Document Type : Original article
Abstract
Background: Mindfulness-Based Cognitive Therapy (MBCT) is a short-term and structured intervention approach that has a favorable research background. The aim of this study was to evaluate the effectiveness of MBCT on negative automatic thought, psychological symptoms, severity of pain and quality of life in female patients with fibromyalgia.
Methods: In a randomized controlled trial, from February to October 2021, 20 patients with fibromyalgia were selected using purposive sampling method and assigned into two experimental and control groups through block randomization. MBCT was presented to the participants in the experimental group in eight sessions and the control group was placed on a waiting list. Quality of Life Questionnaire (WHOQOL-BREF), Pain Intensity Questionnaire (PIS), Psychological Symptoms Questionnaire (anxiety, stress and depression) (DASS), and Automatic Negative Thoughts Questionnaire (QNS) were completed by the participants in two stages (pre-test and post-test). Data were analyzed using multivariate analysis of covariance in SPSS version 26.
Results: Preliminary results showed that MBCT had a significant effect on the severity of pain index and psychological symptoms (all’s <0.05). Secondary results also indicated that this therapeutic intervention was effective in reducing negative automatic thought and improving the quality of life (all’s<0.05).
Conclusion: Findings of this study in line with the research background showed the effectiveness of this therapeutic approach on psychological indices in female patients with fibromyalgia, although additional studies in this field are suggested.
Keywords: Anxiety, Female, Fibromyalgia, Mindfulness, Pain, Quality of life
Introduction
Fibromyalgia syndrome is a chronic musculoskeletal disease characterized by widespread pain and the presence of diffuse sensitive points in the absence of any inflammation or musculoskeletal abnormality (1,2). This syndrome is associated with symptoms such as fatigue, insomnia, morning stiffness, anxiety and depression, and cognitive deficits such as forgetfulness and difficulty in concentrating are seen in these patients (3). Fibromyalgia is also a debilitating syndrome that is related to diffuse and multifaceted musculoskeletal pain, the presence of multiple and unstable points sensitive to pain, sleep disturbance, and muscular flexibility (4). Pain is a common phenomenon in these patients and it has recently been identified that it plays an important role in their mental health and quality of life (5). Quality of life is one of the most important components of mental health and is examined in individual and social contexts (6,7). Many factors affect the quality of life in fibromyalgia patients, including severity of pain (8).
Disseminated body pain is a hallmark of the disease, which may be described by terms such as sharp and burning, throbbing, painful, blurred and deep, or tingling and numbness (8). Fibromyalgia syndrome is associated with high levels of psychological distress, including depression, anxiety, and stress (9). Research has also shown that attitudes and thoughts are an effective factor in pain tolerance (10). Accordingly, the range of psychological problems, chronic pain, as well as negative automatic thought can seriously affect the quality of life and adaptation process of a person with fibromyalgia. These problems have prompted psychologists and physicians to make extensive efforts to help fibromyalgia patients (11).
In this regard, a number of psychological interventions (12) including behavioral therapy, hypnotherapy, mindfulness and relaxation-based therapies can be named that have significant effects on physical and psychological symptoms of these patients (13,14). One of these programs is cognitive-consciousness-based behavior therapies (15) in which people learn to create the present moment consciousness instead of automatic guidance and new ways of responding to situations (16). Mindfulness means paying attention to specific and purposeful ways, in the present and free from judgment (17,18). Research has shown that Mindfulness-Based Cognitive Therapy (MBCT) can improve the quality of life and mood as an effective treatment program, and short-term training of this intervention reduces fatigue and anxiety and improves the quality of life (19).
Research has also proved the effectiveness of MBCT on improving patients’ quality of life (20-23). Also, many studies have been conducted on the effectiveness of MBCT on pain intensity, which shows the effectiveness of MBCT on pain intensity in different patients (24-27).
MBCT is a short-term and structured approach proposed by Teasdale et al (28). Some research suggests that MBCT has been used to improve the symptoms of anxiety, depression, and stress in a wide range of medical disorders (29-32). Another variable in this study is negative automatic thought. Dysfunctional attitudes, beliefs, and inflexible attitudes are extreme and resistant to changes that predispose a person to mental disorder (33,34). A large number of studies (31,35-37) have examined the effect of MBCT on negative automatic thought and it has been shown that this treatment causes patients to distance themselves from negative thoughts.
