospital files were the references of information. The codified data were entered into the SPSS software 24, and the frequency of various symptoms and signs in whole cases and histologic subtypes via descriptive tests and correlation of symptoms with age and parity status via chi-square tests were analyzed. p-value<0.05 was considered significant.
Results
128 cases of MOGCTs were detected. The mean age was 23.88±7.85 years. Demographic data showed that 52% had got married, and 68% were nulliparous (Table 1). Interview with the patients indicated that 85% of the cases had symptoms for days to months prior to the diagnosis. Dysgerminoma and immature teratoma for 3 days to 11 months, mixed tumors for 15 days to 11 months, yolk sac for 7 days to two months and Squamous Cell Carcinoma on teratoma (SCC teratoma) for 4 months were reported by the patients. More than 90% complained of abdominal distension and pain (Figure 1).
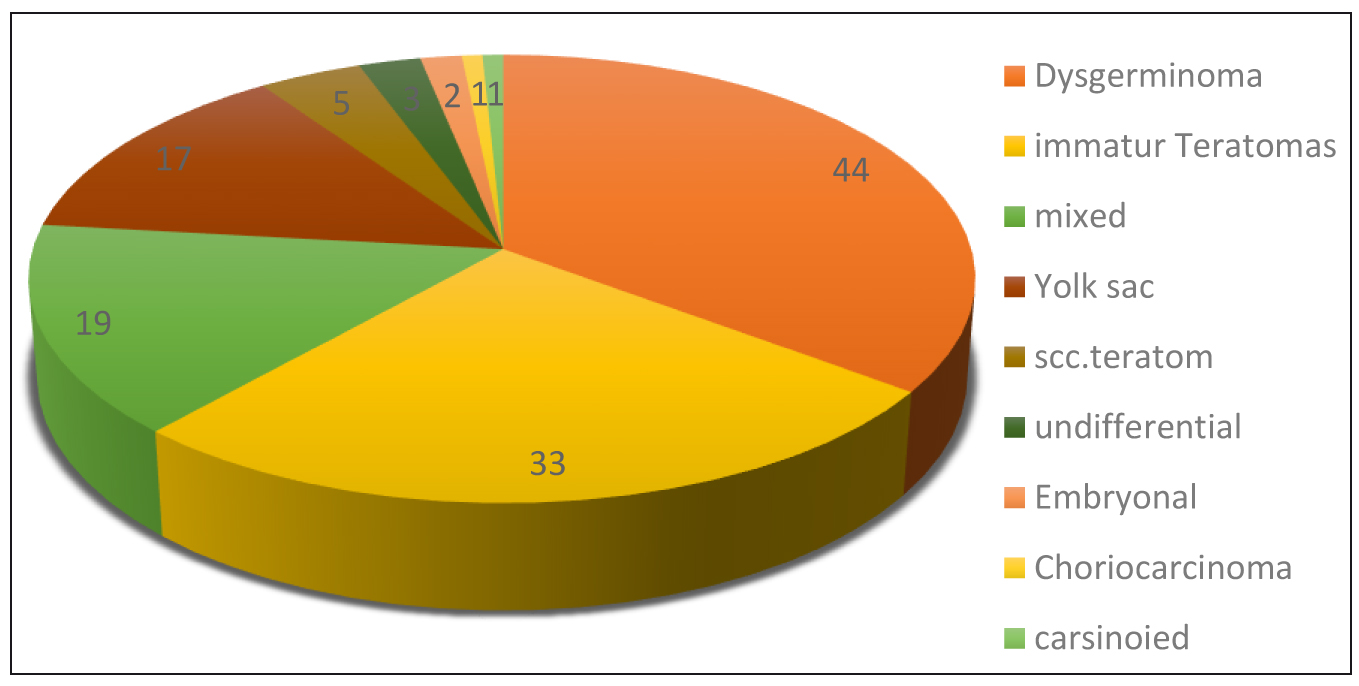
In 22 of the cases, the menstruation had not already been commenced and 5 cases had Dysgenic gonads. The number of para in multipara cases included: 1 para (22), 2(11), 3(4), 5(1) and 6(2). Incidence of subtypes of MOGCTs were dysgerminoma (35.2%), immature teratomas (26.4%), mixed (15.2%), yolk sac (13.6%), SCC teratoma 4%, undifferential (2.4%), embryonal (1.6%), choriocarcinoma (0.8%), and carcinoid (0.8%), respectively.