Based on the results of the previous research, effectiveness of MBCT, successful and standard intervention methods in correcting habits and improving and reducing the psychological problems have been considered in other groups, but very limited investigations have been conducted on their effectiveness among Fibromyalgia patients. No significant investigation has been implemented on the effectiveness of a positive approach on psychological problems.
Thus, there was a need to implement extensive measures in this field. In the present study, an attempt is made to investigate the effect of this intervention on various procedures in people with fibromyalgia. For this reason, with the application of the above treatment on these patients, it is hoped that the existing research gap in this field will be filled. As a result, this study seeks to answer the question of whether MBCT is effective on negative automatic thought, psychological symptoms, and pain intensity and quality of life in female patients with fibromyalgia.
Materials and Methods
Study design and participants
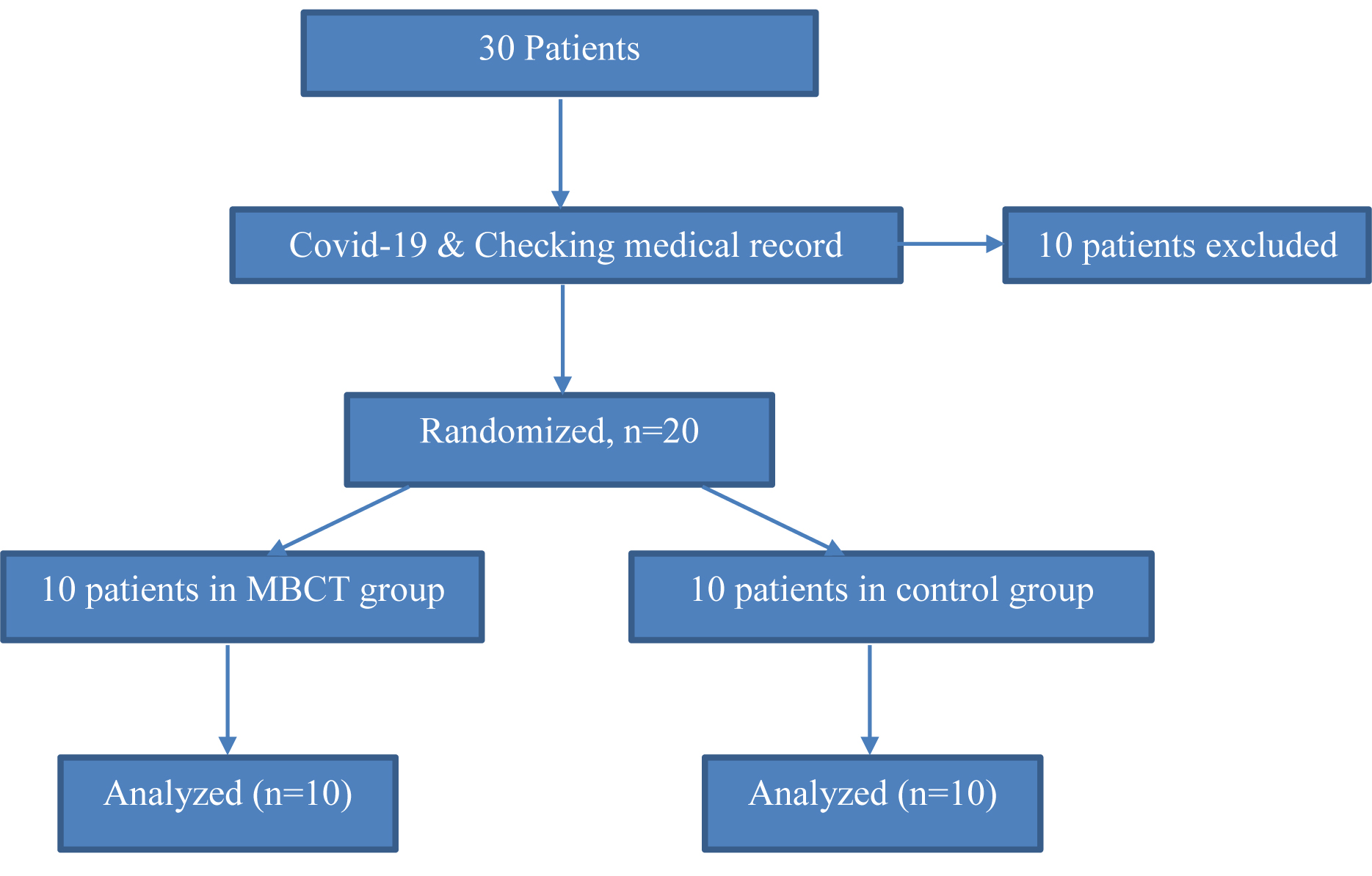
The present study was a randomized controlled trial conducted from February to October 2021 in Tehran. The statistical population of this study consisted of all individuals with fibromyalgia symptoms referred to clinics. From this population, 20 people were purposefully selected and assigned into two experimental groups (10 participants) and control (10 participants) using block randomization method (Figure 1). It should be noted that initially 30 people from this community were purposefully selected (15 people in each group), but due to the conditions of Covid-19 and some limitations, some patients withdrew from the project and 20 people for remained the intervention in the present study and they were divided into two experimental and control groups; the sample size was 20 people (each group included 10 people) and the questionnaires in the first session for the pre-test before the presentation of the treatment plan was answered by the subjects, Then, the treatment protocol, cognitive therapy based on mindfulness, which was developed by Segal et al (31), was implemented by the researcher on the subjects in 8 weekly sessions of one and a half hours. And once after the end of the therapeutic intervention, a post-test was taken from the subjects.
Entry criteria were:
1. Diagnosis of fibromyalgia based on the American College of Rheumatology (ACR) (classification criteria for diagnosing fibromyalgia are: diffuse pain that lasts for at least three months with tenderness that continues at least in 11 of the 18 points); 2. Obtaining the written consent to participate in the study, and 3. Not receiving any psychological intervention in the last 6 months (including drug therapy, counseling and psychotherapy interventions). Also, the exclusion criteria were:
1. Unwillingness to continue attending the intervention sessions; 2. Having a comorbid psychiatric disorder that needs immediate treatment (Major Psychiatric Disorders), and 3. Reporting any musculoskeletal pain outside the criteria of fibromyalgia (it should be noted that only people who met the criteria for the diagnosis of fibromyalgia and no other muscle pain unrelated to the disease should have participated in the intervention).
Data collection
A standard questionnaire was used to collect the data. Demographic data including age and education were asked via the questionnaire. Other questionnaires and treatment protocols are as follows:
World Health Organization Quality of Life-Brief (WHOQOL-BREF)
Quality of Life Questionnaire is a summary of WHOQOL-100 (1996). The Persian version of this questionnaire measures four areas of physical health, mental health, social relations and environmental health with 24 questions. The first two questions do not belong to any of the domains and assess the state of health and quality of life in general, thus this questionnaire has a total of 26 items (38). First, we have to give each of the 26 questions a score of 1 to 5. The World Health Organization has confirmed the validity and content of the instrument and its validity in different countries with Cronbach’s alpha method above 0.70. Nejat et al (38) in a study on 1167 participants examined the validity and reliability of the quality of life questionnaire. The reliability of the questionnaire was assessed using Cronbach’s alpha and correlation within the clusters obtained from the retest. Intra-cluster correlation and Cronbach’s alpha values were reported to be above 0.7 in all domains. Cronbach’s alpha obtained in the present study is 0.92.
Pain Intensity Survey (PIS)
This questionnaire was designed in 1992 by Vonkorff et al (39) to measure the severity of chronic pain. In this research, the Persian version of this questionnaire was utilized. The questionnaire consists of 7 items that rank the three axes of pain intensity, stability or duration of pain and the degree of disability resulting from pain in the form of an eleven-point scale of 0-10. In a study conducted by Smith et al (40) on the reliability and validity of this instrument, the internal reliability of the scale was 0.91 and the validity of all the questions was over 0.75 (40). Cronbach’s alpha was reported to be 0.87 and 0.68 for disability and pain intensity, respectively. In Shirazitehrani et al’s study (41), the reliability coefficient using Cronbach’s alpha for disability and pain intensity were 0.91 and 0.83, respectively. Cronbach’s alpha obtained in the present study is 0.82
Depression Anxiety Stress Questionnaire (DASS)
The Depression Anxiety Stress Questionnaire (DASS), developed by Lovibond and Lovibond (42) is a set of three self-reporting scales for assessing Negative Emotions in Depression, Anxiety and Stress. The application of this questionnaire is to measure the severity of the main symptoms of depression, anxiety and stress. In this research, the Persian version of this questionnaire was used.