Table 1. Demographic characteristics of the malignant ovarian germ cell tumors
|
Age |
Min (year) |
11 |
|
Mean (mean ± SD) |
23.99±7.88 |
|
|
Max (year) |
50 |
|
|
Others |
27.6% |
|
|
Education |
Unlettered |
6.3% |
|
Student (school) |
32.8% |
|
|
Diploma or undergraduate |
9/60% |
|
|
Place of living |
Urban |
80% |
|
Rural |
20% |
|
|
Socio-economic status |
Well-off |
15.4% |
|
Medium |
76.9% |
|
|
Poor |
7.7% |
|
|
Body mass index |
Thin (<18.5) |
25% |
|
Normal |
53.6% |
|
|
Overweight (>24.9) |
21.4% |
|
|
Marital Status |
Single |
47.7% |
|
Married |
52.3% |
|
|
Parity |
No parity |
68.8% |
|
Parous |
31.2% |
|
|
Menstruation |
Yes |
106 (82.8%) |
|
No |
22 (17.2%) |
|
|
Menstruation disorders |
Yes |
43 (40.57%) |
|
No |
63 (59.43%) |
|
|
Karyotype (no menstruation- 22 cases) |
Normal gonad (XX) |
17 (77.27) |
|
Dysgenic gonad (XY) |
5 (22.73) |
About 41% referred by acute abdomen, although only 15% had sudden acute pain and 26% stated mild nonspecific symptoms in previous days. 9.27% were asymptomatic and detected incidentally (Figure 2).
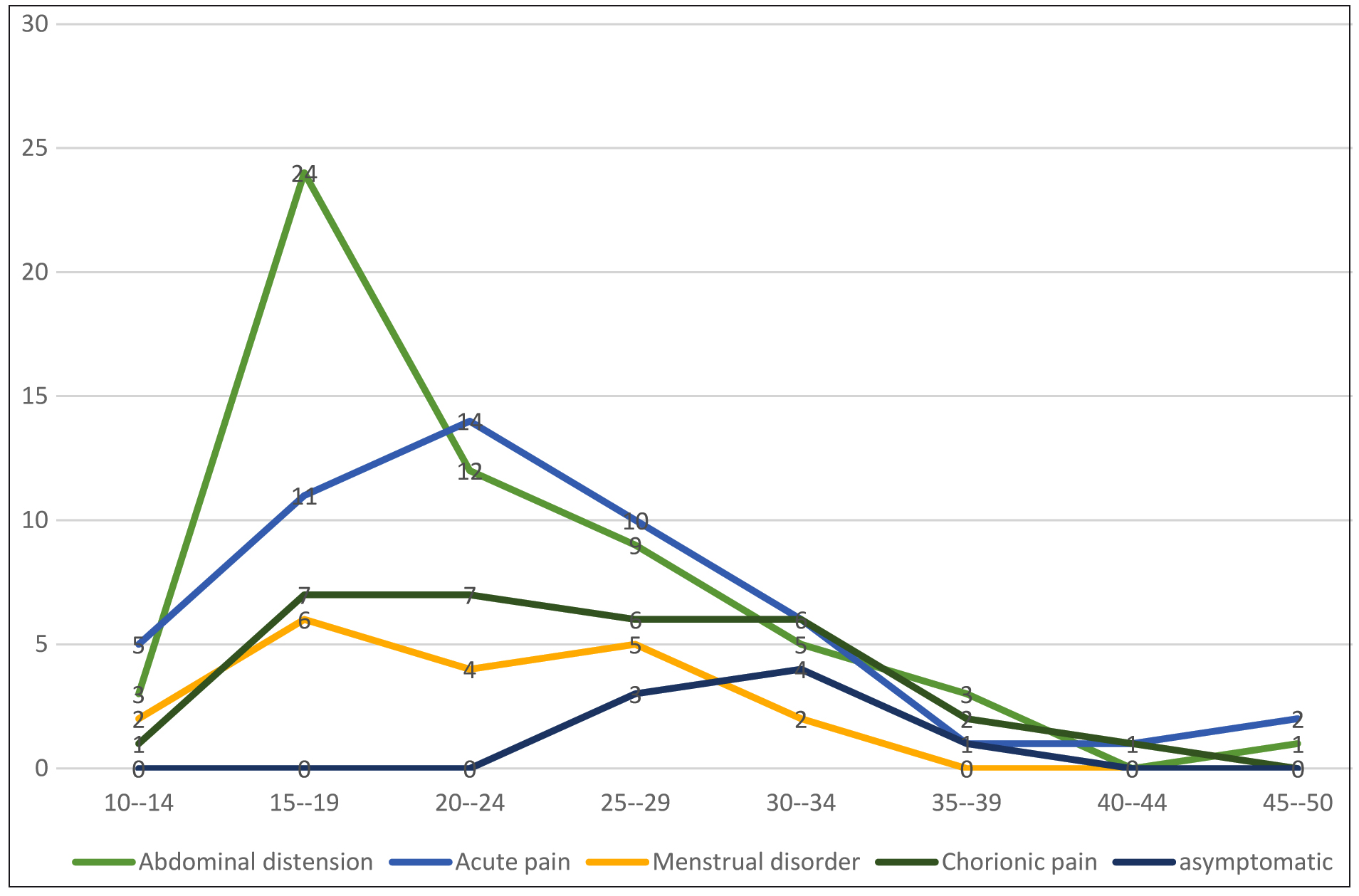
Although abdominal distension, pain and menstrual disorders were the most symptoms in all age groups, their incidence declined after 24 years old, and also asymptomatic cases were increased (Figure 3).
Menstrual disorders and incidental detection in multiparas were significantly more than nulliparous (Table 2).
Abdominal distension and pain were the most common symptoms in all subtypes. Also, dysgerminoma and immature teratoma were the most common types which were detected incidentally. Menstrual disorders and sense of mass were more in dysgerminoma and mixed. The three undifferentiated cases referred only by acute abdomen. Torsion of mass in immature and yolk sac was more and fever was higher in immature and mixed tumors (Table 3).
Table 2. Comparison of the symptoms and signs in multiparas to nulliparous
|
|
Nulliparous |
Multiparas |
p-value |
|
Abdowwminal distension |
43 (48.9%) |
14 (35%) |
0.144* |
|
Acute pain |
34 (38.6%) |
16 (40%) |
0.883* |
|
Chorionic pain |
22 (25%) |
8 (20%) |
0.536* |
|
Menstrual irregularity |
17 (19.3%) |
2 (5%) |
0.035* |
|
Ascites |
10 (11.4%) |
2 (5%) |
0.211** |
|
Sense of abdominal firmness and mass |
9 (10.2%) |
1 (2.5%) |
0.121** |
|
Urinary |
7 (8%) |
1 (2.5%) |
0.223** |
|
Fever |
6 (6.8%) |
1 (2.5%) |
0.296** |
|
Nausea |
6 (6.8%) |
1 (2.5%) |
0.296** |
|
Torsion |
5 (5.7%) |
3 (7.5%) |
0.482** |
|
Lack of appetite |
4 (4.5%) |
2 (5%) |
0.611** |
|
Loss of weight |
4 (4.5%) |
- |
0.219** |
|
Hirsutism |
2 (2.3%) |
2 (5%) |
0.37** |
|
Incidental detection (asymptomatic) |
1 (1.1%) |
7 (%17.5) |
0.001** |
|
Hemoperitoneum |
1 (1.1%) |
1 (2.5%) |
0.529** |
* Chi-square, ** Exact fisher.
Table 3. Frequency of the symptoms and signs according to histology
|
Undifferential |
Mixed |
Squamous Cell Carcinoma on teratoma (SCC teratoma) |
Carcinoid |
Choriocarcinoma |
Embryonal |
Yolk sac |
Immature Teratoma |
Dysgerminoma |
|
|
- |
7 (36.8%) |
3 (60%) |
- |
- |
2 (100%) |
8 (47.1%) |
14 (42.4%) |
22 (50%) |
Abdominal distension |
|
3 (100%) |
8 (42.1%) |
2 (40%) |
- |
1 (100%) |
1 (50%) |
8 (47.1%) |
15 (45.5%) |
11 (25%) |
Acute pain |
|
- |
4 (21.1%) |
2 (40%) |
- |
1 (100%) |
- |
4 (23.5%) |
9 (27.3%) |
9 (20.5%) |
Chronic pain |
|
- |
4 (21.1%) |
- |
- |
- |
- |
1 (5.9%) |
5 (15.2%) |
9 (20.5%) |
Menstrual disorder |
|
- |
3 (15.8%) |
- |
- |
- |
- |
1 (5.9%) |
1 (3%) |
5 (11.4%) |
Sense of abdominal firmness and mass |
|
- |
2 (10.5%) |
- |
- |
- |
- |
4 (23.5%) |
1 (3%) |
5 (11.4%) |
Ascites |
|
- |
- |
1 (20%) |
- |
- |
- |
2 (11.8%) |
1 (3%) |
4 (9.1%) |
Urinary |
|
- |
1 (5.3%) |
- |
- |
- |
- |
- |
4 (12.1%) |
3 (6.8%) |
Incidental detection (asymptomatic) |
|
- |
- |
- |
- |
- |
- |
2 (11.8%) |
4 (12.1%) |
2 (4.5%) |
Torsion |
|
- |
2 (10.5%) |
- |
- |
- |
- |
1 (5.9%) |
2 (6.1%) |
2 (4.5%) |
Nausea |
|
- |
1 (5.3%) |
- |
- |
- |
- |
1 (5.9%) |
- |
2 (4.5%) |
Hirsutism |
|
- |
1 (5.3%) |
- |
- |
- |
- |
1 (5.9%) |
- |
2 (4.5%) |
Loss of weight |
|
- |
1 (5.3%) |
- |
- |
- |
- |
1 (5.9%) |
3 (9.1%) |
1 (2.3%) |
Lack of appetite |
|
- |
1 (14.3%) |
- |
- |
- |
- |
3 (17.6%) |
2 (6.1%) |
1 (2.3%) |
Fever |
|
- |
- |
- |
- |
- |
- |
1(%5.9) |
- |
1 (2.3%) |
Hemoperitoneum |
Discussion
Ovarian cancer was already entitled “silent killer” since it was frequently recognized at the advanced stages (13). This delay can obviously impact the outcome and survival of the patients. Since MOGCTs generally affect young women, it would be so vital to be diagnosed quickly. We found out that at least 85% of the patients have had symptoms for a considerable time prior to diagnosis. This is in agreement with past reports showing that 89% and 97% of women in early and advanced stages were already symptomatic (9,14-16).