Each of the subscales of this questionnaire is comprised of 7 items, the final score of each of which is obtained through the sum of the scores of the related questions. Each question is scored from zero (it does not apply to me at all) to 3 (it is absolutely true of me). Since DASS-21 is the abbreviated form of the original scale (42 questions), the final score of each of these subscales should be doubled (42). The results of calculating the correlation between factors in the study of Anthony et al (43) indicate a correlation coefficient of 0.48 between the two factors of depression and tension, a correlation coefficient of 0.53 between anxiety and tension, and a correlation coefficient of 0.53 between anxiety and tension. The correlation coefficient was 0.28 between anxiety and depression. The validity and reliability of this questionnaire in Iran have been examined by Samani and Jokar (44) that reported the retest validity for the Depression, Anxiety and Stress scales to be 0.80, 0.76 and 0.77, and Cronbach’s alpha for the Depression, Anxiety, and Stress scales were 0.81, 0.74, and 0.78, respectively. Cronbach’s alpha obtained in the present study is 0.76.
Automatic Negative Thought Questionnaire (QNS)
The Automatic Negative Thought Questionnaire was designed by Holon and Kendall (45) and has 30 items. In this research, the Persian version of this questionnaire was used. Its scoring is based on the Likert scale so that the options are never, sometimes, usually, often and always given a score of 1 to 5, respectively. The total score of each person is between 30 and 150. The Automatic Negative Thought Questionnaire measures four aspects of these automatic thoughts, including personal incompatibility and tendency to change, negative self-concept and negative expectations, low self-esteem, and helplessness. The validity of this questionnaire has very good internal stability (45). Holon and Kendall (45) reported Cronbach’s alpha of this questionnaire as 0.89. In research conducted by Nikkhah et al (36), the convergence validity of this questionnaire has been reported to be favorable. This researcher also obtained the reliability of the questionnaire using Cronbach’s alpha coefficient equal to 0.83. Cronbach’s alpha attained in the present study is 0.89.
Mindfulness-Based Cognitive Therapy (MBCT) Protocol
After the pre-test, the treatment method (MBCT) was presented in 8 sessions of one and a half hours per week, according to the protocol of the following 8 sessions (Table 1).
Table 1. Structure of MBCT group training sessions
|
Sessions |
Topics of each session |
|
Session 1 |
Establishing the initial communication, practicing physical examination, and focusing on daily activities |
|
Session 2 |
Exercises related to physical examination, presence of mind on the flow of breathing for 10 minutes, practicing the thoughts and feelings, explaining emotion and identifying positive and negative emotions, training to record desirable events, turning attention to daily activities with the presence of mind |
|
Session 3 |
Seeing and hearing meditation, meditation in a sitting position (presence of mind related to breathing and body), walking with presence of mind, practicing three-minute breathing space, recording undesirable events |
|
Session 4 |
Seeing and hearing meditation, meditation in a sitting position (awareness of breathing, body, sounds, and thoughts), definition of principles and rules governing emotion, regular three-minute breathing space, and three-minute confrontational breathing space |
|
Session 5 |
Sitting meditation (awareness of breathing, body parts, sounds and thoughts), and how to react to thoughts, feelings and bodily sensations, three minutes of regular and confrontational breathing space, reading the story of the king and his three sons and introducing the concept of acceptance |
|
Session 6 |
Meditation in a sitting position (becoming aware of breathing, body parts, sounds and thoughts), communicating with one’s thoughts and feelings, and developing them, and accepting unpleasant thoughts and emotions |
|
Session 7 |
Meditation in a sitting position (awareness of breathing, body parts, sounds and thoughts), awareness of the relationship between activity and mood, making a list of enjoyable activities and activities that create a sense of mastery in the person, and three minutes of regular breathing and confrontational space |
|
Session 8 |
Reflection on body examination, course review |
Ethical considerations
The study protocol was approved by the Ethics Committee of Arak University of Medical Sciences (Code: IR.IAU.ARAK.REC.1400.005). This project followed the ethical principles and national norms and standards for conducting the medical research in Iran. All personal data were protected and kept anonymous. Also, all stages of the study were performed after obtaining orally-informed consent from the patients.
Statistical analysis
Multivariate analysis of covariance was utilized to evaluate the effectiveness of the intervention. Examination of the assumptions of analysis of covariance showed that there was no outlier data among the values, the values of skewness and elongation of variables were in the range of +2 to -2 and was the evidence of normality of the data distribution. Homogeneity of variances with Levin test indicated that the significance level is over 0.05 and the assumption of homogeneity of variances was confirmed (p<0.05). In addition, the homogeneity test of regression slopes was performed by examining the interactive effect of the pretest with the group. All the effects were rejected and the assumption of homogeneity of regression slopes was confirmed (p<0.05). Box’s M test with the aim of examining the homogeneity of covariance matrices of variance showed that the mentioned hypothesis is confirmed (Box`s M=13.34, F=1.01 and p=0.435). The alpha error level for testing the hypotheses was considered 0.05 (p<0.05). The IBM SPSS v.26 was utilized to analyze the data.