In our findings, the most common symptom at the initial visit was abdominal pain (acute and chronic). Other authors have also reported it at 55-80% (17,18). Although acute pain in our population was significantly more than other regions (41 vs. 10-25%) (19), many patients remembered that they have already had a kind of constitutional discomforts for a while. Our results revealed that acute pain was more prevalent in adolescents and young adults. It had no relationship with parity. Undifferentiated and mixed tumors were the most common subtypes showing acute abdomen which was not consistent with previous reports (20). Our dysgerminomas, similar to the past reports, were hardly associated with acute abdomen (21). Acute pain due to adnexal torsion was mostly seen in yolk sac and immature teratomas, while none of SCC. teratomas referred with adnexal torsion. Although benign teratomas were the most likely tumors to be twisted in literature (22,23), our malignant teratomas showed diverse behaviors in this regard.
Abdominal distention has been reported at 45-85% in different reports (17-19), and we found it at 45%. Mixed tumors were the most common types involved with abdominal distention which confirmed other reports (20). We found its peak at 20 which was decreased sharply after that. It can be attributed to limited bony skeleton of adolescents leading to fast extension of ovarian tumors into the abdomen (24). We found out that multiparas had less complaints of abdominal distention compared to nulliparas, although the difference was not significant.
Hormonal imbalance due to the secretions of human chorionic gonadotropin (HCG), estrogen or androgen from germ cell tumors can induce menstrual irregularity, hirsutism or precocious puberty (25,26). The incidence of menstrual irregularity in our cases was parallel to other surveys (14.7 vs. 16.9%) (17). It was more in adolescents and young adults, and interestingly, nulliparas were significantly more involved with menstrual irregularity. According to histology, dysgerminomas, immature teratomas and mixed tumors were the most in this regard. On the other hand, germ cell tumors may be discovered in adolescents with primary amenorrhea which warrants assessment of karyotype to detect dysgenetic gonads. Regarding the risk of malignancy in dysgenetic gonads, in 30-50% bilateral ovarectomy should be considered (27-29). We faced five cases of primary amenorrhea who owned 46 XY chromosomes, three of which had mixed tumors, and two cases had pure dysgerminomas.
Other symptoms and signs like urinary and gastrointestinal complaints, fever, low appetite and weight loss were very limited in the patients which is in agreement with the previous studies (17,25) Importantly, 9.2% of the cases were asymptomatic and detected incidentally (during ultrasonography for another problem). It was more common in immature teratomas. Asymptomatic cases were significantly more in multiparas and older women. It can be associated with limited pelvic capacity in adolescents which cause fast expansion of tumor into the abdomen and incidence of clinical manifestations (24).
Conclusion
Malignant ovarian germ cell tumors can represent nonspecific various symptoms which can differ in point of severity and duration according to histology, age and parity. Pain, abdominal distention and menstrual irregularity are the most common symptoms. Women over 20-25 years, and multiparas may be less symptomatic or even asymptomatic. These tumors can produce acute abdomen due to late diagnosis which is higher in adolescents. However, it should be considered that a considerable number of patients may be symptomatic for days to even months prior to the first approach. Education of different presentations of malignant ovarian germ cell tumors to target populations and also health providers can help to avoid late diagnosis of the disease and establish the life and fertility of many young women worldwide.
Ethical issues
(IR.TUMS JKHC.Rec.1396.4819).
Acknowledgements
Hereby, we extend our gratitude to all the patients for their cooperation. We would also like to thank the chief and staff of Vali-e-Asr Hospital in Tehran, Iran for assisting us in the data collection.
Conflict of Interest
The authors declare that they have no conflicts of interest.