Results
The results of the chi-square test represented that there is no significant difference in terms of demographic characteristics between the two groups (p<0.05) (Table 2).
Table 2. Demographic characteristics of the research sample
|
Variables |
Mindfulness |
Control |
Chi-square |
||
|
Frequency |
Percentage |
Frequency |
Frequency |
p-value |
|
|
Age |
|
|
|
|
0.984 |
|
˂30 |
4 |
40 |
3 |
30 |
|
|
30-50 |
3 |
30 |
4 |
40 |
|
|
50˃ |
3 |
30 |
3 |
30 |
|
|
Education |
|
|
|
|
|
|
Diploma˂ |
3 |
30 |
2 |
20 |
0.915 |
|
Diploma and associate |
3 |
30 |
5 |
50 |
|
|
Bachelor> |
4 |
40 |
3 |
30 |
|
Examination of the means showed that the mean pain intensity in the mindfulness group decreased by 24.20 points and in the control group, it increased by 0.50 points in the post-test. The mean of the psychological symptoms in the mindfulness group indicated a decrease of 21.20 points and in the control group, it decreased by 0.02 points. The mean of negative automatic thought in the mindfulness group showed a decrease of 25.50 points and in the control group out of 10, a decrease of 4.6 points. The average quality of life in the mindfulness group indicated an increase of 15.60 points and in the control group, it increased by 0.70 points (Table 3).
Table 3. Mean and standard deviation of the variables by groups and pre-test and post-test stages
|
Variables |
Group |
Pre-test |
Post-test |
||
|
Mean |
Std. deviation |
Mean |
Std deviation |
||
|
Severity of pain |
Mindfulness |
122.30 |
12.76 |
88.10 |
11.83 |
|
Control |
110.10 |
11.22 |
110.60 |
12.49 |
|
|
Psychological symptoms |
Mindfulness |
79.40 |
11.15 |
58.40 |
7.95 |
|
Control |
78.80 |
8.40 |
78.78 |
7.55 |
|
|
Negative automatic thought |
Mindfulness |
96.80 |
6.51 |
71.30 |
7.20 |
|
Control |
98.10 |
10.18 |
93.50 |
4.65 |
|
|
Quality of life |
Mindfulness |
67.50 |
6.36 |
83.10 |
6.84 |
|
Control |
67.00 |
5.60 |
67.70 |
5.89 |
|
Table 4 presents the results of analysis of covariance with the aim of investigating the effect of MBCT intervention on four research variables. The findings of table 3 showed that MBCT intervention had a significant effect on four variables of pain intensity, psychological symptoms, negative automatic thought and quality of life (p<0.05). According to the means reported in Table 3, it can be concluded that MBCT intervention has significantly reduced the severity of pain, psychological symptoms and negative automatic thought and also has improved and enhanced quality of life. The obtained effect size indicates that the MBCT intervention had the greatest effect on psychological symptoms with ETA share coefficient of 0.613 and on the quality of life with ETA share coefficient of 0.575.
Table 4. Results of multivariate analysis of covariance to evaluate the effectiveness of MBCT intervention
|
Variables |
Source |
Degree of freedom |
Sum of squares |
Mean of squares |
F- value |
p-value |
Effect size |
|
Severity of pain |
Group effect (intervention) |
1 |
2883.47 |
2883.47 |
58.49 |
<0.001 |
0.507 |
|
Error |
14 |
49.30 |
|
|
|
|
|
|
Psychological symptoms |
Group effect (intervention) |
1 |
2046.73 |
2046.73 |
146.93 |
<0.001 |
0.613 |
|
Error |
14 |
13.93 |
|
|
|
|
|
|
Negative automatic thought |
Group effect (intervention) |
1 |
2346.49 |
2346.49 |
59.22 |
<0.001 |
0.509 |
|
Error |
14 |
39.62 |
|
|
|
|
|
|
Quality of life |
Group effect (intervention) |
1 |
1095.88 |
1095.88 |
97.95 |
<0.001 |
0.575 |
|
Error |
14 |
11.19 |
|
|
|
|
p<0.001, F=78.11, Wilk’s Lambda= 0.034
Discussion
This study was conducted to evaluate the effectiveness of MBCT on negative automatic thought, psychological symptoms, pain intensity and quality of life in female patients with fibromyalgia. Preliminary findings showed that MBCT has a significant effect on pain intensity index and psychological symptoms. Secondary results also represented that this therapeutic intervention was effective in reducing negative automatic thought and improving the quality of life. These findings are consistent with the results of studies on the effectiveness of MBCT in the research background (5,24,46,47).
In explaining these results, it can be stated that patients with fibromyalgia show high levels of catastrophic pain. The study findings of Soleymani et al (46) and Pardos-Gascón et al (5) have been conducted to investigate the effect of MBCT on admission and pain intensity in patients with fibromyalgia, which showed mindfulness helps people to identify situations leading to discomfort and pain in them and get to know themselves better, identify their strengths and weaknesses, and then learn coping strategies to deal with these situations and thus develop the ability to control their anxious and worrying thoughts, and consequently their anxiety and pain intensity are steadily reduced (47).
Regarding the effectiveness of MBCT on the psychological symptoms of patients with fibromyalgia, these findings are consistent with the results (27-29,48-51). Mindfulness training teaches people how to break the habitual skills of the central motor from rigidity and prepare the ground for change by directing information processing resources toward attention goals such as breathing or the sense of the moment (27). Therefore, re-applying attention to this method prevents the increase or persistence of depression and rumination and makes defective processing cycles less accessible (48). MBCT offers a different way to deal with excitement and anxiety. Letting go of negative thoughts and not engaging in them prevents one from engaging in mental rumination. In mindfulness exercises, at any given moment, people realize the connection between thoughts, emotions and body sensations, and as a result of this awareness, depressive thoughts and moods are identified and with the practice of letting go and the acceptance of these thoughts, depression and psychological symptoms gradually reduce (49).
Regarding the effectiveness of MBCT on the negative automatic thought of patients with fibromyalgia, the results of the present study are consistent with conducted studies (31,35-37,52,53). MBCT is one of the most common methods for reducing negative automatic thought (52). In this method of treatment, the therapist performs a kind of cognitive reconstruction without directly involving the inactive thoughts of the subjects. Although the main purpose of mindfulness is not to calm down, non-judgmental observation of negative, internal, or physiological arousal events causes this condition and allows us to perceive events in the present less than they are distressing. When we are aware of the present time, our attention is no longer focused on the past or the future, while most psychological problems are due to focusing on the past (54) and this can reduce dysfunctional thoughts in patients. Therefore, it seems that mindfulness-based cognitive therapeutic exercises, by increasing people’s awareness of the present moment through techniques such as paying attention to breathing and body and paying attention to the here and now, affects cognitive system and information processing (31,53).
Regarding the effectiveness of MBCT on the quality of life, these findings are consistent with the results of previous studies (19-21,37,55). Based on these findings, it can be acknowledged that the reduction of activities, especially those that are socially enhanced and of value and importance to the patient, can lead to more social withdrawal, decreasing self-efficacy, increasing anxiety and depression, feelings disability as well as decrease in quality of life in these patients (20,55). Quality of life is significantly correlated with depressive stress, and as a result, it is expected that by performing regular mindfulness exercises, positive changes will be made in some psychological functions, such as reducing stress, increasing well-being, and mental health. As a result, these changes affect the quality of life of fibromyalgia patients (21).
In this study, as in other studies in the field of behavioral sciences and psychology, there were some limitations. The results of the present study are only associated with women with fibromyalgia living in Tehran and the generalizations to other settings are challenging and also, the limitation of the sample to people with medium and high social and economic level is another limitation of the present study. It is suggested that this research be conducted in other medical centers and on a larger sample so that the results are announced to counseling centers and hospitals for information and use. It is also suggested that the statistical research community be formed from different regions of the country. It is better to compare this treatment method with other psychiatric and pharmacological treatments in the future studies.
Conclusion
Cognitive-therapy based on mindfulness protocol was associated with reducing negative thoughts, psychological symptoms, pain intensity, and consequently improving the quality of life in female patients with fibromyalgia. According to this treatment protocol, relevant specialists can use the positive effect of this method as a complementary therapy along with drug treatments for fibromyalgia patients.
Acknowledgements
The authors thank the staff for their help. This article is extracted from the Ph.D dissertation by Dr. Naghmeh Shokouhi Nejad, Dr. Mohammad Reza Bayat as the corresponding author and the supervisor, Dr. Firoozeh Zangeneh Motlagh as the advisor on this project. This study obtained its ethical approval from the Research committee of Islamic Azad university Arak Branch code: IR. IAU. ARAK.REC.1400.005.
References